A preprint in 84 older adults with epilepsy found that abnormal Alzheimer's-related blood biomarkers were common, but the biomarker categories did not line up neatly with cognitive impairment.
Research Highlights
- Only 32.1% had normal biomarkers: 27 of 84 older adults with epilepsy were A−T−N− using blood-based amyloid, tau, and neurodegeneration markers.1
- AD-continuum profiles were common: 31 participants (36.9%) had amyloid-positive profiles, placing them on the Alzheimer's disease (AD) continuum under the AT(N) framework.
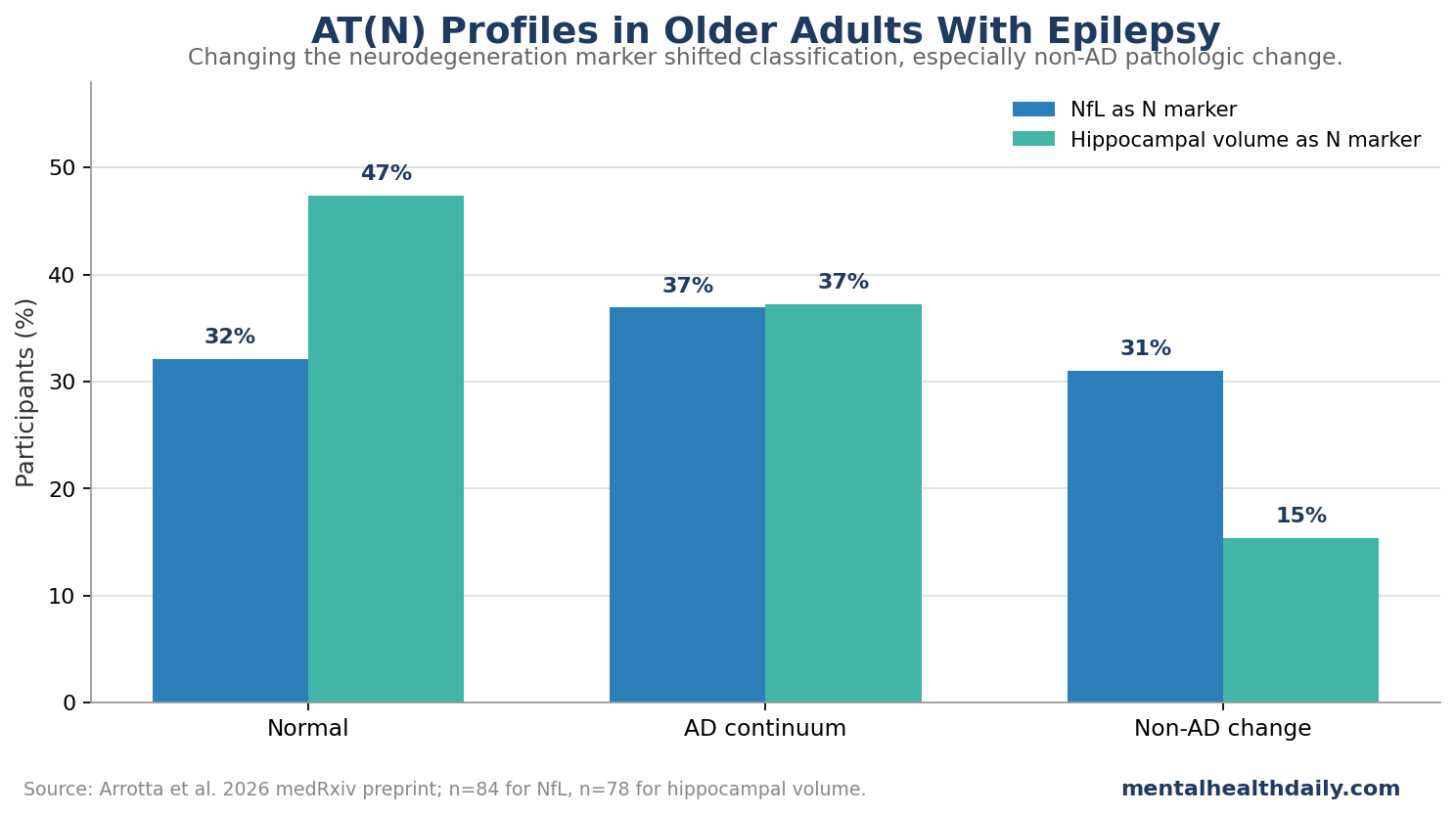
- Non-AD pathologic change depended on the N marker: using neurofilament light chain classified 31.0% as non-AD pathologic change, while substituting hippocampal volume lowered that to 15.4%.
- Early-onset epilepsy carried higher abnormal-biomarker odds: early-onset epilepsy had adjusted odds ratio (aOR) 8.84 for abnormal profiles vs. late-onset unexplained epilepsy, with higher NfL, higher p-tau217, and lower Aβ42/Aβ40.
- p-tau181 tracked memory better than AT(N) categories: categorical AT(N) profiles were not significantly associated with MoCA or IC-CoDE cognition, while p-tau181 was linked to worse delayed word-list recall in 84 participants.
AT(N) is the amyloid/tau/neurodegeneration framework, a research system that classifies Alzheimer's biology by amyloid burden, tau pathology, and neuronal injury or atrophy. It was built for Alzheimer's disease, but epilepsy complicates each part of the framework because seizures, antiseizure medications, hippocampal injury, and vascular risk can also affect cognition and brain-injury markers.
Arrotta et al. applied this framework to older adults with focal epilepsy from the Brain Aging and Cognition in Epilepsy study. The findings support cautious interpretation: blood biomarkers may detect risk-relevant biology while still requiring epilepsy-specific context.
84 Older Adults Had Plasma Amyloid, Tau, and NfL Measured
The 2026 medRxiv preprint included 93 participants with epilepsy, then excluded 9 because AT(N) data were missing. The final sample had 84 participants with mean age 66.3 years, 57.1% female sex, 85.7% white race, and average epilepsy-onset age 44.0 years.
The cohort was clinically mixed:
- Epilepsy duration: median 20 years, with interquartile range 5 to 37.5 years.
- Drug resistance: 52 participants (61.9%) met criteria for drug-resistant epilepsy.
- Epilepsy site: 41 participants (48.8%) had temporal lobe epilepsy.
- Recent seizures: only 3 participants had a seizure within 24 hours of blood draw.
- Cognition: mean Montreal Cognitive Assessment score was 24.6, and 27 participants (32.1%) met IC-CoDE criteria for cognitive impairment.
The researchers measured Aβ42/Aβ40, the amyloid-beta 42-to-40 ratio used as a blood-based amyloid marker; p-tau181 and p-tau217, phosphorylated tau markers linked to Alzheimer's biology; and neurofilament light chain (NfL), a blood marker of neuronal injury. They also tested hippocampal volume as an alternative neurodegeneration marker.
Normal Biomarkers Were Less Common Than AD-Continuum or Non-AD Change
Using NfL as the neurodegeneration marker, the blood-based AT(N) split was:
- Normal biomarkers: 27 of 84 participants (32.1%).
- AD continuum: 31 of 84 participants (36.9%), meaning an amyloid-positive profile.
- Non-AD pathologic change: 26 of 84 participants (31.0%), meaning tau-positive and/or neurodegeneration-positive without amyloid positivity.
Those proportions differ from what researchers have reported in cognitively unimpaired older adults, where normal profiles are often closer to 52-55% and AD-continuum profiles around 22-24%.15 The comparison is imperfect because cohorts, assays, and age distributions differ, but the epilepsy sample did not look like a biomarker-normal aging sample.
APOE-ε4, a genetic variant associated with higher Alzheimer's risk, also tracked the AD-continuum group. APOE-ε4 positivity was 35.5% in the AD-continuum group vs. 18.5% in the normal-biomarker group and 11.5% in the non-AD pathologic-change group.
Early-Onset Epilepsy Had Higher Abnormal-Biomarker Odds
The study compared early-onset epilepsy with late-onset unexplained epilepsy (LOUE; epilepsy beginning at age 55 or later without a clear cause). When the researchers collapsed AT(N) categories into normal vs. abnormal, early-onset epilepsy was associated with substantially higher abnormal-biomarker odds:
- aOR 8.84: adjusted odds ratio for abnormal biomarker profile in early-onset vs. late-onset unexplained epilepsy.
- 95% CI 2.35 to 41.89: the confidence interval, meaning the estimated effect was imprecise but remained above 1.
- p = 0.003: the association was statistically significant after adjustment for age, education, epilepsy side/site, and chronic kidney disease.
Individual biomarkers gave a more detailed pattern. Early-onset epilepsy was associated with higher NfL (B = 29.65, 95% CI 10.71 to 48.59, p = 0.003), higher p-tau217 (B = 1.30, 95% CI 0.33 to 2.28, p = 0.010), and lower Aβ42/Aβ40 ratio (B = −0.004, 95% CI −0.008 to −0.00003, p = 0.048). It was not significantly associated with p-tau181.
This does not prove seizures caused Alzheimer's pathology. Childhood-onset epilepsy has been linked to higher amyloid burden decades later,4 and late-onset epilepsy has been associated with amyloid markers in cohort data,2 but directionality remains hard to pin down. Epilepsy can reflect brain disease, contribute to network injury, or both.
NfL and Hippocampal Volume Classified Different People
The neurodegeneration part of AT(N) is especially difficult in epilepsy. NfL is sensitive to neuronal injury, but it is not specific to Alzheimer's disease. It can rise with seizure-related injury, inflammatory disease, trauma, and many neurologic disorders.6
Arrotta et al. tested this problem directly by replacing NfL with total hippocampal volume below the 25th percentile. The AD-continuum proportion barely changed, but the normal and non-AD groups shifted:
- Normal profile: 47.4% with hippocampal volume vs. 32.1% with NfL.
- AD continuum: 37.2% with hippocampal volume vs. 36.9% with NfL.
- Non-AD pathologic change: 15.4% with hippocampal volume vs. 31.0% with NfL.
- NfL vs. hippocampal volume: no significant correlation, Spearman r = −0.155, p = 0.174.
That is the most useful methodological result in the paper. If NfL labels twice as many people as non-AD pathologic change compared with hippocampal volume, clinicians and researchers should avoid treating the N category as a single stable construct in epilepsy.
AT(N) Categories Did Not Explain Cognition, but p-tau181 Tracked Memory
The categorical profiles did not significantly predict global cognition or cognitive classification. AT(N) group was not significantly associated with MoCA total score, IC-CoDE cognitive phenotype, IC-CoDE memory-domain impairment, or delayed word-list recall after adjustment.
Individual biomarkers were more informative than the categorical framework. Log-transformed p-tau181 was associated with lower Rey Auditory Verbal Learning Test delayed-recall T score in adjusted models (B = −5.59, 95% CI −10.31 to −0.86, p = 0.021). After removing 1 p-tau181 outlier, the estimated memory association strengthened to B = −7.58 (95% CI −13.77 to −1.39, p = 0.017).
That pattern fits prior temporal-lobe epilepsy work showing Alzheimer-like amyloid and tau alterations associated with cognitive deficit,3 and surgical tissue work linking hyperphosphorylated tau with cognitive decline in refractory epilepsy.7 It also shows why the full category can be less informative than a continuous biomarker when the sample is heterogeneous.
Epilepsy Biomarkers Need Epilepsy-Specific Interpretation
The strongest reading is not that every abnormal blood biomarker in epilepsy equals Alzheimer's disease. Blood biomarkers can reveal risk-relevant biology, but epilepsy adds several confounders:
- Seizure-related injury: NfL can reflect neuronal damage from recent or cumulative seizure activity.
- Temporal-lobe vulnerability: hippocampal and medial temporal structures are involved in both epilepsy and Alzheimer's-related memory networks.
- Medication burden: antiseizure medication count and sedating effects can affect cognition without being Alzheimer's pathology.
- Mixed mechanisms: amyloid, tau, vascular injury, hippocampal sclerosis, sleep, mood, and seizure burden may all contribute to cognitive impairment.
That is why the paper's method result is as important as its prevalence result. Applying AD-centric blood biomarkers to epilepsy may help identify people who need closer cognitive monitoring, but the framework probably needs multimodal support: serial biomarkers, MRI, seizure history, medication review, cognitive testing, and comparison against epilepsy-free aging cohorts.
Evidence-strength note: this was a cross-sectional preprint, so it can map biomarker patterns at one point in time but cannot show whether abnormal AT(N) status predicts future dementia.
The clinically useful interpretation is risk stratification, not diagnosis. A neurologist could treat an abnormal blood profile as a reason to look harder at cognition, seizures, medication effects, sleep, vascular risk, and MRI findings, while waiting for longitudinal data to show which biomarker combinations actually forecast decline in older adults with epilepsy.
Questions About Epilepsy and Alzheimer's Blood Biomarkers
Does an abnormal AT(N) profile mean an older adult with epilepsy has Alzheimer's disease?
No. AT(N) is a biological research framework, not a stand-alone clinical diagnosis. In epilepsy, abnormal biomarkers may reflect Alzheimer's-related pathology, seizure-related injury, mixed neurodegeneration, or several processes at once.
Which biomarker looked most connected to memory?
p-tau181 had the clearest memory association in this study. Higher p-tau181 was linked to worse delayed word-list recall after adjustment, while categorical AT(N) profiles were not significantly associated with memory classification or global cognition.
Why did NfL and hippocampal volume give different classifications?
NfL is a broad neuronal-injury marker. Hippocampal volume is a structural marker that may be more anatomically specific but can miss diffuse or early injury. In epilepsy, both can be affected by non-Alzheimer's mechanisms.
What should future studies do?
They need longitudinal follow-up. A single blood draw can show abnormality, but it cannot determine whether biomarkers predict future memory decline, dementia, seizure worsening, or response to treatment.
References
- AT(N) Framework in Older Adults with Epilepsy: Plasma Biomarkers and Associations with Demographic, Clinical, and Cognitive Features. Arrotta K et al. medRxiv. 2026. doi:10.64898/2026.04.24.26351489
- Association of Plasma Aβ42/Aβ40 Ratio and Late-Onset Epilepsy. Johnson EL et al. Neurology. 2023;101(13):e1319-e1327. doi:10.1212/WNL.0000000000207635
- Alzheimer-Like Amyloid and Tau Alterations Associated with Cognitive Deficit in Temporal Lobe Epilepsy. Gourmaud S et al. Brain. 2020;143(1):191-209. doi:10.1093/brain/awz381
- Association Between Childhood-Onset Epilepsy and Amyloid Burden 5 Decades Later. Joutsa J et al. JAMA Neurology. 2017;74(5):583-590. doi:10.1001/jamaneurol.2016.6091
- Age-Specific and Sex-Specific Prevalence of Cerebral β-Amyloidosis, Tauopathy, and Neurodegeneration in Cognitively Unimpaired Individuals Aged 50-95 Years. Jack CR et al. Lancet Neurology. 2017;16(6):435-444. doi:10.1016/S1474-4422(17)30077-7
- Blood Neurofilament Light: A Critical Review of Its Application to Neurologic Disease. Barro C et al. Annals of Clinical and Translational Neurology. 2020;7(12):2508-2523. doi:10.1002/acn3.51234
- Hyperphosphorylated Tau in Patients with Refractory Epilepsy Correlates with Cognitive Decline: A Study of Temporal Lobe Resections. Tai XY et al. Brain. 2016;139(Pt 9):2441-2455. doi:10.1093/brain/aww187