Sleep problems during chemotherapy include more than daytime fatigue. In a 2026 outpatient chemotherapy sample, 87% reported poor sleep quality and 61% had variable sleep timing, while measured bedroom light, temperature, and self-reported environmental disruption were not significantly linked to overall sleep health.1
Research Highlights
- Small chemotherapy sample: Adams et al. studied 23 adults receiving outpatient chemotherapy who already reported poor sleep quality or insomnia symptoms.1
- Sleep quality dominated: 87% rated sleep as fairly bad or very bad, making subjective quality the most common sleep-health problem in the cohort.1
- Sleep timing was also unstable: 61% had variable timing, and actigraphy showed average sleep duration of 6 hours 57 minutes with 58 minutes awake after sleep onset.1
- Bedroom environment did not explain much: Sleep environment scores, measured light, and measured temperature had no significant association with overall or domain-specific sleep health.1
- Broader cancer literature agrees on burden: Meta-analytic and symptom-cluster work links sleep disturbance in cancer with fatigue, pain, anxiety, depressive symptoms, and poorer quality of life.2,3
The grounded takeaway: bedroom environment can still matter, but in this small chemotherapy group the biggest measurable sleep problems were quality and timing, while obvious light or temperature exposure did not explain overall sleep health.
Adams 2026 Measured 7 Sleep-Health Domains During Chemotherapy
Adams et al. recruited 23 adults diagnosed with cancer in the prior 6 months and receiving outpatient chemotherapy in Western Australia.1
- Sample size: 23 chemotherapy outpatients with sleep complaints.
- Age and sex: mean age 54.1; 78% female.
- Cancer mix: 14 of 23 participants had breast cancer; stage II disease was most common.
- Treatment setting: outpatient chemotherapy, mostly neoadjuvant treatment with fewer adjuvant cases.
The study used a multidimensional sleep-health framework rather than a single insomnia score. Sleep health included duration, continuity, timing, regularity, rhythmicity, daytime sleepiness or alertness, and subjective quality. Measurements came from sleep questionnaires, wrist actigraphy, and a bedside temperature/light logger.
Cancer sleep disturbance is usually discussed as insomnia, but insomnia is only one piece of the sleep-health picture. A person can spend enough time in bed and still have unstable timing, fragmented sleep, poor perceived quality, or daytime impairment.
Intervention choice depends on the dominant sleep-health domain. A patient whose main problem is irregular timing needs a different plan from a patient waking repeatedly from pain, nocturia, steroid activation, or hot flashes. The old generic sleep-hygiene script tends to flatten those distinctions; a domain-by-domain sleep-health check keeps the problem specific enough to treat.
Poor Sleep Quality and Variable Timing Were the Main Problems
The results were clear: quality and timing were worse than duration or sleepiness. 87% rated their sleep as fairly bad or very bad. 61% had variable sleep timing. Average sleep duration was 417 minutes, or 6 hours 57 minutes, just under the National Sleep Foundation adult recommendation of 7–9 hours.1,8
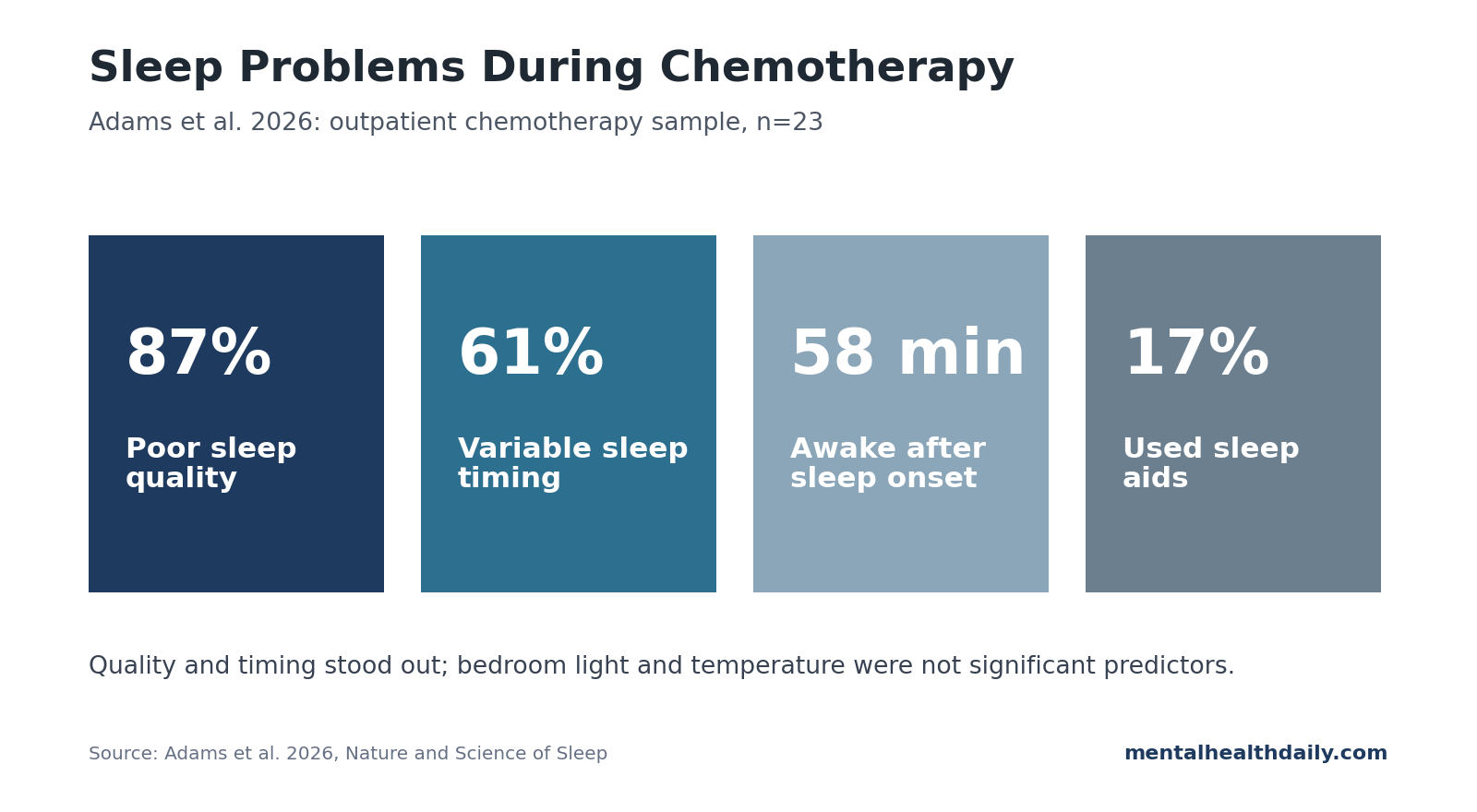
Sleep continuity was also not great. Participants averaged 58 minutes of wake after sleep onset, well above the 20–30 minute range usually considered better sleep continuity. Daytime sleepiness was less abnormal, with mean Epworth Sleepiness Scale score below the clinical threshold of 10.1
Someone can avoid severe daytime sleepiness and still have sleep that feels bad, shifts around the clock, and fragments through the night. Chemotherapy sleep management should therefore ask about timing, continuity, and “how many hours did you sleep?”
Bedroom Light and Temperature Were Not the Main Explanation
The environmental data were narrower than expected.
- Bedroom temperature: average sleep-period temperature was 23°C, with observed values ranging from 16°C to 28°C.
- Light exposure: generally low, with about 10 minutes above 10 lux during sleep periods.
- Environment scores: disruptive sleep environment factors were not common overall.
Despite measuring both subjective and objective environment variables, the researchers found no significant association between sleep environment factors and overall sleep health or individual sleep-health domains. That should not be overread: the study had only 23 participants, so absence of statistical significance is not proof that environment is irrelevant.
Still, the finding keeps the interpretation grounded. For chemotherapy patients already dealing with nausea, pain, steroid exposure, anxiety, fatigue, hot flashes, and disrupted routines, changing the bedroom alone may be too weak an intervention unless the environment is clearly bad.
The strongest environmental interpretation is therefore conditional. If the room is hot, bright, noisy, crowded, or unsafe, the fix is obvious and low-risk. If the room is already quiet, dark, and reasonably cool, the chemotherapy sleep problem probably lives elsewhere: treatment timing, symptom control, conditioned arousal, daytime inactivity, or anxiety around the next cycle.
Cancer Sleep Disturbance Usually Clusters With Fatigue and Mood Symptoms
The broader oncology literature makes the Adams result more plausible. A 2022 systematic review and meta-analysis estimated high sleep-disturbance prevalence across cancer samples, and chemotherapy cohorts repeatedly show sleep disturbance clustering with fatigue, pain, anxiety, depressive symptoms, cognitive complaints, and poorer quality of life.2,3,4
Sleep sits inside this symptom loop. Sleep disruption can amplify pain sensitivity, fatigue, mood instability, and treatment burden. A single environmental fix is unlikely to normalize sleep when the driver is a treatment-symptom cycle more than a noisy bedroom.
The practical approach is multidomain: ask about insomnia symptoms, sleep timing, wake after sleep onset, naps, steroid timing, pain control, nausea, anxiety, and bedroom conditions. If the bedroom is bright, hot, noisy, or unsafe, fix it. If the bedroom is already reasonable, the next step is behavioral and symptom-targeted sleep care.
A sleep-health framework keeps the clinical conversation from collapsing into vague sleep hygiene advice.
- Drifting sleep timing: stronger morning light exposure and a more regular wake time may be the first target.
- Long nocturnal awakenings: insomnia-focused behavioral treatment may fit better than generic sleep hygiene.
- Medication-linked disruption: sleep disruption after dexamethasone or antiemetic dosing may need medication-timing review.
These are different problems, even when all of them get described as “bad sleep.”
Environment still belongs in the checklist, especially because light, temperature, noise, bed partners, and perceived safety are modifiable. The Adams data simply suggest that, in this small sample, environment was not the obvious first-order driver or the best standalone treatment target.
Limitations of This Chemotherapy Sleep Analysis
- Sample size was tiny. With 23 participants, regression models had little power to detect environment-sleep associations unless effects were large.
- The design was cross-sectional. Sleep and environment were measured in the same window, so the study cannot show whether sleep changes followed chemotherapy, environment, symptoms, or pre-existing insomnia.
- The cohort was selected for sleep complaints. Findings do not estimate sleep disturbance prevalence among all chemotherapy patients; they describe sleep-health domains among patients already reporting poor sleep or insomnia symptoms.
- Cancer types were uneven. Breast cancer dominated the sample, so results may not generalize to hematologic cancers, advanced disease, or inpatient chemotherapy.
Sleep Care During Chemotherapy Should Start With Timing and Quality
The Adams study supports a practical hierarchy. First, identify the dominant sleep-health domain: quality, timing, continuity, duration, sleepiness, regularity, or rhythmicity. Second, identify obvious medical and treatment drivers. Third, clean up the bedroom environment when it is clearly disruptive, but do not assume environment is the main cause.
For many chemotherapy patients, the strongest first questions are concrete:
- Sleep quality: Does sleep feel restorative, or does it feel light, broken, and unrefreshing?
- Sleep timing: Is bedtime or wake time drifting across the week?
- Continuity: How long are awakenings after sleep onset?
- Treatment timing: Are steroids, antiemetics, pain medication, caffeine, or daytime naps pushing the sleep window around?
That approach is more specific than treating chemotherapy insomnia as a generic bedroom-hygiene problem.
It also gives patients a more realistic target. The goal during chemotherapy may not be perfect sleep.
A more specific goal is identifying the 1 or 2 domains most responsible for next-day fatigue and then intervening there, whether that means regularizing wake time, treating nausea earlier in the evening, reducing long naps, or using CBT-I (cognitive behavioral therapy for insomnia) before adding another sedative.
Questions About Sleep Problems During Chemotherapy
Does chemotherapy directly cause insomnia?
Sometimes, but the pathway is usually mixed. Steroids, nausea, pain, anxiety, hot flashes, fatigue, inflammation, daytime napping, and hospital routines can all disrupt sleep during treatment.
The sleep-health domain keeps the symptom label specific. “Insomnia during chemotherapy” can mean trouble falling asleep, repeated awakenings, unstable timing, short sleep duration, or sleep that feels non-restorative despite enough hours in bed.
Is sleep quality more important than sleep duration?
Both matter. In this cohort, duration was only slightly below the recommended range, while perceived sleep quality and timing variability were much more common problems.
Should chemotherapy patients change bedroom temperature or lighting?
Yes if the room is hot, bright, noisy, or unsafe. But Adams 2026 did not find measured light, temperature, or environment scores to be significant predictors of sleep health in this small sample.
So the bedroom is worth checking, not worshipping. Fix obvious problems, then move quickly to treatment symptoms, sleep timing, and insomnia behavior if the environment already looks reasonable.
What treatment has the best evidence for cancer-related insomnia?
Cognitive behavioral therapy for insomnia (CBT-I) has the strongest non-drug evidence. Medication can be useful short term, but long-term hypnotic use needs periodic reassessment, especially in older or medically fragile patients.
References
- Adams S, Clay TD, Hasani A, Turner M, Cruickshank T. Multidimensional sleep health and sleep environment factors in individuals with cancer undergoing outpatient chemotherapy: an exploratory cross-sectional analysis. Nature and Science of Sleep. 2026;18:1567-1578. doi:10.2147/NSS.S572577
- Al Maqbali M, Al Sinani M, Alsayed A, Gleason AM. Prevalence of sleep disturbance in patients with cancer: a systematic review and meta-analysis. Clinical Nursing Research. 2022;31(6):1107-1123. doi:10.1177/10547738221092146
- Fox RS, Ancoli-Israel S, Roesch SC, et al. Sleep disturbance and cancer-related fatigue symptom cluster in breast cancer patients undergoing chemotherapy. Supportive Care in Cancer. 2020;28(2):845-855. doi:10.1007/s00520-019-04834-w
- Calvo-Schimmel A, Paul SM, Cooper BA, et al. Oncology outpatients with worse anxiety and sleep disturbance profiles are at increased risk for a higher symptom burden and poorer quality of life. Cancer Nursing. 2023;46(6):417-431. doi:10.1097/NCC.0000000000001139
- Billings ME, Hale L, Johnson DA. Physical and social environment relationship with sleep health and disorders. Chest. 2020;157(5):1304-1312. doi:10.1016/j.chest.2019.12.002
- Caddick ZA, Gregory K, Arsintescu L, Flynn-Evans EE. A review of the environmental parameters necessary for an optimal sleep environment. Building and Environment. 2018;132:11-20. doi:10.1016/j.buildenv.2018.01.020
- Buysse DJ. Sleep health: can we define it? Does it matter? Sleep. 2014;37(1):9-17. doi:10.5665/sleep.3298
- Hirshkowitz M, Whiton K, Albert SM, et al. National Sleep Foundation’s updated sleep duration recommendations. Sleep Health. 2015;1(4):233-243. doi:10.1016/j.sleh.2015.10.004