A 2026 ENIGMA structural MRI preprint involving 3,958 people diagnosed with schizophrenia and 5,489 controls found 2 cortical-alteration subtypes rather than 1 uniform brain pattern.1 The result maps heterogeneity: anterior-cingulate and temporoparietal network patterns may separate patients, but the result is not a diagnostic MRI test.
Research Highlights
- Large MRI base: The analysis included 3,958 schizophrenia patients and 5,489 neurotypical controls across ENIGMA-style multisite datasets.1
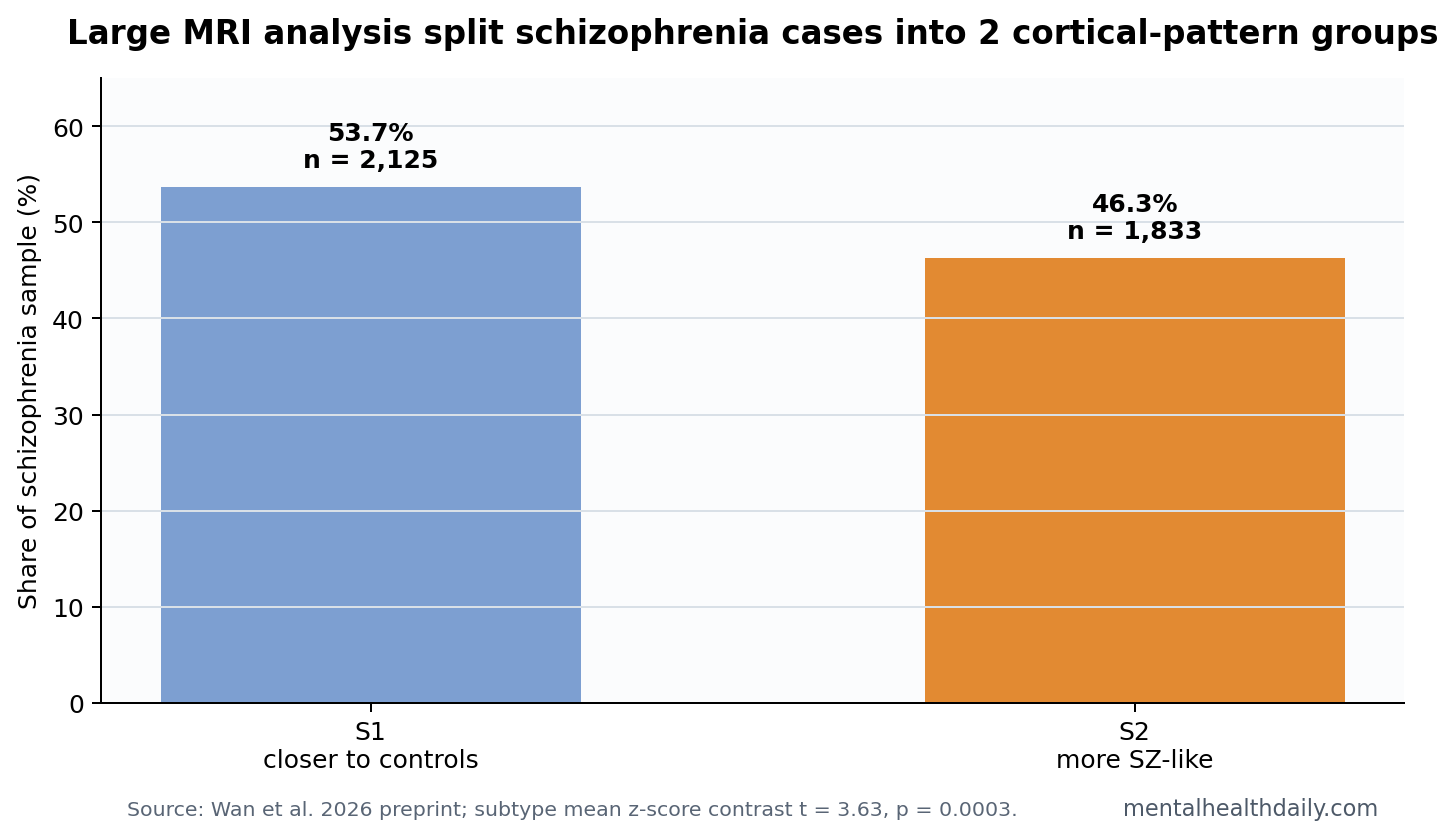
- 2 patient patterns emerged: Subtype S1 included 2,125 patients, or 53.7%, while S2 included 1,833 patients, or 46.3%.1
- Subtype separation was measurable: Mean z-scores differed between S1 and S2, t = 3.63, p = 0.0003, with S2 showing a more schizophrenia-like cortical profile.1
- Symptoms tracked topology: A partial least squares brain-symptom model was robust at P bootstrap < 0.001, and disorganization symptoms were most linked to topology changes.1
- Clinical use is not ready: A 2026 preprint can guide hypothesis-building, but it cannot make individual MRI classification safe.
Cortical gradients are smooth maps of how cortical regions vary from sensory areas to higher-order association cortex. In schizophrenia research, they offer a way to describe brain organization without pretending every region is an isolated island.
Network topology describes how brain regions are connected as a system: hubs, path length, clustering, and small-world organization. The Wan analysis used those tools to ask whether schizophrenia alters cortical organization in one average way or several separable ways.
3,958 Schizophrenia MRI Scans Did Not Collapse Into 1 Pattern
The study’s size is the main reason it deserves attention. Small neuroimaging studies can find striking maps that disappear when scanner, site, medication, age, and illness-duration variation hit the model. Here, the researchers used a multisite structural MRI pool large enough to test whether cortical-gradient and topology changes were broad, stable, and symptom-linked.
The case-control result followed familiar schizophrenia MRI territory: widespread cortical alteration along inferior-superior and frontal-temporal axes, with topology differences around hubs such as the insula and anterior cingulate cortex. Anterior cingulate cortex means a medial frontal region involved in conflict monitoring, motivation, and cognitive control; insula means a folded cortical region tied to interoception, salience, and body-state integration.
Those regions fit older schizophrenia imaging work, but the subtype analysis is the more useful piece. Instead of treating every patient as a diluted version of the same average map, the researchers clustered cortical alteration patterns and found 2 groups.
Older ENIGMA analyses established the large-average frame: schizophrenia is associated with thinner cortex across many regions, with some of the largest effects in frontal and temporal areas.2 The average map is still useful because it shows that the disorder has reproducible brain-level correlates across large samples.
The limitation of the average map is clinical interpretation. A group mean can be statistically powerful while still hiding different patient profiles. If 1 patient has a more salience-network-centered pattern and another has a more posterior association-cortex pattern, averaging both can produce a map that describes neither person especially well.
S1 Was Closer to Controls, While S2 Looked More Schizophrenia-Like
S1 included 2,125 patients, or 53.7% of the schizophrenia sample. S2 included 1,833 patients, or 46.3%. S2 showed the more schizophrenia-like cortical profile, while S1 stayed closer to controls. The group contrast was measurable: subtype mean z-scores differed, t = 3.63, p = 0.0003.1
What the split can support: schizophrenia is probably not one cortical anatomy pattern. The same diagnosis can contain more anterior-cingulate-centered and more temporoparietal/posterior-centered alteration profiles.
What the split cannot support: a clinician should not read an individual MRI scan and assign a patient to S1 or S2. The result still needs external validation, test-retest reliability, scanner robustness, and prospective clinical prediction before it becomes a tool.
The subtype split also needs symptom and course anchoring. A biologically meaningful subtype should eventually predict something outside the clustering algorithm: cognitive profile, disorganization severity, negative symptoms, functional decline, treatment response, relapse risk, or medication side-effect vulnerability. Without that bridge, the subtype labels remain mathematically clean but clinically thin.
That is why the symptom result is important, even though it is not enough by itself. A cortical-topology link to disorganization gives the map a behavioral handle. It suggests the subtypes may reflect different forms of distributed network disruption rather than scanner noise or arbitrary cluster boundaries.
Disorganization Symptoms Were the Strongest Symptom Link
The symptom result is narrower than a broad claim that MRI explains schizophrenia severity. Partial least squares modeling linked brain topology to symptom variation with P bootstrap < 0.001, and disorganization symptoms carried the strongest relationship.1
Disorganization symptoms include fragmented speech, disrupted goal-directed behavior, and difficulty maintaining coherent thought structure. A topology link is plausible because those symptoms depend on distributed communication across cognitive-control, salience, language, and association networks rather than one lesion-like site.
Prior ENIGMA work also found widespread cortical abnormalities in schizophrenia, but large averages do not automatically tell whether patients separate into biologically meaningful subgroups.2 Gradient methods add a second layer: they ask whether alterations respect the brain’s large-scale sensory-to-association organization.3
Gradient interpretation: a sensory-to-association gradient helps translate a long list of regions into a simpler organizational axis. If cortical differences fall along that axis, the result is easier to connect to cognition, language, salience, and self-referential processing than a scattered region table would be.
Topology interpretation: hub disruption is clinically plausible because schizophrenia symptoms often involve coordination failures across systems. Working memory, social inference, language coherence, and action planning depend on distributed communication. A hub-centered change can therefore look small in 1 region and still matter at the network level.
Preprint MRI Subtypes Need External Validation
Evidence-strength note: this is a preprint and a group-level neuroimaging subtype analysis. It can show reproducible-looking patterns inside a large dataset. It cannot prove that subtypes are stable within a person, predict treatment response, or distinguish schizophrenia from bipolar disorder, trauma-related psychosis, substance-associated psychosis, or neurodevelopmental conditions.
Medication exposure is another live issue. Antipsychotic treatment, illness duration, age of onset, smoking, metabolic health, and scanner protocol can all shape cortical thickness. Large multisite samples reduce some noise, but they do not erase those interpretive limits.
The practical value is therefore research triage. If S1 and S2 replicate, future studies can ask whether they differ in cognition, disorganization, inflammation, dopamine imaging, genetic loading, or treatment response. Without that next step, the subtypes remain a map of cortical heterogeneity rather than a clinical category.
Replication should also test whether the same subtype labels appear in first-episode psychosis, chronic schizophrenia, treatment-resistant schizophrenia, and high-risk cohorts. A subtype that appears only after years of illness or medication exposure would mean something different from a subtype detectable near onset.
The most useful future design would combine structural MRI with symptom ratings, cognitive testing, medication history, and longitudinal outcomes. That would show whether cortical-gradient subtypes explain real course differences or simply summarize anatomy at 1 point in time.
A second validation step should compare schizophrenia subtypes with other psychiatric groups. Bipolar disorder with psychosis, schizoaffective presentations, trauma-related psychosis, and substance-associated psychosis can share symptoms while differing in course and treatment. A subtype that separates schizophrenia from controls but fails against those neighboring groups would remain scientifically interesting but clinically weak.
This is also where symptom-linked topology has to prove more than visual elegance. If the disorganization link holds, the next test is whether S1 and S2 separate people by speech coherence, functional outcome, medication response, relapse pattern, or cognitive-control impairment. A subtype that only redraws MRI anatomy is a research map. A subtype that predicts a clinical trajectory becomes a candidate stratification tool.
The same caution applies to the ENIGMA scale advantage. A 9,447-person MRI sample reduces the small-study problem, but large sample size does not automatically solve medication exposure, scanner harmonization, illness-stage differences, site effects, cohort composition, or cross-diagnosis specificity.
The best interpretation is therefore layered. The study strengthens the case that schizophrenia involves large-scale cortical-network organization, especially around salience and association systems. It also shows why 1 average case-control map is too blunt for a heterogeneous diagnosis. The next question is whether those maps predict outcomes that change care.
Until then, the safest clinical stance is curiosity without overuse. MRI subtypes can guide research conversations about disorganization and network hubs, while routine care still depends on symptoms, function, longitudinal course, medication response, side effects, and patient goals.
Questions About Schizophrenia MRI Subtypes
Does this mean schizophrenia can be diagnosed by MRI?
No. The study found group-level cortical-gradient and topology patterns. Diagnosis still depends on clinical history, symptoms, course, exclusions, and functioning.
Why does the anterior cingulate cortex matter here?
The anterior cingulate cortex sits at the intersection of salience, cognitive control, motivation, and conflict monitoring. Changes there are biologically plausible for disorganization and cognitive-control symptoms, but they are not specific to schizophrenia.
What would make the subtype claim clinically stronger?
Replication in independent cohorts, stability across scanners, prediction of outcomes, and treatment-response differences would move the result from descriptive neuroscience toward clinical usefulness.
References
- Wan L, et al. Individualized cortical gradient and network topological alterations in schizophrenia. medRxiv. 2026. doi:10.64898/2026.04.25.26351736
- van Erp TGM, et al. Cortical brain abnormalities in 4474 individuals with schizophrenia and 5098 control subjects via the ENIGMA consortium. Biological Psychiatry. 2018. doi:10.1016/j.biopsych.2018.04.023
- Margulies DS, et al. Situating the default-mode network along a principal gradient of macroscale cortical organization. Proceedings of the National Academy of Sciences. 2016. doi:10.1073/pnas.1608282113
- Wolfers T, et al. Mapping the heterogeneous phenotype of schizophrenia and bipolar disorder using normative models. JAMA Psychiatry. 2018. doi:10.1001/jamapsychiatry.2017.2663