A 244-person functional MRI study found no significant evidence that ventral striatum activation during reward anticipation works as an endophenotype — a measurable trait used to connect inherited risk with diagnosed illness — for bipolar and psychotic disorders.
Research Highlights
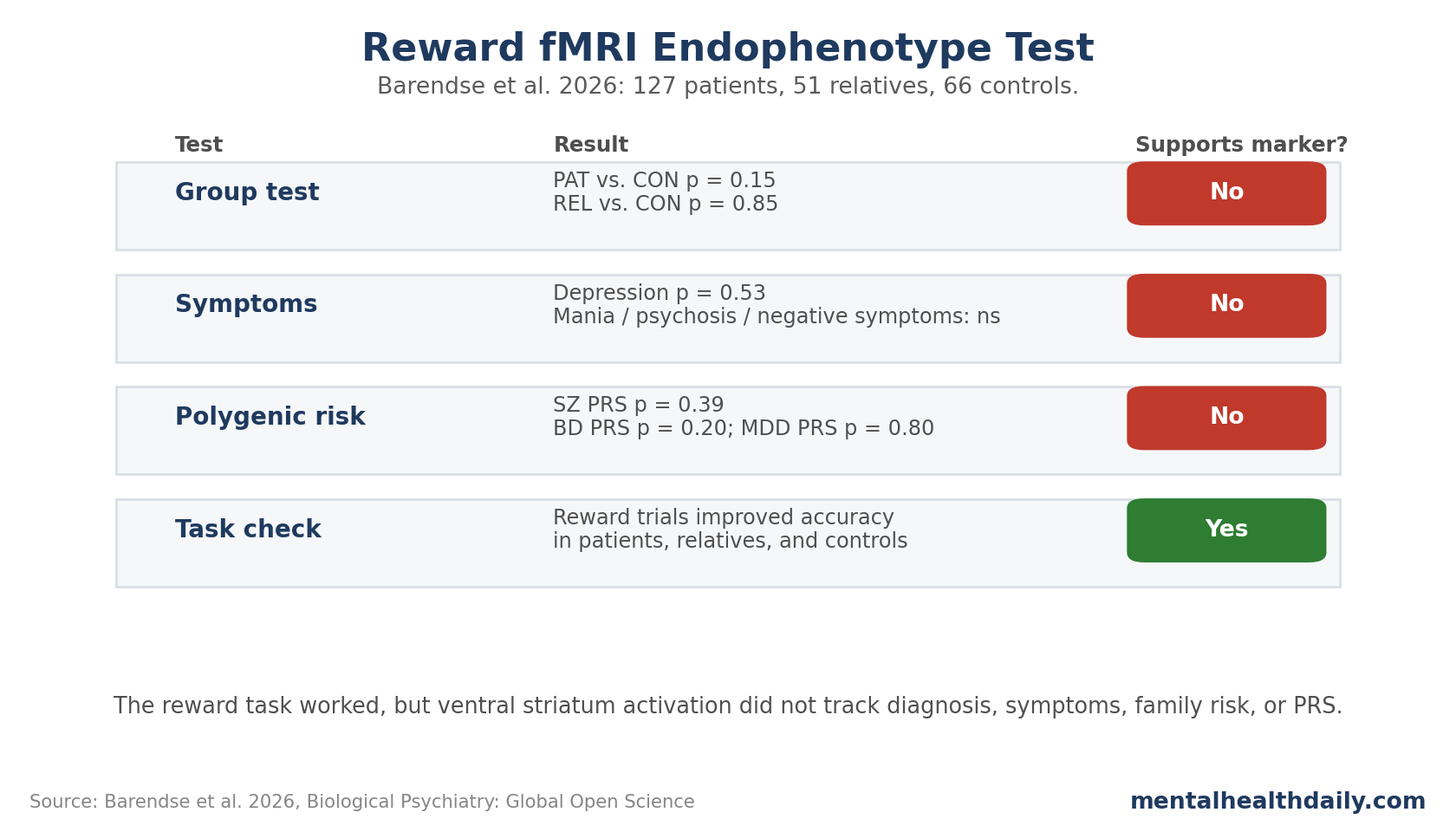
- The registered hypothesis failed: Barendse et al. found no significant ventral striatum reward-anticipation difference among 127 patients, 51 first-degree relatives, and 66 controls.1
- The task still worked behaviorally: all 3 groups responded more accurately on reward than neutral trials, but reward-related accuracy and reaction-time differences did not separate the groups.
- Symptoms did not explain the null: depressive symptoms (p = 0.53), manic symptoms (p = 0.49), positive psychotic symptoms (p = 0.99), and negative symptoms (p = 0.36) were not significantly related to ventral striatum activation during reward anticipation.
- Genetic-risk gradients were real but not neural: bipolar disorder PRS differed by group (F2,148 = 21.1), yet bipolar, schizophrenia, and depression PRSs were not significantly associated with ventral striatum activation.
- The result narrows biomarker claims: in this 244-person sample, reward circuitry remained relevant to psychosis, bipolar disorder, anhedonia, and motivation, but this fMRI marker did not behave like a stable familial-risk trait.
Researchers use endophenotypes in psychiatric genetics to test whether a measurable brain, cognitive, or biological trait helps connect genetic liability with clinical diagnoses. A useful endophenotype should be associated with illness, partly heritable, present even outside acute episodes, and more common in unaffected relatives than in the general population.6
Ventral striatum reward anticipation looked like a candidate because schizophrenia, bipolar disorder, depression, anhedonia, and negative symptoms have all been linked to reward-circuit alterations. This study tested whether that candidate survived a family-risk design.
That distinction is stricter than a standard patient-control imaging contrast. A brain response can differ between diagnosed patients and controls because of current symptoms, medication exposure, illness duration, hospitalization history, task engagement, sleep, substance use, or scanner-era sampling. An endophenotype claim has to survive a harder test: the marker should appear in a pattern that points toward inherited liability rather than only illness state.
Unaffected first-degree relatives are central to that test. They share more genetic and family-background risk with patients than unrelated controls, but they do not carry the same diagnostic state. If ventral striatum reward anticipation were a strong bipolar-psychosis endophenotype, relatives would be expected to show at least a partial shift toward the patient pattern. Barendse et al. instead found no significant patient-control difference and no intermediate relative pattern.1
244 Participants Completed Reward fMRI Across the Mood-Psychosis Spectrum
Barendse et al. studied adults with bipolar or psychotic disorders, first-degree relatives without those diagnoses, and control participants. Participants completed the monetary incentive delay task during functional MRI (fMRI; a method that tracks blood-oxygen changes as a proxy for neural activity).
Study snapshot:
- Final fMRI sample: 244 participants after exclusions for nonresponses, motion, and artifacts.
- Groups: 127 patients, 51 first-degree relatives, and 66 controls.
- Patient diagnoses: 92 bipolar disorder type 1, 5 other bipolar disorder, 10 schizoaffective disorder, 3 delusional disorder, 2 brief psychotic disorder, and 14 schizophrenia.
- Mean age: 52.0 years in patients, 53.5 in relatives, and 52.3 in controls; group difference p = 0.74.
- Main outcome: ventral striatum activation during reward anticipation, averaged across left and right regions of interest.
The design tested 3 claims. First, patients should show lower ventral striatum activation than controls. Second, relatives should sit between patients and controls if the marker tracks familial liability. Third, polygenic risk scores (PRSs; genetic-risk summaries built from many variants) and current symptoms should relate to ventral striatum activation if the marker reflects inherited or state-linked risk.
Reward Anticipation Activated the Ventral Striatum, But Groups Did Not Separate
The monetary incentive delay task did what it was supposed to do. Participants in every group were more likely to press in time when reward was offered than during neutral trials: patients t126 = 6.14 (p < 0.001), relatives t50 = 4.75 (p < 0.001), and controls t65 = 3.25 (p = 0.002). Reward anticipation also elicited positive ventral striatum activation across the sample.
The group comparison was the problem for the endophenotype hypothesis. Ventral striatum activation during reward anticipation did not differ significantly:
- Patients vs. controls: b = 0.23, SE = 0.02, t = 1.46, p = 0.15.
- Relatives vs. controls: b = 0.04, SE = 0.03, t = 0.19, p = 0.85.
- After false-discovery-rate correction: all confirmatory p values were greater than 0.50.
This is not a weak trend in the expected direction. The relatives did not sit between patients and controls, and patients did not show the predicted lower ventral striatum response. The task moved the reward system, but not in a way that mapped onto diagnostic or familial-risk status.
Symptoms and Polygenic Risk Also Failed to Track the Signal
The researchers then tested whether reward activation behaved more like a symptom-state marker than a diagnosis marker. It did not. Depressive symptoms were not significantly related to ventral striatum activation during reward anticipation (b = −0.002; SE = 0.004; t = −0.63; p = 0.53), and the depression-by-group interaction was not significant.
Patient-only symptom models were also null:
- Mania symptoms: b = −0.004, SE = 0.006, t = −0.69, p = 0.49.
- Positive psychotic symptoms: b = −0.000, SE = 0.005, t = −0.008, p = 0.99.
- Negative symptoms: b = 0.004, SE = 0.004, t = 0.92, p = 0.36.
The genetic-risk analysis was especially useful because it showed a split between psychiatric genetic liability and this specific fMRI signal. Bipolar disorder PRS differed by group (F2,148 = 21.1; p < 0.001), and schizophrenia PRS differed by group (F2,148 = 8.5; p < 0.001). Major depressive disorder PRS did not (F2,148 = 0.24; p = 0.79).
Yet none of those PRSs was significantly related to ventral striatum reward-anticipation activation: schizophrenia PRS p = 0.39, bipolar disorder PRS p = 0.20, and major depression PRS p = 0.80. Substance-use and medication covariate checks did not change the pattern.
Ventral Striatum Null Result Narrows Earlier Reward-Circuit Claims
Earlier meta-analyses gave the hypothesis a real basis. Zeng et al. reported ventral striatum hypoactivation during reward anticipation in schizophrenia, and Long et al. reported altered reward-anticipation activation in bipolar disorder.45 Broader monetary-incentive-delay meta-analyses also confirm that ventral striatum, anterior insula, and ventromedial prefrontal regions reliably participate in reward and loss anticipation or outcomes.23
Barendse et al. did not erase that literature. It tested a narrower claim: whether one region-of-interest reward-anticipation response behaves like a familial, genetically anchored marker across bipolar and psychotic disorders.
That narrower claim did not hold here. Several interpretations remain plausible:
- State-dependent marker: ventral striatum blunting may appear mainly during acute episodes, higher negative-symptom burden, severe anhedonia, or poorer functioning.
- Medication and illness-history complexity: long illness duration and treatment exposure may blur simple patient-control differences, even if medication covariates did not explain the result here.
- Task-specific marker: the monetary incentive delay task captures one slice of reward processing, not reward learning, effort valuation, social reward, or real-world motivation.
- Diagnostic heterogeneity: the combined mood-psychosis group improves dimensional testing, but it can hide subtype-specific effects.
Limitations of This Reward fMRI Study
The sample was stable and relatively low-symptom. Patients were often high-functioning and not in acute psychotic or manic episodes. That protects consent and scanning quality, but it limits variance in symptoms that may matter most for reward blunting.
The patient group mixed diagnoses by design. A cross-diagnostic approach fits the endophenotype question, but it cannot answer whether one subgroup, such as active psychosis, bipolar depression, or schizophrenia with severe negative symptoms, has a stronger signal.
The study was powered for medium effects. The researchers stated they had enough power to detect medium effects, while earlier meta-analyses reported medium-to-large effects. Smaller, subgroup-specific, or state-dependent effects could still be missed.
Polygenic-risk scores are still blunt tools. PRSs capture statistical genetic liability, not specific dopaminergic, striatal, developmental, or medication-response pathways. A null PRS association does not prove genes play no role in reward circuitry.
Questions About Reward Brain Activation in Bipolar and Psychosis
Does this mean reward circuitry is normal in schizophrenia and bipolar disorder?
No. It means this study did not support ventral striatum reward-anticipation activation as a stable endophenotype across the tested mood-psychosis spectrum.
Reward circuitry can still be altered in specific states, symptoms, subgroups, task designs, or illness phases.
Why does the relative group matter?
Unaffected first-degree relatives help test familial liability. If a brain marker is an endophenotype, relatives often show an intermediate pattern between patients and controls. That did not happen here.
What should future studies test?
More symptomatic cross-diagnostic samples, explicit anhedonia and negative-symptom enrichment, longitudinal episode tracking, and reward tasks that measure effort, learning, prediction error, and social reward may be more informative than a single reward-anticipation contrast.
This 244-person family-risk functional MRI test argues against treating ventral striatum reward anticipation as a stable bipolar-psychosis endophenotype. Reward circuitry remains biologically relevant, but this marker did not track diagnosis, symptoms, family risk, or polygenic risk in this sample.
References
- Reward-Related Brain Function as an Endophenotype in the Mood-Psychosis Spectrum. Barendse MEA et al. Biological Psychiatry: Global Open Science. 2026;6:100692. doi:10.1016/j.bpsgos.2026.100692
- Shared and distinct neural activity during anticipation and outcome of win and loss: A meta-analysis of the monetary incentive delay task. Chen Y et al. NeuroImage. 2022;264:119764. doi:10.1016/j.neuroimage.2022.119764
- Brain activations associated with anticipation and delivery of monetary reward: A systematic review and meta-analysis of fMRI studies. Jauhar S et al. PLOS ONE. 2021;16:e0255292. doi:10.1371/journal.pone.0255292
- Neural substrates of reward anticipation and outcome in schizophrenia: a meta-analysis of fMRI findings in the monetary incentive delay task. Zeng J et al. Translational Psychiatry. 2022;12:448. doi:10.1038/s41398-022-02201-8
- Altered brain activation during reward anticipation in bipolar disorder. Long X et al. Translational Psychiatry. 2022;12:300. doi:10.1038/s41398-022-02075-w
- The Endophenotype Concept in Psychiatry: Etymology and Strategic Intentions. Gottesman II, Gould TD. American Journal of Psychiatry. 2003;160(4):636-645. doi:10.1176/appi.ajp.160.4.636