A 2026 rat and astrocyte study found that human umbilical cord mesenchymal stem cell exosomes given 6 hours after experimental intracerebral hemorrhage reduced pro-inflammatory signaling and improved neurological recovery scores through the PI3K/AKT/PKM2/H3K18la pathway.1 The result is a mechanistic preclinical signal, not an emergency treatment for human brain hemorrhage.
Research Highlights
- Exosomes were timed early: rats received 100 μg/200 μL hUCMSC exosomes by tail vein 6 hours after collagenase-induced intracerebral hemorrhage.1
- Astrocytes were modeled separately: primary astrocytes were exposed to 20 μM hemin and then treated with 20 μg/mL exosomes 6 hours later.1
- Inflammation shifted lower: TNF-α and IL-1β decreased, while the anti-inflammatory cytokine IL-10 increased.1
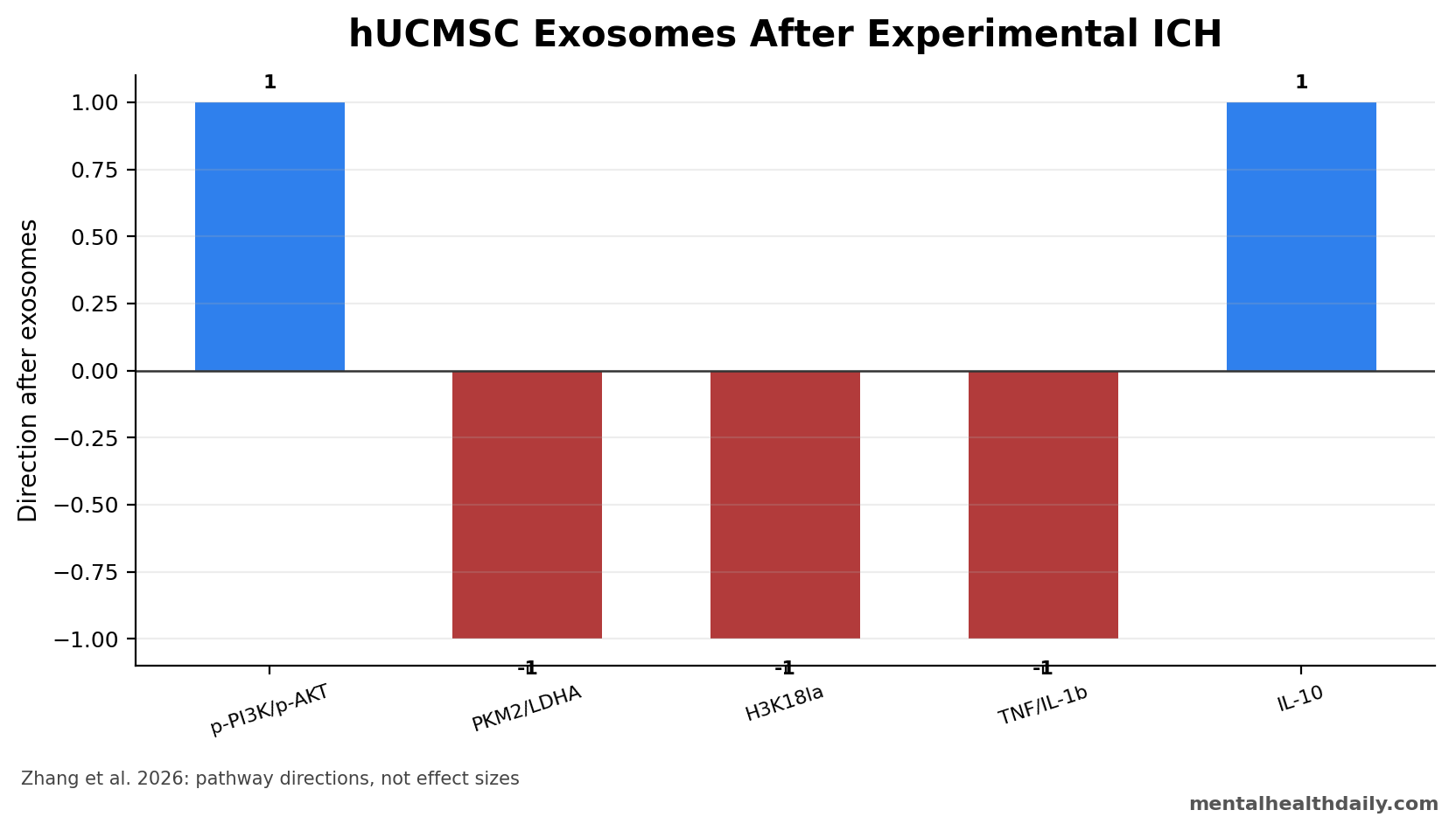
- Lactylation pathway changed: exosomes upregulated p-PI3K and p-AKT while downregulating PKM2, LDHA, and H3K18la.1
- Recovery was tracked 4 times: neurological function was assessed on days 1, 3, 7, and 14 after hemorrhage.1
Intracerebral hemorrhage (ICH) is bleeding into brain tissue. The primary hematoma causes direct injury, and secondary injury follows through edema, blood-brain barrier disruption, oxidative stress, and neuroinflammation.
Exosomes are small extracellular vesicles that cells release to carry proteins, lipids, and RNA-like signals. Human umbilical cord mesenchymal stem cell exosomes are being studied because they may deliver anti-inflammatory and tissue-repair signals without transplanting whole cells.
100 μg of Exosomes Was Given 6 Hours After Rat ICH
Zhang et al. induced ICH by stereotactically injecting collagenase IV into the rat striatum, a deep brain region involved in movement. At 6 hours after hemorrhage, rats received hUCMSC exosomes by tail vein at 100 μg/200 μL.1
The study also used a cell model. Primary astrocytes were exposed to 20 μM hemin, a blood-breakdown product that can trigger inflammatory injury, and then treated with 20 μg/mL exosomes 6 hours later.
Model pairing: the rat experiment tested whole-animal recovery after brain hemorrhage, while the astrocyte experiment tested whether the same pathway could be seen in a controlled cell-injury setting.
The timing is clinically interesting but still preclinical. A 6-hour post-ICH intervention sits after the initial bleed, when secondary injury is already developing, yet before inflammation and edema have fully evolved. That makes it a plausible rescue window in animals, but human ICH care has additional constraints: hematoma size, anticoagulant reversal, blood-pressure control, neurosurgical decisions, and rapid neurological deterioration all shape whether an experimental biologic could be delivered safely.
Why collagenase matters: collagenase models create bleeding by damaging the vessel-supporting matrix in the striatum. They are useful for studying hematoma-associated inflammation and neurological deficits, but they do not perfectly recreate spontaneous human hemorrhage. A treatment that improves collagenase ICH still needs confirmation in additional hemorrhage models before the signal can be treated as robust.
PKM2 Connected Glycolysis to Inflammatory Gene Signaling
The article’s mechanistic center is PKM2, a glycolysis-linked enzyme that can also influence inflammatory gene regulation. Under stress, PKM2 can shift from ordinary metabolic work toward nuclear signaling, where it helps sustain LDHA expression and inflammatory transcription. Zhang et al. framed PKM2 as a bridge between altered glucose metabolism and neuroinflammation after ICH.1
LDHA converts pyruvate toward lactate production. More lactate can then feed histone lactylation, including H3K18la, which changes how inflammatory genes are expressed. In plain English: the pathway links injured-cell metabolism to inflammatory gene activity, rather than treating inflammation as a separate immune-only process.
That is why the combined marker pattern matters more than any single band on a Western blot. Exosomes increased p-PI3K and p-AKT while reducing PKM2, LDHA, and H3K18la. The claimed pathway is therefore directional: hUCMSC exosomes appeared to dampen the glycolysis-lactylation loop that can amplify inflammatory signaling after blood-product injury.1
TNF-α and IL-1β Fell While IL-10 Rose
Inflammatory markers moved in the expected protective direction. TNF-α and IL-1β, two pro-inflammatory cytokines, decreased after exosome treatment. IL-10, an anti-inflammatory cytokine, increased.1
Lactylation is an epigenetic modification in which lactate-derived chemical marks can alter gene-expression regulation. In this study, the relevant mark was H3K18la, a histone lactylation signal tied to glycolysis and inflammatory gene expression.
The pathway result was coherent: exosomes increased phosphorylated PI3K and AKT, while lowering PKM2, LDHA, and H3K18la. PKM2 and LDHA are glycolysis-linked enzymes, so the authors interpreted the result as reduced pathological glycolysis-lactylation signaling.
Inflammatory cytokines gave the pathway a functional readout. TNF-α and IL-1β are pro-inflammatory cytokines that can worsen secondary brain injury by recruiting and activating immune responses. IL-10 is generally anti-inflammatory. Movement in all 3 markers toward lower inflammatory pressure makes the mechanism more coherent than a single isolated protein change.
Cargo remains unresolved: cytokine direction does not automatically identify the exact active material inside the exosomes. hUCMSC exosomes can carry microRNAs, proteins, lipids, and metabolic signals.
The paper supports a pathway-level effect on PI3K/AKT/PKM2/H3K18la signaling, but it does not reduce the therapy to one active ingredient.
Behavior Improved on Days 1, 3, 7, and 14
Neurological function was tested with corner turn, forelimb placement, Longa, and Bederson scores on days 1, 3, 7, and 14. These rodent scales capture asymmetry, limb placement, and neurological deficit after brain injury.1
The behavioral result is important because marker movement alone can be misleading. A pathway can look cleaner without improving function. Zhang et al. reported neurological recovery alongside inflammatory and lactylation-pathway changes.
Evidence-strength note: this was a rat and cell-model study. It can support a plausible mechanism and justify replication. It cannot establish human efficacy, treatment timing, dose, safety, product consistency, or interaction with standard ICH care.
Behavioral scoring also has to be read carefully. Corner-turn, forelimb-placement, Longa, and Bederson scores are useful neurological-deficit measures in rodents, but they are not patient-centered outcomes. Human trials would need outcomes such as death, functional independence, modified Rankin Scale, hematoma expansion, edema, intensive-care complications, and longer-term cognitive or motor disability.
Replication priorities: the next animal work should test whether the signal holds across sex, age, hemorrhage severity, delivery route, dose, and delayed treatment windows. A therapy that only works in young controlled rats 6 hours after a standardized striatal injury would be much weaker than one that survives those stress tests.
Human ICH studies would also need to separate anti-inflammatory benefit from bleeding risk. Any injected biologic given during acute hemorrhage has to avoid worsening coagulation, edema, infection risk, or hemodynamic instability. That safety question is separate from whether the pathway looks favorable in astrocytes.
Route of delivery is another unresolved point. Tail-vein injection is convenient in rats, but human brain delivery depends on circulation, blood-brain barrier permeability, particle clearance, and whether enough vesicles reach the injured perihematomal tissue during the relevant treatment window.
Exosome Therapy Still Has a Manufacturing Problem
Cell-free therapy sounds simpler than stem-cell transplantation, but exosomes are complex biological products. Their cargo depends on the parent cell source, culture conditions, isolation method, storage, and potency assay. Two exosome preparations can share the same broad label while carrying different microRNA, protein, and lipid profiles.
Emergency use requires consistency: a hospital cannot rely on a vague “umbilical cord exosome” category. It would need a reproducible product with defined release criteria, sterility controls, dose units, biodistribution data, and evidence that the intended anti-inflammatory pathway activates in the injured brain.
Practical implication: Zhang et al. strengthen the biological rationale for hUCMSC exosomes in ICH models, but the clinical development path runs through product standardization as much as through efficacy replication. Without a defined product, promising pathway biology is difficult to translate into a real emergency stroke intervention.
Human ICH Translation Would Need Functional Endpoints
Functional outcomes are the real test: clinical translation would need to prove that pathway changes matter to patient function. In human ICH, the practical question is whether treatment improves survival without severe disability, reduces edema or neurological deterioration, or increases the chance of independent daily function months later.
Cytokines, PKM2, LDHA, and H3K18la could become useful biomarkers, but they cannot replace functional outcomes.
Trial timing would be difficult. Many ICH patients arrive after symptom onset is uncertain, some need urgent surgery, and many have anticoagulant exposure or blood-pressure instability. A future exosome trial would need a narrow enrollment window, clear imaging criteria, and safety stopping rules before efficacy claims could be credible.
Best current interpretation: hUCMSC exosomes are a preclinical anti-inflammatory candidate for secondary injury after ICH. The 2026 study makes the mechanism more specific by tying exosomes to PI3K/AKT activation, lower PKM2-LDHA-H3K18la signaling, and better rodent neurological scores, but it remains an animal-and-cell model result.
Questions About Exosomes for Intracerebral Hemorrhage
Did the exosomes stop bleeding?
No. The study targeted secondary injury after experimental hemorrhage, especially inflammation and lactylation signaling, rather than the initial bleeding event.
Why focus on astrocytes?
Astrocytes help regulate inflammation, metabolism, blood-brain barrier support, and scar-like responses after brain injury. Hemin-treated astrocytes gave the researchers a focused model of blood-product-driven injury.
Is this ready for human ICH?
No. Exosome source, purification, dose, timing, biodistribution, sterility, and potency testing would all need rigorous development before human emergency use.
Does this mean lactate is always harmful after brain injury?
No. Lactate can be an energy substrate and a signaling molecule. The concern in this study was a specific injury-linked glycolysis-lactylation pattern involving PKM2, LDHA, and H3K18la that appeared to support inflammatory signaling after experimental ICH.
What would make the result more convincing?
A stronger package would replicate the neurological benefit in additional ICH models, identify exosome cargo tied to the pathway, test delayed dosing beyond 6 hours, and show that a standardized product works without harmful immune, clotting, or off-target effects.
References
- Zhang A, Zhang Z, Liu R, Zhao Z, Liu L. Exosomes derived from human umbilical cord mesenchymal stem cells attenuate neuroinflammation in intracerebral hemorrhage rats by modulating lactylation modification. Journal of Translational Medicine. 2026;24:588. https://doi.org/10.1186/s12967-025-07041-w
- Shi K, Tian DC, Li ZG, Ducruet AF, Lawton MT, Shi FD. Global brain inflammation in stroke. Lancet Neurology. 2019. https://doi.org/10.1016/s1474-4422(19)30078-x
- Zhang D, Tang Z, Huang H, et al. Metabolic regulation of gene expression by histone lactylation. Nature. 2019. https://doi.org/10.1038/s41586-019-1678-1
- Keep RF, Hua Y, Xi G. Intracerebral haemorrhage: mechanisms of injury and therapeutic targets. Lancet Neurology. 2012;11:720–731. https://doi.org/10.1016/s1474-4422(12)70104-7