A 2026 systematic review found that microglia-related immune signals do not line up cleanly with psychiatric diagnosis labels: major depression showed frontolimbic TSPO-PET increases, while schizophrenia showed elevated kynurenic acid in cerebrospinal fluid.1 The strongest interpretation is that immune-brain markers may sort subgroups better than DSM categories do.
Research Highlights
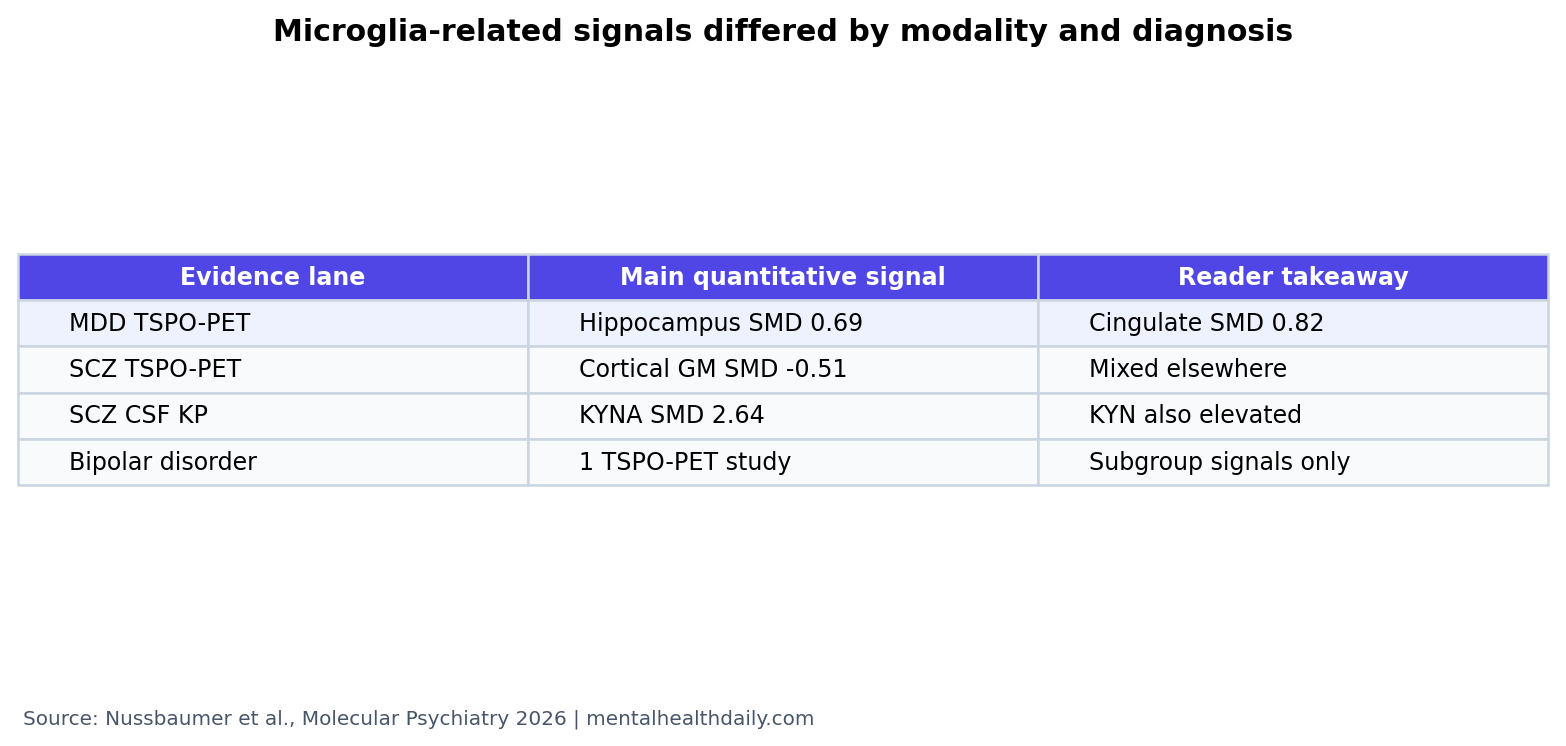
- Depression had the clearest TSPO-PET signal: pooled binding was higher in hippocampus (SMD 0.69), cingulate cortex (SMD 0.82), and prefrontal cortex (SMD 0.42).1
- Schizophrenia did not show the same PET pattern: the only significant pooled TSPO finding was lower whole-brain cortical gray-matter binding (SMD −0.51), not a simple inflammatory increase.1
- Kynurenic acid separated schizophrenia more clearly: CSF KYNA was higher in schizophrenia (SMD 2.64, 95% CI 1.16 to 4.13), with high heterogeneity.1
- Bipolar disorder evidence remained thin: TSPO-PET rested on 1 hippocampal study, so diagnosis-level claims are premature.1
- Subgroups are the better target: suicidality, psychosis, inflammation state, and region-specific markers explained more than a 3-diagnosis split.1
Microglia are immune-surveillance cells inside the brain. They clear debris, shape synapses, release cytokines, and can change neuronal signaling when systemic inflammation, stress biology, infection, blood-brain barrier disruption, or local brain injury shifts their state.
TSPO-PET is positron emission tomography imaging of the translocator protein, a marker used as an indirect in vivo readout of brain immune activation. It is useful, but not microglia-specific: astrocytes, endothelial cells, and technical choices such as tracer and quantification method can change the signal.
The kynurenine pathway is a tryptophan-metabolism route that can produce neuroactive compounds. Kynurenic acid blocks NMDA and alpha-7 nicotinic receptors; quinolinic acid stimulates NMDA receptors. That makes the pathway relevant to glutamate signaling, cognition, mood, and psychosis.
Depression Showed Frontolimbic TSPO-PET Increases
Nussbaumer et al. found the most reproducible in vivo microglia-related signal in major depressive disorder. Pooled TSPO binding was higher in the hippocampus (SMD 0.69, 95% CI 0.36 to 1.02), cingulate cortex (SMD 0.82, 95% CI 0.45 to 1.19), and prefrontal cortex (SMD 0.42, 95% CI 0.11 to 0.72).1
Standardized mean difference means the patient-control gap after putting different measurement scales on one common scale. Values around 0.4 are usually modest; values near 0.8 are larger. In this review, the cingulate and hippocampal depression estimates were not tiny background noise.
The regional pattern also fits depression biology better than a whole-brain inflammation slogan. Hippocampus, cingulate cortex, and prefrontal cortex sit inside stress, mood, memory, and self-regulation circuits. A frontolimbic signal says more than a generic inflammatory label.
Schizophrenia Looked Heterogeneous on TSPO-PET
Schizophrenia did not show a mirrored version of the depression result. The review reported mixed or lower TSPO-PET findings across regions, with the only significant pooled signal showing lower whole-brain cortical gray-matter binding in VT-based studies (SMD −0.51, 95% CI −0.92 to −0.10).1
That result is easy to misread. Lower TSPO binding in schizophrenia is compatible with several explanations: cellular state, illness stage, medication exposure, symptom subtype, or measurement method. TSPO-PET is a biologically messy signal rather than a clean one-direction inflammation meter.
De Picker et al. had already shown that TSPO-PET estimates differ strongly by quantification method across brain disorders; reference-tissue methods produced a positive shift compared with VT-based methods.2 Nussbaumer et al. therefore treated schizophrenia PET heterogeneity as a central result, not as a nuisance to average away.1
Kynurenic Acid Was the Stronger Schizophrenia Signal
The cerebrospinal-fluid pattern was more coherent for schizophrenia. CSF kynurenic acid was higher in schizophrenia (SMD 2.64, 95% CI 1.16 to 4.13), and a separate psychosis CSF meta-analysis also found higher KYNA and kynurenine.1,3
Kynurenic acid matters because it can dampen NMDA-receptor and alpha-7 nicotinic-receptor signaling. Both receptor systems are relevant to cognition, sensory gating, and glutamatergic theories of schizophrenia. A KYNA-skewed pathway is therefore also a plausible neural-computation marker.
Depression did not show the same CSF kynurenine-pathway pattern. MDD findings were largely null in CSF, with only a trend toward higher quinolinic acid based on 2 studies and extreme heterogeneity.1 Bipolar disorder showed a possible KYNA trend, but again with sparse data and I2 near 98%.1
Bipolar Disorder Was Too Sparse for a Diagnosis-Wide Claim
Bipolar disorder is often forced into either the “mood” or “psychosis” side of the old divide. The biomarker literature did not support that neat placement. TSPO-PET evidence in bipolar disorder came from 1 study reporting right hippocampal increases, while postmortem microglial markers were mostly unchanged at the diagnosis level.1
Signals appeared more informative after subgrouping. Suicide-stratified postmortem work and psychosis-linked kynurenine-pathway findings suggested that bipolar biology may separate by state, symptom dimension, and clinical subgroup rather than by the diagnostic label alone.
Evidence-strength note: this is a systematic review, but bipolar-specific conclusions remain limited because several key claims rest on single studies or descriptive synthesis. The review can identify a pattern worth testing; it cannot assign individual bipolar patients to an immune subtype.
Diagnosis Labels Are Too Blunt for Immune-Brain Biomarkers
Goldsmith et al. previously found blood cytokine alterations across schizophrenia, bipolar disorder, and depression, but those peripheral immune changes did not turn diagnoses into clean biological boxes.4 Nussbaumer et al. reached a similar conclusion from brain and CSF modalities: immune-brain readouts may be real, but categorical diagnosis is the wrong resolution.
Better stratification would test specific dimensions:
- Symptom dimension: psychosis burden, cognitive impairment, suicidality, anhedonia, or treatment resistance.
- Biological state: systemic inflammation, blood-brain barrier disruption, stress-axis activation, or medication exposure.
- Regional target: cingulate, hippocampus, prefrontal cortex, cortical gray matter, or white matter.
- Modality: TSPO-PET, CSF metabolites, postmortem cell markers, and future microglia-specific tracers.
This is the practical shift. “Depression vs. schizophrenia vs. bipolar disorder” is useful for clinical language, but it may be too wide for microglia and kynurenine biology. A transdiagnostic subgroup can be more biologically coherent than a diagnosis-wide average.
Anti-Inflammatory Treatment Needs Biomarker Selection
The treatment implication is narrower than the biomarker excitement. If microglia-related findings are subgroup-specific, anti-inflammatory or kynurenine-targeted trials should not enroll broad diagnosis groups and then expect a clean average benefit. They should identify the biological state they are trying to change.
For depression: a trial might enrich for elevated peripheral inflammation, frontolimbic TSPO-PET signal, stress-axis activation, or treatment-resistant inflammatory symptoms. The target would be the immune-active subgroup, not everyone with low mood.
For schizophrenia: a trial might focus on kynurenine-pathway biology, cognition, glutamatergic dysfunction, or psychosis-linked inflammatory phenotypes. KYNA elevation is more relevant to receptor signaling than to a generic “brain inflammation” label.
For bipolar disorder: the immediate need is basic stratification. The current evidence is too sparse to justify diagnosis-wide biomarker claims, but psychotic features, suicidality, mood state, and inflammatory subtype are plausible separators for future work.
Blood-vs-brain caution: peripheral cytokines can help flag immune state, but blood results do not automatically identify the regional brain signal. A high C-reactive protein value, a cingulate TSPO increase, and a CSF kynurenine-pathway shift may overlap in some patients and diverge in others.
The next useful studies should combine modalities in the same people: blood cytokines, TSPO-PET or newer immune-cell tracers, CSF or plasma kynurenine metabolites, symptom dimensions, medication history, and longitudinal outcome. The goal is not another one-number inflammation score. It is a map from biological state to psychiatric phenotype and treatment response.
That standard would also reduce overinterpretation of null results. If a broad depression trial of an immune drug fails, the failure may mean the drug is weak, the target is wrong, the biomarker did not select the right subgroup, or the outcome was too far downstream. Without matching biology to symptom dimension, a negative trial can be as hard to interpret as a positive one.
A sharper design would enroll by immune phenotype in addition to diagnosis. For example, depressed patients with frontolimbic TSPO elevation, schizophrenia patients with high kynurenic acid, and bipolar patients with psychotic or suicidal inflammatory signatures may need different tests rather than one cross-diagnostic inflammation bucket.
Medication status is another major separator. Antipsychotics, antidepressants, mood stabilizers, smoking, obesity, infection, and sleep disruption can all move immune markers and kynurenine biology.
Without that control, diagnosis differences can partly reflect treatment history.
That makes matched cohorts essential.
Questions About Microglia and Kynurenine in Psychiatry
Does this prove neuroinflammation causes depression or schizophrenia?
No. The review found biomarker patterns, not causality. TSPO-PET and CSF metabolites can reflect downstream, compensatory, or state-dependent biology.
Why is schizophrenia linked to kynurenic acid?
Kynurenic acid can reduce NMDA and alpha-7 nicotinic receptor activity. That makes it relevant to glutamate signaling and cognition, but it is not a standalone schizophrenia test.
Could anti-inflammatory treatment help psychiatric patients?
Possibly for subgroups, but the review argues against diagnosis-wide treatment claims. Future trials need inflammatory phenotype, symptom dimension, and biomarker-defined entry criteria.
What should readers take from the bipolar findings?
Bipolar evidence is underpowered. The more honest conclusion is that bipolar disorder needs targeted, subgroup-aware microglia and kynurenine studies before strong claims are made.
References
- Nussbaumer M, Guest PC, Schiltz K, et al. Multimodal microglial and kynurenine pathway alterations across the affective-psychosis spectrum: a systematic review of patterns, heterogeneity, and dimensional implications. Molecular Psychiatry. 2026. doi:10.1038/s41380-026-03614-3
- De Picker LJ, Morrens M, Branchi I, et al. TSPO PET brain inflammation imaging: a transdiagnostic systematic review and meta-analysis of 156 case-control studies. Brain, Behavior, and Immunity. 2023;113:415-431. doi:10.1016/j.bbi.2023.07.023
- Romer TB, Jeppesen R, Christensen RHB, Benros ME. Biomarkers in the cerebrospinal fluid of patients with psychotic disorders compared to healthy controls: a systematic review and meta-analysis. Molecular Psychiatry. 2023;28:2277-2290. doi:10.1038/s41380-023-02059-2
- Goldsmith DR, Rapaport MH, Miller BJ. A meta-analysis of blood cytokine network alterations in psychiatric patients: comparisons between schizophrenia, bipolar disorder and depression. Molecular Psychiatry. 2016;21:1696-1709. doi:10.1038/mp.2016.3