A 2026 review in Purinergic Signalling argues that P2X7 receptors are one of the clearest molecular bridges between stress, ATP danger signaling, microglial inflammation, NLRP3 inflammasome activation, reduced BDNF, and new antidepressant drug targets.1
Research Highlights
- P2X7 is the lead receptor: Mattova et al. reviewed 7 ATP-gated P2X receptor subunits, with P2X7 carrying the strongest depression-relevant stress-inflammation signal.1
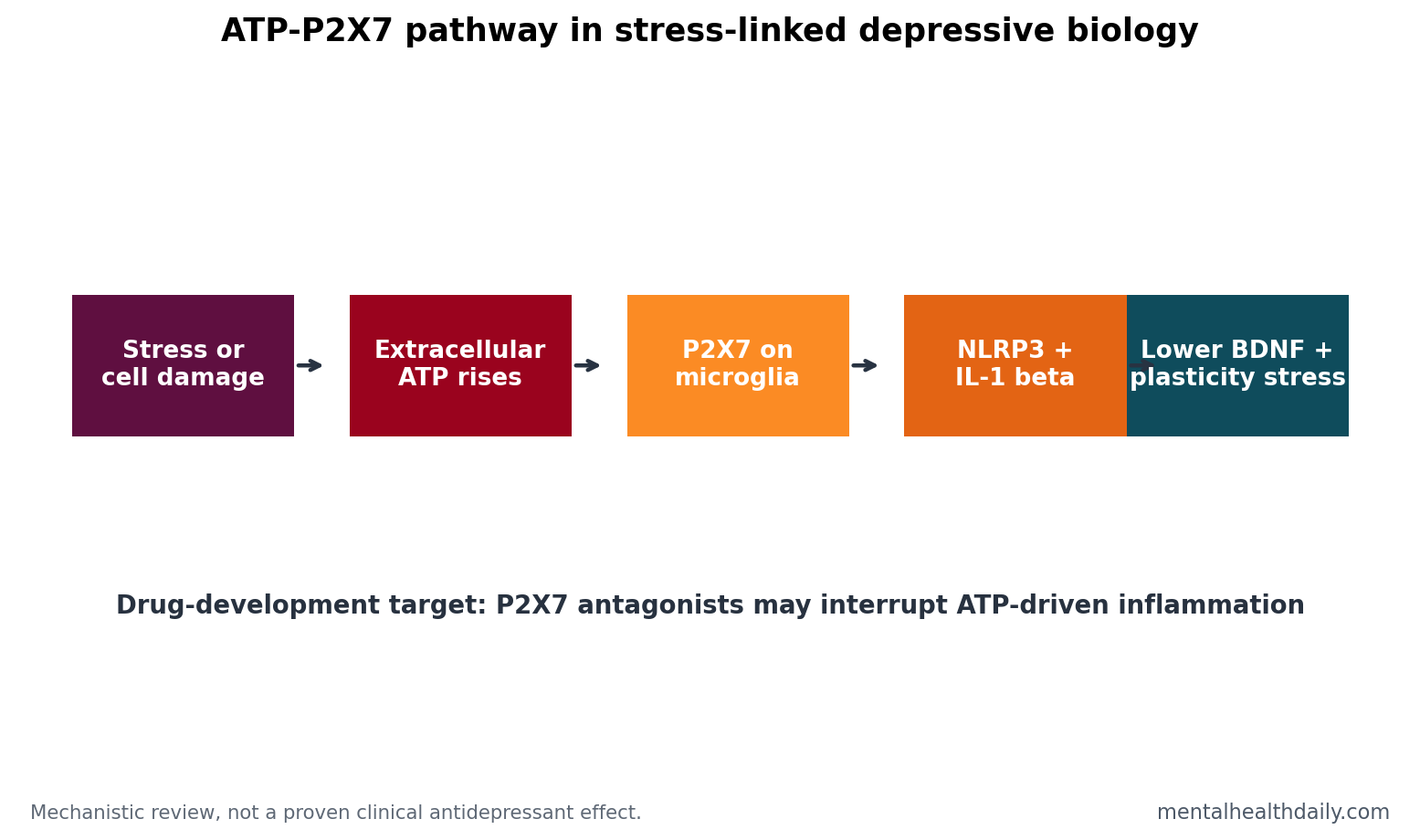
- Microglia are the pathway hub: high extracellular ATP can activate P2X7 on microglia, triggering NLRP3 inflammasome signaling and release of IL-1β and IL-18.1
- Animal evidence is stronger than human efficacy: P2X7 blockade reduced depression-like behavior in several rodent stress models, but clinical antidepressant proof remains early.1
- Genetics are mixed: a rapid-cycling bipolar signal for rs2230912 had OR = 2.2 (P = 0.002), but broader candidate-gene and GWAS evidence did not make P2X7 a single-gene explanation.1
- Clinical candidates exist: JNJ-54175446 and JNJ-55308942 are discussed as human-stage P2X7 antagonists, but they remain drug-development signals rather than proven depression treatments.1
P2X receptors are ion channels opened by extracellular ATP. Inside cells, ATP is energy currency. Outside cells, ATP can act like a danger signal, telling immune and glial cells that tissue stress, injury, inflammation, or cellular disruption is present.
P2X7 is the most depression-relevant member of this receptor family because it is highly involved in immune activation. It requires relatively high extracellular ATP, behaves like a damage sensor, and can trigger inflammatory cascades that affect brain plasticity.
Mechanistic value: the review identifies a specific receptor-level route through which stress biology, glial immune activity, cytokines, and plasticity could be connected in a druggable way. A druggable pathway is more useful than a vague inflammatory label.
That specificity matters for trial design, biomarker selection, patient subgrouping, and interpretable negative trials.
P2X7 Links ATP Danger Signals to Microglial Inflammation
The review’s central pathway is the microglia-P2X7-inflammasome axis.1 Microglia are immune-like cells in the brain. When stress or injury increases extracellular ATP, P2X7 receptors on microglia can activate the NLRP3 inflammasome, a molecular complex that helps convert inflammatory signals into cytokine release.
The cytokines emphasized in the review include IL-1β and IL-18. These are not “sadness chemicals.” They are immune messengers that can change synaptic plasticity, glial behavior, neurotransmission, and stress-response biology. That is the route by which inflammation can become mood-relevant.
NLRP3 inflammasome means an intracellular immune complex that helps activate inflammatory cytokines after danger signals. In the P2X7 model, extracellular ATP is one upstream alarm. P2X7 activation helps convert that alarm into microglial inflammatory output, which can then affect neurons and synapses.
BDNF Gives the Inflammation Story a Plasticity Endpoint
BDNF (brain-derived neurotrophic factor) is a growth factor that supports neuron survival, synaptic plasticity, and adaptive remodeling. The P2X7 review repeatedly connects inflammatory activation with downstream reductions in BDNF and neuroplasticity.1
The plasticity endpoint sharpens the mechanism because depression involves learning, reward, sleep, threat processing, energy, social behavior, and cognitive control. A receptor pathway becomes more plausible when it connects immune activation to plasticity systems that can alter those domains.
BDNF also keeps the model from becoming pure immune-system language. If inflammatory signaling reduces growth-factor support, hippocampal plasticity, and stress adaptation, the pathway starts to explain why chronic stress can have cognitive, motivational, and mood consequences rather than only changes in blood cytokines.
P2X7 Antagonists Are Plausible but Not Proven Antidepressants
Animal-model evidence is the strongest part of the case. The review describes P2X7 genetic deletion or pharmacological inhibition preventing or reducing depression-like behavior in stress models, including chronic unpredictable stress and chronic social defeat stress contexts.1
The clinical side is earlier. JNJ-54175446 showed pharmacokinetic, safety, and anti-inflammatory properties in healthy-volunteer work and was reported to attenuate acute dysphoria after total sleep deprivation. JNJ-55308942 advanced from Phase I safety work into a Phase II bipolar-depression trial. Those facts support development; they do not establish routine treatment efficacy.
This is the right place for calibrated optimism. P2X7 antagonists are attractive because they target a plausible upstream inflammatory gate rather than downstream symptoms. The clinical risk is that a strong rodent stress signal becomes a weak human antidepressant once patient heterogeneity, dosing, blood-brain-barrier penetration, baseline inflammation, and outcome measures enter the trial.
Genetics Calibrate the P2X7 Claim
The review is careful enough to include the genetic weakness. Candidate-gene studies around P2RX7 have produced inconsistent results. One rapid-cycling bipolar-I analysis reported an association for rs2230912 (OR = 2.2, P = 0.002), but the result was not replicated. Meta-analytic and GWAS evidence does not support a simple P2X7-gene theory of major affective disorders.1
That calibration fits the broader genetics of mood disorders. Large bipolar-disorder GWAS work identified many loci and a highly polygenic architecture rather than one dominant inflammatory receptor gene.4 P2X7 may still matter as a pathway node even when common genetic variants in P2RX7 do not behave like a stand-alone risk marker.
Pathway-level genetics means a set of related genes may carry weak coordinated signal even when no single gene becomes decisive. The review notes purinergic receptor genes appearing in near-significant pathway analyses tied to synaptic membranes, trans-synaptic signaling, postsynaptic compartments, immune processes, and mitochondria. That is hypothesis-generating evidence, not a clinical genetic test.
P2X4 and P2X3 Broaden the Pathway Without Replacing P2X7
P2X4 and P2X3 receptors also appear in the review. P2X4 is expressed in neurons and microglia, is highly permeable to calcium, and can influence BDNF release and glial-neuronal communication. The review notes P2X4 ATP sensitivity around EC50 = 3-10 μM.1
P2X3 is better known for pain and sensory signaling. Its depression relevance is likely indirect: chronic pain, neuroimmune activation, and stress-related somatic symptoms can worsen mood. P2X3 is not the core affective-disorder receptor in this review.
The receptor hierarchy matters for drug development. P2X7 is the most direct inflammation-depression target. P2X4 may influence glial-neuronal communication and BDNF. P2X3 may matter most in chronic pain and somatic stress states where sensory input worsens mood. Treating all P2X receptors as one depression target would blur those differences.
The Clinical Use Is Subtyping, Not Universal Inflammation Talk
Evidence-strength note: this was a mechanistic review, not a new randomized antidepressant trial. It supports P2X7 as a biologically coherent target in stress-linked inflammatory depression models. It does not show that every depressed patient has P2X7 overactivation or that P2X7 antagonists outperform existing antidepressants.
The most realistic future is subgroup work: patients with inflammatory signatures, stress biology, sleep-disruption sensitivity, chronic pain, bipolar-depression profiles, or biomarker evidence that ATP-P2X7 signaling is active. That is a narrower and more useful claim than “inflammation causes depression.”
For readers, the practical implication is not to look for an over-the-counter P2X7 blocker. The practical implication is to understand why the next generation of antidepressant trials may divide patients by immune and stress-biology markers. If the pathway is real, the benefit will probably be concentrated rather than universal.
A realistic trial would not enroll “depression” as one undifferentiated category and hope for a large average effect. It would predefine inflammatory markers, stress-exposure profiles, sleep-deprivation sensitivity, pain comorbidity, bipolar-depression status, or other signs that ATP-P2X7 signaling is plausibly active. That kind of enrichment design is where the receptor biology becomes clinically testable.
Safety also matters. P2X7 is involved in immune defense and inflammatory signaling, so long-term blockade needs careful monitoring for infection risk, immune effects, and off-target biology. The receptor is promising because it is upstream, but upstream immune targets can have wider consequences than symptom-level drugs.
The review also keeps bipolar disorder in the frame. Immune, mitochondrial, and purinergic pathways may cut across mood diagnoses while still producing different clinical phenotypes. A P2X7-focused program would need to test unipolar depression and bipolar depression separately rather than assuming one mood-disorder mechanism.
Clinically, the current use is conceptual: P2X7 helps explain why stress, inflammation, sleep disruption, chronic pain, and plasticity can belong in the same biological conversation.
That conceptual use is still valuable when it prevents vague inflammation talk and forces researchers to name the receptor, cell type, cytokine pathway, and patient subgroup being tested.
A useful clinical program would also need biomarkers that can be measured repeatedly, such as inflammatory proteins, sleep-stress physiology, pain burden, or transcriptomic signatures. A receptor target becomes actionable only when clinicians can identify the patients most likely to carry that pathway state.
Outcome choice matters too. If P2X7 mainly affects fatigue, anhedonia, pain sensitivity, or stress reactivity, a total depression score may hide the benefit in the wrong endpoint.
Endpoint design should follow the biology being tested.
That is where mechanistic psychiatry becomes practically useful.
Questions About P2X7 Receptors and Depression
Is P2X7 a depression biomarker?
Not by itself. The review supports P2X7 as a pathway target, but genetic and clinical evidence is too mixed for a single-receptor diagnostic marker.
Are P2X7 antagonists available antidepressants?
No. They are investigational compounds and research targets. Existing evidence is promising enough for development, not strong enough for routine clinical use.
Why does ATP matter in depression?
Extracellular ATP can signal danger or stress. When it activates P2X7 receptors on microglia, it can trigger inflammatory pathways that alter plasticity and mood-relevant circuits.
References
- Mattova L, et al. ATP and major affective disorders: the involvement of P2X receptors. Purinergic Signalling. 2026. https://doi.org/10.1007/s11302-026-10147-5
- Iwata M, Ota KT, Duman RS. The inflammasome: pathways linking psychological stress, depression, and systemic illnesses. Trends in Neurosciences. 2016. https://doi.org/10.1016/j.tins.2016.04.005
- Bhattacharya A, et al. Pharmacological inhibition of the P2X7 receptor as a therapeutic strategy for mood disorders. Neuropsychopharmacology. 2018. https://doi.org/10.1038/npp.2017.217
- Stahl EA, et al. Genome-wide association study identifies 30 loci associated with bipolar disorder. Nature Genetics. 2019. https://doi.org/10.1038/s41588-019-0397-8