Intranasal esketamine — FDA-approved for treatment-resistant depression in 2019 — failed cost-effectiveness benchmarks against four cheaper third-line options in a 2026 Hong Kong modeling study, with incremental cost-effectiveness ratios (ICERs) of US$134,127 to US$312,750 per quality-adjusted life-year (QALY) at a US$50,000/QALY willingness-to-pay (WTP) threshold.1 Combination antidepressant therapy was the most cost-effective strategy modeled.
Research Highlights
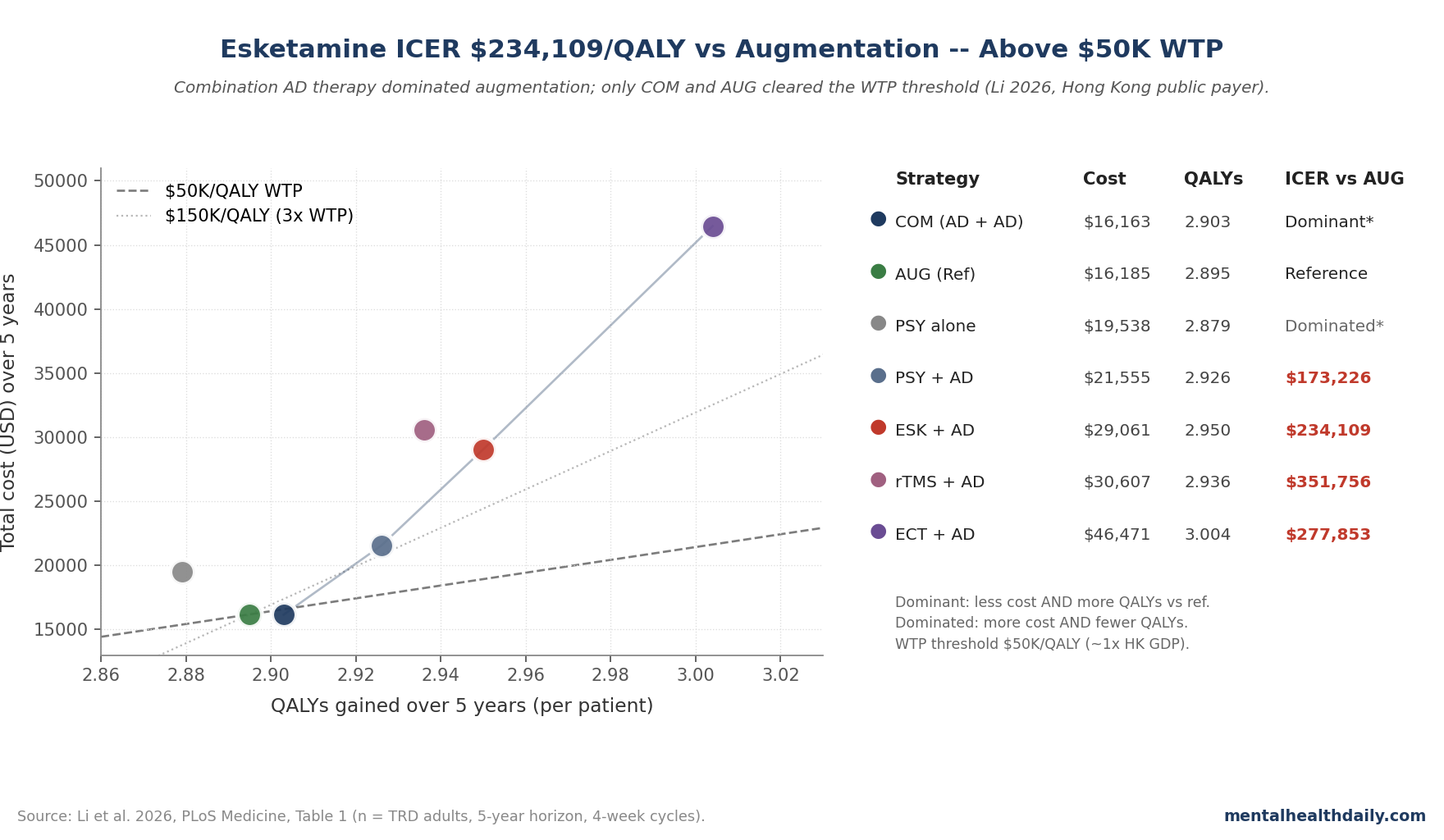
- Headline finding: Esketamine plus an oral antidepressant cost US$29,061 per patient over 5 years for 2.950 QALYs — about 80% more than augmentation (US$16,185) for 0.055 extra QALYs in the Hong Kong base-case.1
- ICER ladder: Esketamine vs. augmentation: US$234,109/QALY. Vs. combination therapy: US$274,426/QALY. Vs. psychotherapy plus AD: US$312,750/QALY. All exceed the US$50,000/QALY WTP threshold (~1× Hong Kong GDP per capita) by 3–6×.1
- Combination therapy won: Two oral antidepressants (mianserin or mirtazapine added to a first-line AD) cost US$16,163 for 2.903 QALYs — less expensive and more effective than augmentation, dominating it on the cost-effectiveness frontier.1
- Esketamine beat rTMS, lost to ECT on QALYs: Esketamine dominated rTMS (lower cost, higher QALYs). ECT plus AD produced more QALYs (3.004) but at US$46,471, with an ICER of US$322,407/QALY vs. esketamine.1
- Price cuts barely move it: A 75% reduction in esketamine acquisition price still left an ICER of US$116,327/QALY. Hitting US$50,000/QALY required cutting total per-patient cost ~35% (to US$18,935). Over a 20-year horizon, the ICER stayed at US$229,750/QALY.1
Cost-effectiveness modeling doesn’t tell payers whether a drug works. It tells them whether the price tag matches the value delivered, given the local cost of healthcare and what alternatives exist.
Esketamine works — the TRANSFORM-1/2 and SUSTAIN-1 trials are well-established.2,3 The question Li et al. asked is narrower: at Hong Kong public-payer prices, against the third-line options patients with TRD are actually offered, does esketamine pencil out?
Their answer is the third independent “no” in five years. A 2020 US analysis by Ross et al. concluded esketamine adjunct to oral AD was unlikely to be cost-effective at standard US WTP thresholds.4
The UK NICE technology appraisal declined esketamine for NHS use on the same grounds.5 Three jurisdictions, three different cost structures, three rejections at standard thresholds. The geography rotates; the math holds.
Esketamine Cost US$29,061 for 0.055 Extra QALYs vs. Augmentation
The Markov cohort model simulated adults with TRD over 5 years with 4-week cycles, drawing efficacy from TRANSFORM-1/2 and SUSTAIN-1 for esketamine and from network meta-analyses and trial pools for the six comparator strategies.1 Costs came from Hong Kong Hospital Authority utilization data and published unit costs.
All costs and outcomes were discounted at 3% per annum. The reference comparator was augmentation therapy — an oral antidepressant plus an antipsychotic (olanzapine, cariprazine, quetiapine, ziprasidone) or lithium — consistent with the NICE appraisal framing for real-world third-line care.
The base-case numbers are blunt. Esketamine plus AD cost US$29,061 per patient over 5 years for 2.950 QALYs.
Augmentation cost US$16,185 for 2.895 QALYs. The 0.055-QALY gain (roughly 20 days of full-quality life) cost an incremental US$12,876, working out to US$234,109 per QALY — 4.7× the WTP threshold.
Against psychotherapy plus AD, the ICER climbed to US$312,750/QALY. Against combination therapy, US$274,426/QALY.
Against psychotherapy alone, US$134,127/QALY. None of those four cleared US$50,000.
Combination Antidepressant Therapy Was the Most Cost-Effective Option
The most striking result isn’t about esketamine at all. It’s that combination therapy — adding a second oral antidepressant (mianserin or mirtazapine) to a first-line AD — dominated augmentation on both axes: lower 5-year cost (US$16,163 vs. US$16,185) and higher QALYs (2.903 vs. 2.895).1
Augmentation with second-generation antipsychotics is what most TRD patients in Hong Kong (and in the US, and in the UK) are actually offered as third-line treatment. The model puts a cheaper alternative ahead of it on the efficiency frontier — not by miles, but consistently.
On the cost-effectiveness frontier, the nondominated strategies were combination therapy (cheapest, lowest QALYs of the surviving set), psychotherapy plus AD, esketamine plus AD, and ECT plus AD — in that order of ascending cost. rTMS and psychotherapy alone were dominated and dropped from the frontier.
The ICER walking up the frontier from PSY+AD to ESK+AD was US$312,750/QALY, and from ESK+AD to ECT+AD was US$322,407/QALY.
Even a 75% Price Cut Doesn’t Get Esketamine to US$50,000/QALY
The most policy-relevant scenario analyses asked: what would have to change for esketamine to clear the WTP threshold?1
A 75% reduction in esketamine acquisition price — an aggressive negotiation outcome — brought the ICER vs. augmentation down to US$116,327/QALY. Still above the US$50,000 threshold, though within 3× WTP (US$150,000/QALY).
Reducing each dose from 84 mg to 56 mg, switching to direct intranasal administration with simpler monitoring, and applying NICE-style 3.5% discount rates produced incremental but not threshold-clearing improvements.
The most favorable scenario was extending the model cycle from 4 to 8 weeks (a structural proxy for less frequent administration), which dropped the ICER to US$73,556/QALY — the closest any non-threshold scenario got. Even there, esketamine remained not cost-effective at US$50,000/QALY.
The threshold-back-calculation scenario (Scenario 8) made the bar explicit: holding effectiveness constant, total per-patient esketamine cost would need to fall ~35%, from US$29,061 to US$18,935, to hit the US$50,000/QALY WTP. That’s the gap between current pricing and cost-effectiveness arithmetic.
Esketamine Beat rTMS but Lost to ECT on QALYs
On the neurostimulation comparators, the picture splits.1 Esketamine dominated rTMS plus AD: lower total cost (US$29,061 vs. US$30,607) and slightly higher QALYs (2.950 vs. 2.936).
For payers weighing esketamine vs. rTMS specifically, esketamine wins outright in this model.
ECT plus AD was the highest-QALY strategy modeled (3.004 QALYs, US$46,471). Going from esketamine to ECT cost US$322,407 per QALY — above WTP, but the QALY gain (0.054) is real and ECT’s clinical evidence base for severe TRD is older and arguably more robust than esketamine’s.6
The cost gradient reflects ECT’s anesthesia and inpatient/day-hospital infrastructure, not the procedure cost itself.
What this rearranges is the case for esketamine specifically. The pitch in the FDA-approval era was that esketamine was a less invasive, less stigmatized alternative to ECT for severe TRD.
That pitch survives the model. The cheaper-than-ECT framing also survives.
What doesn’t survive is the implicit comparison to augmentation and combination AD therapy — the much larger volume of TRD patients who would never have been considered for ECT in the first place.
Cost-Effectiveness Model Boundaries
Cost-effectiveness models trade comprehensiveness for tractability, and several real-world dimensions sit outside the framework.
Indirect comparisons. No head-to-head trial pits esketamine against augmentation against combination therapy. The model leans on heterogeneous trial populations and network meta-analytic effect estimates.
Real-world patient mixes can differ. The authors flag this as the study’s main limitation.1
Speed of response. Esketamine’s signature clinical feature — rapid antidepressant effect, often within hours to days — gets compressed into 4-week QALY cycles. For a patient with active suicidal ideation, the practical value of fast response isn’t fully captured by averaged QALY trajectories.
Whether that gap is large enough to flip the math is unclear; payers have generally concluded it isn’t.
Productivity and societal costs. The Hong Kong analysis used a healthcare-payer perspective. Models taking a societal perspective — including productivity, caregiver burden, workforce participation — can shift ICERs, sometimes substantially.
Ross et al.’s US analysis modeled both perspectives and reached similar conclusions.4
Pricing isn’t fixed. Modeled cost is the variable everyone can move. Janssen’s pricing strategies, biosimilar entry timelines, and direct-to-clinic delivery models could all shift the arithmetic.
The Scenario 8 analysis quantifies the gap: ~35% total cost reduction to hit WTP at the modeled effectiveness.
How This Lines Up With US and UK Cost-Effectiveness Verdicts
The Hong Kong findings aren’t an outlier. They line up with the two prior major payer-perspective analyses.4,5
Ross et al. modeled US esketamine cost-effectiveness in 2020 and found ICERs well above standard US WTP thresholds (US$100,000–US$150,000/QALY) under base-case assumptions, with sensitivity to long-term effectiveness, dosing frequency, and acquisition price — the same levers Li et al. find in Hong Kong.4 The UK NICE TA854 appraisal declined esketamine for routine NHS use, citing incremental cost relative to alternatives.5
What’s worth noting is that the three analyses span very different healthcare-system structures — US mixed payer, UK single-payer NHS, Hong Kong public payer — and very different absolute price points. The shared conclusion isn’t a quirk of one cost structure.
It’s a stable finding about esketamine’s price-to-incremental-effectiveness ratio at standard WTP thresholds, across three jurisdictions and seven years.
For clinicians, that doesn’t mean esketamine has no place. It does mean the pitch — rapid antidepressant action, FDA approval, novel mechanism — has to be weighed against payer arithmetic that has, so far, consistently come out the same way.
For TRD patients with severe functional impairment, urgent suicidality, or prior failure of multiple alternatives, the case can still be made on grounds the model doesn’t fully capture. For broader TRD use, the model’s answer is that combination AD therapy and augmentation are doing similar work for substantially less money.
Questions About Esketamine Cost-Effectiveness
What does “not cost-effective” actually mean here?
It means that under a US$50,000/QALY willingness-to-pay threshold — the standard Hong Kong public-payer benchmark, roughly equal to one year of GDP per capita — esketamine’s incremental cost per quality-adjusted life-year gained exceeded that threshold by 3–6× against four of six comparator strategies. It doesn’t mean the drug doesn’t work.
It means the price asked exceeds the value delivered at standard payer benchmarks.
Why use a US$50,000/QALY threshold and not US$150,000?
The US$50,000/QALY threshold is widely used in international cost-effectiveness analyses as a conservative WTP anchor and corresponds to ~1× Hong Kong GDP per capita. WHO methodology has historically used 1–3× GDP per capita as a flexibility band.
At US$150,000/QALY (~3× GDP per capita), esketamine still failed in the base case but came closer in some scenarios — the 75% price-cut scenario reached US$116,327/QALY, within the 3× band.
Did Li et al. find any scenario where esketamine cleared US$50,000/QALY?
No, except Scenario 8, which was explicitly a back-calculation: holding effectiveness constant, what total cost reduction would the drug need? Answer: ~35%, bringing per-patient cost to US$18,935.
Every other scenario — price cuts, dosing changes, longer time horizons, NICE-style discounting — left esketamine above US$50,000/QALY.
How does this match the US and UK cost-effectiveness verdicts?
Closely. Ross et al.’s 2020 US analysis concluded esketamine was unlikely to be cost-effective at US WTP thresholds; the UK NICE TA854 declined esketamine for routine NHS use.
Three independent analyses across three healthcare systems with very different cost structures reached the same headline conclusion at standard WTP thresholds.
Does this mean patients shouldn’t try esketamine?
Cost-effectiveness analyses inform payer and health-system decisions. They don’t dictate individual clinical decisions.
For a patient with severe TRD, multiple prior antidepressant failures, urgent functional impairment, or active suicidality, esketamine can be the right call regardless of population-level ICER arithmetic. The model’s relevance is to coverage policy and care-pathway design, not bedside decisions.
What’s the most cost-effective TRD treatment in this model?
Combination antidepressant therapy — adding a second oral AD (mianserin or mirtazapine) to a first-line antidepressant. It dominated augmentation (lower cost, more QALYs) and sat at the bottom of the cost-effectiveness frontier.
That’s a bigger story for routine TRD care than the esketamine result.
What changes between this study and 5 years from now?
The most plausible mover is esketamine pricing. Generic competition, biosimilar pathways, or direct-to-clinic delivery models that reduce monitoring overhead could close some of the ~35% cost gap Scenario 8 quantifies.
Long-term real-world effectiveness data — particularly on duration of response and relapse rates beyond the SUSTAIN-1 horizon — could also shift modeled QALY estimates either direction.
Did the model use real Hong Kong cost data?
Yes. Healthcare resource utilization and unit costs came from Hong Kong Hospital Authority’s Clinical Data Analysis and Reporting System and from published Hong Kong sources.
Efficacy parameters were drawn from international trial data (TRANSFORM-1/2, SUSTAIN-1) and network meta-analyses, since equivalent local clinical-outcome data weren’t available in the EMR. The protocol, parameters, and code are publicly archived on Zenodo (DOI 10.5281/zenodo.19520620).
References
- Li Y, Chan VKY, Jit M, Cheng FWT, Yiu HHE, Bishai DM, et al. Cost-effectiveness of esketamine versus alternative treatment strategies for treatment-resistant depression in Hong Kong: a multi-armed modeling study. PLoS Medicine. 2026;23(4):e1005047. doi:10.1371/journal.pmed.1005047
- Daly EJ, Singh JB, Fedgchin M, Cooper K, Lim P, Shelton RC, et al. Efficacy and safety of intranasal esketamine adjunctive to oral antidepressant therapy in treatment-resistant depression: a randomized clinical trial. JAMA Psychiatry. 2018;75(2):139–148. doi:10.1001/jamapsychiatry.2017.3739
- Daly EJ, Trivedi MH, Janik A, Li H, Zhang Y, Li X, et al. Efficacy of esketamine nasal spray plus oral antidepressant treatment for relapse prevention in patients with treatment-resistant depression: a randomized clinical trial (SUSTAIN-1). JAMA Psychiatry. 2019;76(9):893–903. doi:10.1001/jamapsychiatry.2019.1189
- Ross EL, Soeteman DI. Cost-effectiveness of esketamine nasal spray for patients with treatment-resistant depression in the United States. Psychiatric Services. 2020;71(10):988–997. doi:10.1176/appi.ps.201900625
- National Institute for Health and Care Excellence. Esketamine nasal spray for treatment-resistant depression: technology appraisal guidance TA854. NICE; 2022. nice.org.uk/guidance/ta854
- UK ECT Review Group. Efficacy and safety of electroconvulsive therapy in depressive disorders: a systematic review and meta-analysis. Lancet. 2003;361(9360):799–808. doi:10.1016/S0140-6736(03)12705-5