
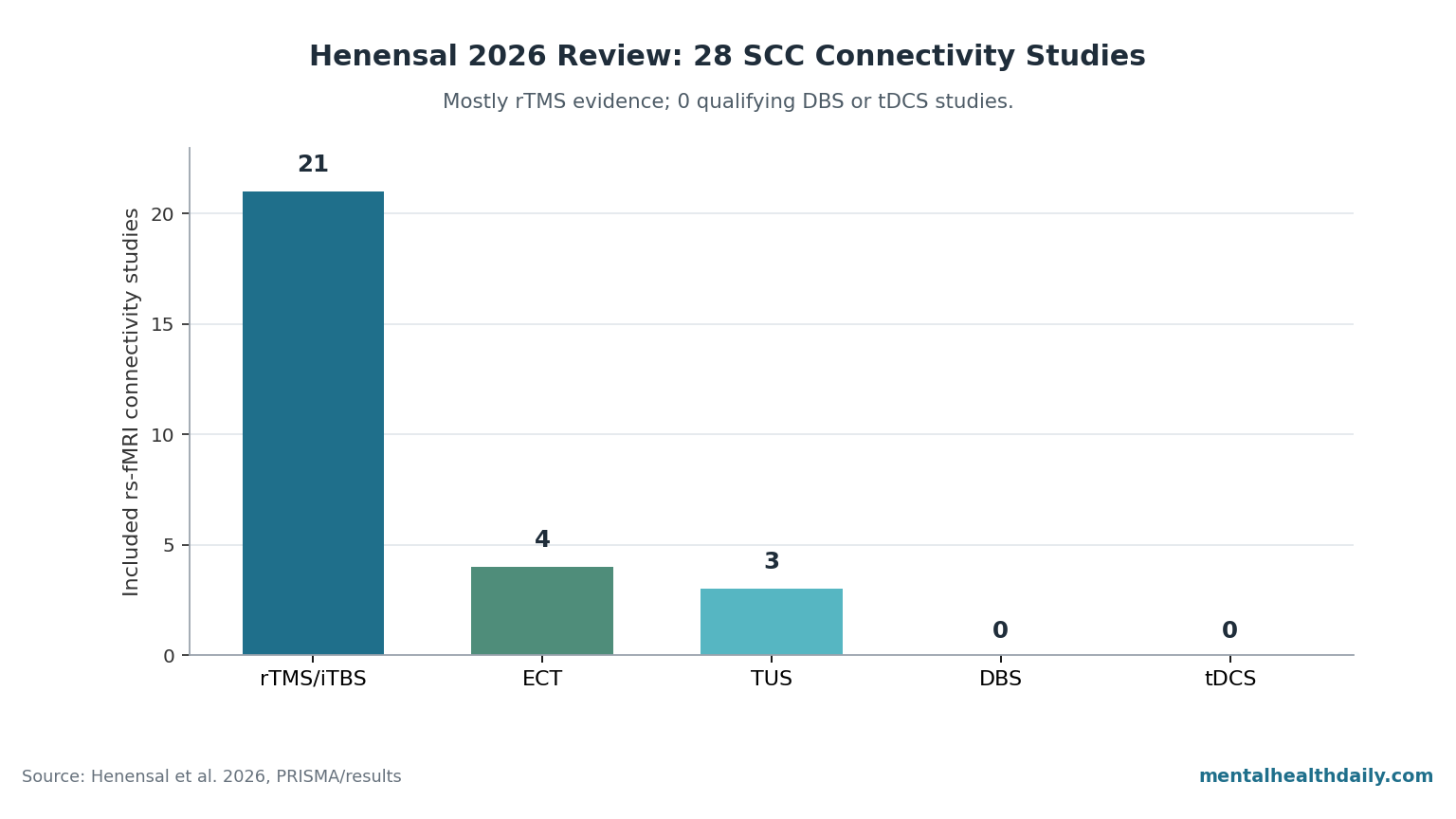
A 2026 systematic review of subcallosal cingulate (SCC) functional connectivity found 28 qualifying resting-state fMRI studies in depression: 21 rTMS/iTBS studies, 4 ECT studies, 3 focused-ultrasound studies, and 0 DBS or tDCS studies.1 That number is the useful correction: SCC DBS may still be biologically plausible, but the current fMRI connectivity literature mostly explains noninvasive stimulation, not implanted stimulation.
Research Highlights
- Evidence base is lopsided: Henensal et al. screened 442 records and included 28 studies, but 21 of 28 were rTMS/iTBS studies while DBS and tDCS contributed 0 qualifying resting-state fMRI studies.1
- DBS was absent for technical reasons: the review says implanted electrodes and extension wires can create MRI artifacts, so much SCC DBS work uses PET, tractography, scalp EEG, or intracranial recordings instead of pre/post fMRI connectivity.1
- rTMS has the strongest SCC predictor: several studies link better response to stronger baseline DLPFC-SCC anticorrelation than weaker anticorrelation, but a 295-patient cohort found the signal modest and subgroup-dependent.2,3,4
- TUS is early but directly relevant: the review found 3 transcranial ultrasound studies; one direct left-SCC protocol used 25 sessions in 5 treatment-resistant depression patients and shifted SCC-DLPFC connectivity from negative to positive.1,5
- DBS remains investigational: BROADEN failed its 6-month sham-controlled Phase 3 test, while later connectomic targeting and a 2023 intracranial biomarker study keep the SCC target alive without proving routine clinical efficacy.6,7,8
Subcallosal cingulate means the subgenual anterior cingulate region under the front of the corpus callosum, often discussed as Brodmann area 25. Depression studies care about it because it sits at a traffic junction between medial prefrontal cortex, default-mode regions involved in self-referential thought, and limbic regions involved in negative emotion.
Functional connectivity means correlated activity between brain regions during scanning. In resting-state fMRI, researchers do not watch a patient perform a task; they ask whether the SCC rises and falls with regions such as the dorsolateral prefrontal cortex (DLPFC), ventromedial prefrontal cortex, precuneus, hippocampus, amygdala, or temporal pole.
The 2026 review is useful because it separates that network-mapping question from the older, louder question of whether SCC DBS should be an approved depression treatment.
28 fMRI Studies, 0 Qualifying DBS Studies
Henensal et al. pre-registered the review and searched PubMed, Web of Science, Cochrane, and reference lists through December 15, 2025. Their PRISMA flow started with 442 records, removed 123 duplicates, screened 319 abstracts, assessed 179 full texts, and ended with 28 included articles.1
The modality split is the central result: 21 rTMS/iTBS studies, 4 ECT studies, 3 TUS studies, 0 DBS studies, and 0 tDCS studies. That does not establish DBS researchers stopped studying the SCC.
It means the specific evidence lane in this review — adult depression studies using resting-state fMRI to measure SCC connectivity before or after stimulation — mostly belongs to noninvasive stimulation.
The review states the contradiction directly: “Contrary to the initial objectives and predefined inclusion criteria, no articles involving tDCS or DBS were included in this review.”1 The reason is partly technical. Implanted DBS leads and extension wires can distort MRI signal near the target, so DBS studies often lean on PET, diffusion tractography, or intracranial local field potentials rather than conventional resting-state fMRI connectivity.
SCC Connectivity After BROADEN Failed
SCC DBS began with a small but striking open-label signal. Mayberg et al. reported in 2005 that chronic high-frequency stimulation near the SCC improved severe treatment-resistant depression in a 6-patient series, with metabolic changes in the broader limbic-cortical network.9
That early work made the target famous because the patients were not mild antidepressant nonresponders; they had long, disabling, treatment-resistant illness.
The randomized test did not reproduce that excitement. BROADEN, the pivotal multisite Phase 3 trial of SCC DBS, compared active stimulation with sham stimulation and was stopped for futility.
In the 2017 report, 12 of 60 active-stimulation patients and 3 of 30 sham patients met response criteria at 6 months, a directional difference that was not statistically convincing and far below the open-label expectation.6
That failure matters because it blocks the simplest story. SCC DBS is not a treatment that sailed through early trials and merely awaits better marketing.
The best calibrated reading is sharper: coordinate-based SCC DBS failed its sham-controlled test, while later work argues that coordinate-based targeting may have missed the relevant white-matter bundles in many patients.
Connectomic DBS Targets Bundles, more than Brodmann Area 25
Connectomic targeting uses a patient’s brain-connectivity map to guide stimulation toward circuits rather than a fixed coordinate. In SCC DBS, the post-BROADEN argument is that the therapeutic target is more than gray matter labeled BA25; it is a convergence zone where several white-matter pathways meet.
Riva-Posse et al. retrospectively examined successful SCC DBS contacts and identified 4 tract families that mattered: forceps minor, cingulum bundle, uncinate fasciculus, and frontostriatal fibers.10 Their prospective 2018 test then used individualized tractography for SCC DBS targeting and reported high response in a small open-label treatment-resistant depression cohort.7
That does not erase BROADEN. It reframes the failed trial as evidence against a broad coordinate recipe, not as final proof that the SCC circuit is irrelevant.
The problem is that the revived connectomic DBS evidence is still mostly small, open-label, and specialized. It is promising enough to keep the target alive, but not strong enough to make SCC DBS routine care.
Alagapan et al. added a different kind of support in 2023 by recording chronic intracranial activity from SCC DBS systems. The study reported that cingulate dynamics tracked depression recovery and could identify a neural-state transition associated with clinical improvement.8
That is not a regulatory efficacy trial, but it strengthens the mechanistic case that SCC stimulation can engage a depression-relevant circuit when the implant is well placed and the patient responds.
The rTMS Signal Is Stronger Than the DBS Signal in This Review
For everyday depression care, the review’s most practical signal is not DBS. It is the DLPFC-SCC rule for repetitive transcranial magnetic stimulation (rTMS), a noninvasive treatment that stimulates cortex through the scalp.
The DLPFC is a surface-accessible frontal target; the SCC is deeper. The working idea is that stimulating a DLPFC spot strongly anticorrelated with the SCC may indirectly push the SCC network in a therapeutic direction.
Fox et al. helped establish this logic in 2012 by showing that more effective depression rTMS targets were more strongly connected, in an inverse direction, with the subgenual cingulate.2 Weigand et al. later prospectively validated that stronger DLPFC-SCC anticorrelation predicted better antidepressant response to rTMS sites.3
The 2026 review finds repeated support for this general pattern, but not a clean plug-and-play biomarker. Some studies found positive SCC connections predicting response in other regions, including orbitofrontal and default-mode areas.
Some studies reported post-treatment connectivity shifting in opposite directions depending on protocol, target, laterality, and analytic method. Elbau et al.’s 295-patient sample is the necessary cold shower: sgACC-DLPFC connectivity related to outcomes, but the association was generally weak and strongest in a smaller subgroup with respiration-related signal patterns.4
The practical interpretation is not “connectivity does not matter.” It is that SCC-DLPFC anticorrelation is a real group-level clue, while individual-level targeting still depends on MRI quality, region-of-interest definition, electric-field modeling, and patient heterogeneity.
TUS Tests the SCC Without an Implant
Transcranial focused ultrasound (TUS) uses acoustic energy to modulate brain tissue without an implanted electrode. The Henensal review found only 3 TUS studies, so this is early evidence, but it is directly relevant because TUS can interrogate the SCC without the MRI-artifact problem created by DBS hardware.
Attali et al. delivered 25 sessions of metalens-based TUS to the left SCC in 5 treatment-resistant depression patients. In the review’s summary, left SCC connectivity with the left DLPFC shifted from negative to positive, connectivity increased with supplementary motor and postcentral regions, and connectivity decreased with right hippocampal and parahippocampal regions.1,5
Other TUS studies targeted the DLPFC rather than the SCC. Oh et al. reported increased connectivity between SCC subregions and medial prefrontal or cerebellar regions after active DLPFC-focused ultrasound.11
The mixed direction is not a nuisance detail; it is the point. Direct SCC stimulation and cortical DLPFC stimulation can move the SCC network through different routes.
ROI Definitions Make or Break SCC Connectivity Claims
A region-of-interest (ROI) is the chunk of brain a study defines as the SCC seed for connectivity analysis. Henensal et al. show how unstable that definition can be.
Studies used coordinates such as (2,18,−8), (6,16,−10), (1,25,−11), (4,26,−10), and (−4,21,−11), with different sphere sizes and inconsistent laterality reporting.1
Those choices are not clerical. Move the seed a few millimeters, change the sphere size, or mix left and right SCC definitions, and a connectivity result can start describing a different tissue neighborhood.
The review also notes that the SCC has low fMRI signal-to-noise because of susceptibility artifacts, which makes individual-level connectivity targeting harder to reproduce.1
This is why the article’s headline cannot be “SCC connectivity predicts depression stimulation response” without calibration. A better sentence is: SCC connectivity is a plausible cross-modality biomarker, with the best replicated rTMS signal around DLPFC-SCC anticorrelation, but current methods are too heterogeneous to treat the biomarker as a settled clinical rule.
Clinical Takeaway for Treatment-Resistant Depression
SCC DBS should still be described as investigational for depression. The failed 6-month Phase 3 result prevents casual optimism, and the 2026 review does not add DBS fMRI evidence because no qualifying DBS studies entered the review.1,6
The clinic-level takeaway is: use established treatments first, treat SCC-guided rTMS targeting as a promising but imperfect optimization strategy, and reserve SCC DBS for research settings or highly specialized cases where connectomic targeting and long-term monitoring are available. TUS is the watchlist modality because it can probe the same deep target noninvasively, but 3 qualifying studies are not enough to define its treatment role.
For the SCC target, the evidence now splits into 3 tiers:
- Most clinically mature: rTMS/iTBS studies using SCC-DLPFC connectivity as a targeting or prediction signal, with 21 qualifying fMRI studies in the review.
- Most mechanistically direct: SCC DBS work using tractography and intracranial recordings, scientifically important but outside the review’s qualifying fMRI evidence.
- Most experimentally flexible: TUS studies that can modulate SCC-related networks without surgery, still early at 3 qualifying studies.
Questions About SCC Stimulation for Depression
Why did a review about SCC stimulation include 0 DBS fMRI studies?
Because the review required resting-state fMRI connectivity data before or after stimulation, and DBS hardware makes that difficult. Implanted electrodes and extension wires can distort MRI signal near the target, so DBS researchers often use PET, tractography, EEG, or intracranial recordings instead.1
Does the 0-DBS finding mean SCC DBS is dead?
No. It means the Henensal review cannot be used as DBS efficacy evidence.
SCC DBS still has open-label, connectomic-targeting, and intracranial-biomarker support, but the sham-controlled BROADEN trial failed at 6 months, so the treatment remains investigational.6,7,8
What SCC connectivity result is strongest enough to affect rTMS targeting?
The best-supported rule is that DLPFC sites more strongly anticorrelated with the SCC tend to produce better rTMS outcomes. The rule is useful for research-guided targeting, but large and real-world studies show that it is not a stand-alone predictor for every patient.2,3,4
Why are TUS results not interchangeable with DBS results?
TUS and DBS both can engage SCC-related circuits, but they use different physics, doses, targets, and timescales. TUS is noninvasive and easier to study with fMRI, while DBS is implanted, chronic, and more directly adjustable.
A 5-person SCC TUS study cannot substitute for a sham-controlled SCC DBS trial.5
Why does the exact SCC coordinate matter so much?
The SCC is small, deep, and noisy on fMRI. Henensal et al. list multiple SCC seed coordinates and sphere sizes across studies, meaning different papers may not be measuring precisely the same subregion.
That weakens direct comparisons and helps explain why connectivity directions look inconsistent across protocols.1
What should a patient take from this if they have treatment-resistant depression?
The evidence does not support seeking SCC DBS as routine care. It supports asking whether an rTMS clinic uses modern targeting methods, considering established treatments such as ECT, ketamine/esketamine, and rTMS before invasive options, and viewing SCC DBS or SCC TUS as research-stage interventions unless offered through an experienced protocol.
References
- Henensal A, Attali D, Aubry JF, Plaze M. Subcallosal cingulate functional connectivity in depression: a systematic review of brain stimulation-induced changes and pretreatment connectivity predictors. Translational Psychiatry. 2026. doi:10.1038/s41398-026-03999-3
- Fox MD, Buckner RL, White MP, Greicius MD, Pascual-Leone A. Efficacy of transcranial magnetic stimulation targets for depression is related to intrinsic functional connectivity with the subgenual cingulate. Biological Psychiatry. 2012;72(7):595–603. doi:10.1016/j.biopsych.2012.04.028
- Weigand A, Horn A, Caballero R, et al. Prospective validation that subgenual connectivity predicts antidepressant efficacy of transcranial magnetic stimulation sites. Biological Psychiatry. 2018;84(1):28–37. doi:10.1016/j.biopsych.2017.10.028
- Elbau IG, Lynch CJ, Downar J, et al. Functional connectivity mapping for rTMS target selection in depression. American Journal of Psychiatry. 2023;180(3):230–240. doi:10.1176/appi.ajp.20220306
- Attali D, Tiennot T, Manuel TJ, et al. Deep transcranial ultrasound stimulation using personalized acoustic metamaterials improves treatment-resistant depression in humans. Brain Stimulation. 2025. doi:10.1016/j.brs.2025.04.018
- Holtzheimer PE, Husain MM, Lisanby SH, et al. Subcallosal cingulate deep brain stimulation for treatment-resistant depression: a multisite, randomized, sham-controlled trial. Lancet Psychiatry. 2017;4(11):839–849. doi:10.1016/S2215-0366(17)30371-1
- Riva-Posse P, Choi KS, Holtzheimer PE, et al. A connectomic approach for subcallosal cingulate deep brain stimulation surgery: prospective targeting in treatment-resistant depression. Molecular Psychiatry. 2018;23(4):843–849. doi:10.1038/mp.2017.59
- Alagapan S, Choi KS, Heisig S, et al. Cingulate dynamics track depression recovery with deep brain stimulation. Nature. 2023;622:130–138. doi:10.1038/s41586-023-06541-3
- Mayberg HS, Lozano AM, Voon V, et al. Deep brain stimulation for treatment-resistant depression. Neuron. 2005;45(5):651–660. doi:10.1016/j.neuron.2005.02.014
- Riva-Posse P, Choi KS, Holtzheimer PE, et al. Defining critical white matter pathways mediating successful subcallosal cingulate deep brain stimulation for treatment-resistant depression. Biological Psychiatry. 2014;76(12):963–969. doi:10.1016/j.biopsych.2014.03.029
- Oh J, Ryu JS, Kim J, et al. Effect of low-intensity transcranial focused ultrasound stimulation in patients with major depressive disorder: a randomized, double-blind, sham-controlled clinical trial. Psychiatry Investigation. 2024;21:885–896. doi:10.30773/pi.2024.0016