A 2026 ALSPAC analysis tested a narrow claim behind routine genetic screening for childhood attention-deficit/hyperactivity disorder (ADHD) and autism spectrum disorder (ASD): whether rare copy number variants (CNVs; deleted or duplicated DNA segments) make young-adult outcomes worse than ADHD/ASD status alone would predict. In 8,414 people with usable CNV data, ADHD and ASD predicted worse education, work, benefits, functioning, and depression outcomes than no childhood ADHD/ASD difficulties, but neurodevelopmental CNVs did not significantly moderate any estimable ADHD/ASD-outcome association.1
Research Highlights
- CNV moderation was not supported: 8,414 ALSPAC participants passed CNV quality control, but only 194 (2.3%) carried a neurodevelopmental CNV, and available interaction tests for ADHD/ASD outcomes were non-significant with p-values from 0.40 to 0.79.1
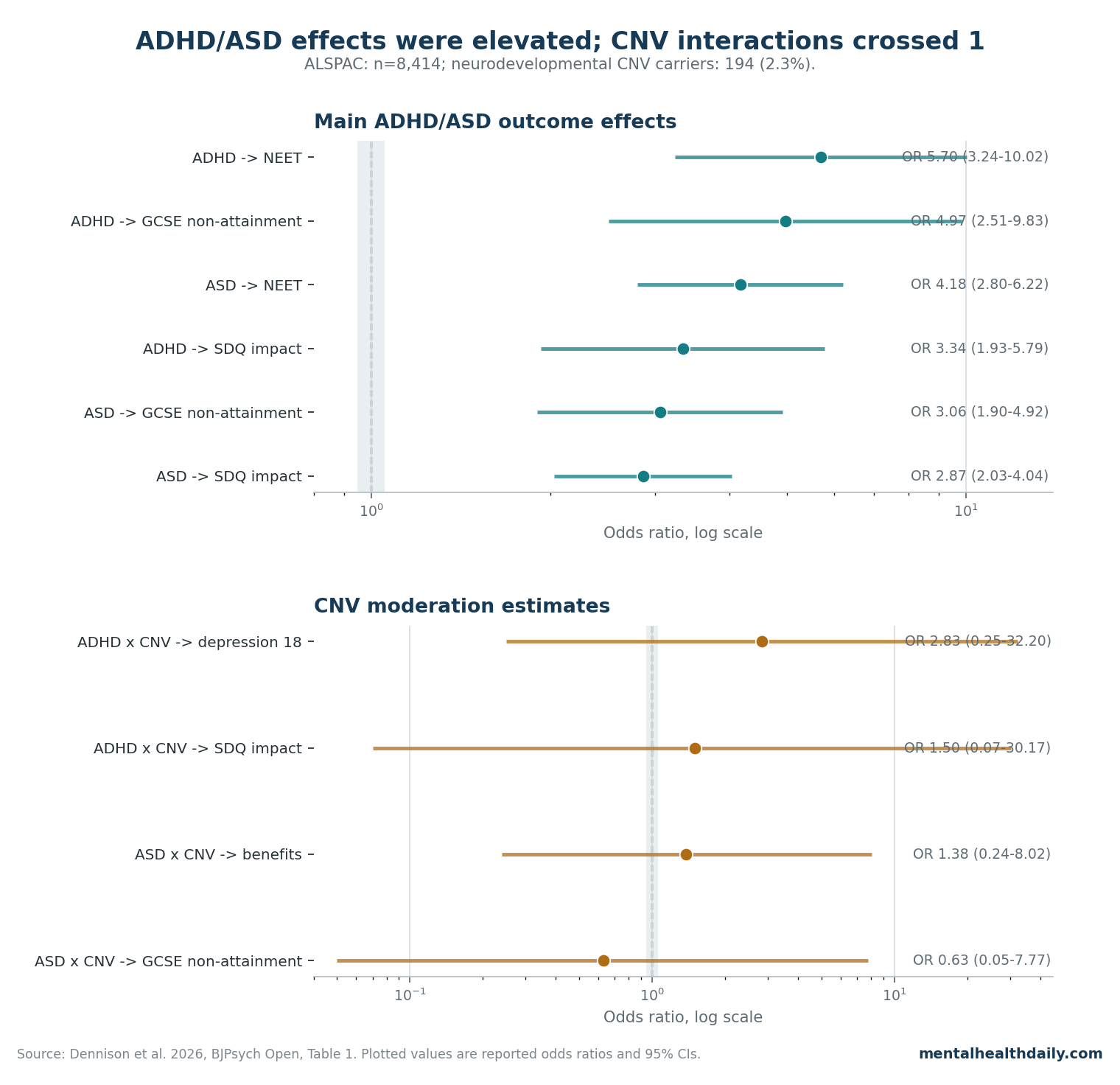
- ADHD main effects were large: childhood ADHD was associated with GCSE non-attainment (OR 4.97, 95% CI 2.51–9.83), NEET status at 25 (OR 5.70, 95% CI 3.24–10.02), and depression at 24 (OR 2.75, 95% CI 1.66–4.56).1
- Autism main effects were broad: ASD difficulties were associated with all measured outcomes, including NEET status (OR 4.18, 95% CI 2.80–6.22), SDQ impact on functioning (OR 2.87, 95% CI 2.03–4.04), and depression at 18 (OR 2.25, 95% CI 1.61–3.14).1
- The null was imprecise: available interaction CIs were extremely wide, such as ADHD x CNV for depression at 18 (OR 2.83, 95% CI 0.25–32.20) and ADHD x CNV for functioning impact (OR 1.50, 95% CI 0.07–30.17).1
- Guideline expansion is not justified by these data: UK guidance already recommends genetic testing for intellectual disability or unusual clinical features, and this 2026 cohort analysis does not show outcome-prediction value for routine CNV testing in broadly defined ADHD/ASD alone.4
The useful interpretation is calibrated, not dismissive. CNVs are real neurodevelopmental risk factors, and prior work links pathogenic CNVs to cognition, functional outcomes, and ASD treatment-response differences.6,7
Dennison et al. asked a more clinical question: if a child already has ADHD or ASD difficulties, does CNV carrier status meaningfully improve prediction of later depression, functioning, school attainment, employment/education status, or benefits receipt?
The ALSPAC answer was no strong evidence. That does not prove CNVs have no prognostic effect; the study was underpowered for rare-carrier interaction tests.
It does argue against using routine CNV screening as an outcome-prediction shortcut for non-syndromic ADHD or ASD presentations.
ALSPAC Tested Genetic Prognosis, Not Genetic Cause
ALSPAC is the Avon Longitudinal Study of Parents and Children, a UK birth cohort that enrolled pregnant women with expected delivery dates from April 1991 through December 1992 and followed their children into adulthood.9 Dennison et al. used this cohort because it combines childhood neurodevelopmental measures, genetic data, and young-adult outcomes in the same population sample.1
ADHD was defined as meeting ICD-10 criteria at ages 7, 10, 13, or 15 using the Development and Well-Being Assessment. ASD difficulties were defined by Social Communication Disorders Checklist scores above the validated threshold at ages 7, 10, 13, or 16.
The ASD exposure was therefore a trait-threshold measure, not the same thing as a clinical autism diagnosis made in a specialist clinic.
Young-adult outcomes covered several domains:
- Education: GCSE non-attainment, defined as not receiving at least 1 A* to C grade General Certificate of Secondary Education qualification by age 18.
- Mental health: ICD-10 depressive episode at ages 18 and 24, assessed with the Clinical Interview Schedule–Revised.
- Functioning: self-rated difficulties endorsed as “definite” or “severe” on the Strengths and Difficulties Questionnaire (SDQ) impact item at age 25.
- Adult role status: not in education, employment, or training (NEET) at age 25.
- Economic support: receipt of state benefits at age 25.
CNVs were called with PennCNV and filtered for technical quality. Neurodevelopmental CNVs were a predefined set of known pathogenic or susceptibility loci, while large rare CNVs were used in sensitivity analyses to broaden the genetic signal beyond the predefined neurodevelopmental list.1
Only 194 Participants Carried a Neurodevelopmental CNV
CNV rarity is the statistical pressure point. Among 8,414 participants with high-quality genetic data, 194 carried a neurodevelopmental CNV and 734 carried any large rare CNV.1
That is enough to estimate broad cohort associations, but it becomes thin when the question is an interaction: ADHD or ASD status, multiplied by CNV carrier status, predicting each young-adult outcome.
The study team used logistic regression with an ADHD/ASD x CNV interaction term. Multiple imputation handled missingness, with 200 imputed datasets.
Genetic data itself was not imputed. The imputation workup matters because young-adult outcome missingness was high before imputation: 59.5% for depression at 18, 65.4% for depression at 24, 70.8% for GCSE non-attainment, 65.8% for NEET, and 65.2% for state benefits.1
Evidence-strength note: this was an exploratory population-cohort analysis. It can test whether a moderation signal is visible in ALSPAC under the authors’ definitions.
It cannot prove individual genetic prognosis, validate a clinical screening program, or exclude smaller effects in severe clinically referred ADHD/ASD samples.
ADHD Odds Ratios Reached 5.70 for NEET and 4.97 for GCSE Non-Attainment
Childhood ADHD showed the expected long-term burden compared with no childhood ADHD difficulties.
- GCSE non-attainment: OR 4.97, 95% CI 2.51–9.83; p = 5.4 x 10−6.
- Depression at age 24: OR 2.75, 95% CI 1.66–4.56; p = 1.0 x 10−4.
- SDQ impact on functioning: OR 3.34, 95% CI 1.93–5.79; p = 2.0 x 10−5.
- NEET status at 25: OR 5.70, 95% CI 3.24–10.02; p = 3.5 x 10−9.
- Benefits receipt at 25: OR 2.86, 95% CI 1.65–4.95; p = 1.9 x 10−4.1
Depression at 18 was the exception: ADHD was not significantly associated with depression at that age (OR 1.16, 95% CI 0.58–2.33; p = 0.67). Continuous ADHD symptom scores produced the same general pattern, with higher scores associated with GCSE non-attainment, depression at 24, SDQ impact, NEET, and benefits, but not depression at 18.1
That ADHD-outcome pattern fits the adjacent literature. Di Lorenzo et al. reviewed childhood/adolescent ADHD followed into adulthood and included 39 studies qualitatively and 27 quantitatively; adult persistence averaged 43%, and long-term impairment clustered around substance/alcohol use disorders, antisocial behavior, and other functional consequences.2
Dennison et al. did not need CNVs to recover that basic prognosis signal: ADHD itself carried the outcome association.
Autism Associations Were Broad, but CNV Interaction Tests Stayed Non-Significant
ASD difficulties were associated with every young-adult outcome in the main analysis compared with no childhood ASD difficulties.
- GCSE non-attainment: OR 3.06, 95% CI 1.90–4.92; p = 5.2 x 10−6.
- Depression at 18: OR 2.25, 95% CI 1.61–3.14; p = 2.2 x 10−6.
- Depression at 24: OR 1.84, 95% CI 1.30–2.59; p = 5.5 x 10−4.
- SDQ impact: OR 2.87, 95% CI 2.03–4.04; p = 4.1 x 10−9.
- NEET at 25: OR 4.18, 95% CI 2.80–6.22; p = 9.6 x 10−12.
- Benefits receipt: OR 1.90, 95% CI 1.30–2.77; p = 9.2 x 10−4.1
Steinhausen et al. had already shown in a systematic review and meta-analysis that adolescent and adult outcomes in ASD are often poor and highly heterogeneous.3 Dennison et al. sharpened the question from “are outcomes heterogeneous?” to “does a rare CNV flag explain enough of that heterogeneity to help prognosis?”
For neurodevelopmental CNV moderation, the available categorical interaction tests did not clear that bar. ADHD x CNV was estimable for depression at 18 (interaction OR 2.83, 95% CI 0.25–32.20; p = 0.40) and SDQ impact (interaction OR 1.50, 95% CI 0.07–30.17; p = 0.79).
ASD x CNV was estimable for GCSE non-attainment (interaction OR 0.63, 95% CI 0.05–7.77; p = 0.72) and benefits receipt (interaction OR 1.38, 95% CI 0.24–8.02; p = 0.72).1
Several other categorical interaction tests could not be estimated because carrier/outcome cells were too small. Continuous ADHD and ASD symptom-score analyses were more stable, and their neurodevelopmental-CNV interaction p-values were also non-significant across outcomes.
Large rare CNV sensitivity analyses likewise did not show moderation: for ADHD, p-values ranged from 0.14 to 0.93 in imputed analyses; for ASD, p-values ranged from 0.23 to 0.96.1
CNV Evidence Supports Risk Biology More Than Routine Prognosis
CNVs are not a fringe genetic idea. Grayton et al. reviewed copy number variation across neurodevelopmental disorders, including autism, schizophrenia, epilepsy, and intellectual disability, and emphasized that pathogenic CNVs created opportunities for diagnosis, genetic counseling, risk prediction, and mechanistic discovery.8
Kendall et al. later found that pathogenic CNV carriers in UK Biobank had poorer cognitive performance and functional outcomes, supporting the idea that CNVs can carry real phenotypic burden outside childhood clinics.6
Tammimies et al. also reported that CNV status could stratify social-skills training response in ASD. In that randomized social-skills training context, carriers of large genic CNVs showed inferior parent-rated Social Responsiveness Scale outcomes after intervention and at follow-up compared with non-carriers.7
That is exactly why the Dennison hypothesis was plausible: rare variants can matter, and they may mark clinically relevant subgroups.
The ALSPAC result narrows the claim. It does not say CNVs are irrelevant to neurodevelopment.
It says CNV carrier status did not add clear moderation of broad young-adult outcomes once the analysis started with childhood ADHD or ASD difficulties in a population cohort. Etiology and prognosis are not interchangeable: a variant can increase risk for a neurodevelopmental condition without becoming a useful outcome-prediction tool for every child who meets ADHD/ASD criteria.
Genetic Testing Guidelines Still Turn on Diagnosis, Dysmorphology, and Clinical Utility
Clinical genetic testing is already recommended in some neurodevelopmental situations. UK psychiatric guidance recommends routine genetic testing for children with intellectual disability, but not for ADHD or ASD alone unless additional comorbidities, dysmorphic features, or unusual medical presentations raise suspicion for a syndromic genetic condition.4
US consensus guidance supports chromosomal microarray as a first-tier diagnostic test for developmental disabilities or congenital anomalies, and US autism practice has generally been more favorable to chromosomal microarray in ASD than the UK psychiatric guidance cited by Dennison et al.5
The guideline distinction is not anti-genetic. It is a clinical-utility threshold.
Genetic testing is easier to justify when it can explain intellectual disability, congenital anomalies, dysmorphic features, seizures, unusual medical presentations, or family recurrence risk. It is harder to justify when the only promised use is broad prognosis in ADHD/ASD and the best available population-cohort test does not show that CNV status changes outcome prediction.
For families, the practical distinction is worth keeping clean. A child with ADHD or ASD plus intellectual disability, developmental anomalies, seizures, dysmorphic features, or a strong family-history pattern belongs in a different genetic-testing conversation than a child with ADHD or ASD alone.
Dennison et al. addressed the second scenario: routine CNV screening for prognosis in broadly defined ADHD/ASD presentations.
Wide Confidence Intervals Keep Rare-CNV Prognosis Unsettled
The null finding should not be inflated into certainty. Rare CNVs make interaction analysis difficult because the clinically interesting subgroup is small.
The interaction CIs in Dennison et al. were so wide that they included small effects, no effect, and effects large enough to matter clinically.1
Attrition adds another limit. Even with multiple imputation, many young-adult outcomes had more than 59% missing data before imputation.
The authors also noted that ASD was assessed through questionnaire-based ASD difficulties rather than diagnosis, and that clinically referred samples might differ from a population cohort. Those limitations do not erase the null, but they control its force.
The clean clinical reading is therefore bounded: current ALSPAC evidence does not support routine CNV testing as a prognostic tool for non-syndromic ADHD or ASD, while larger clinical datasets are still needed to test whether specific CNVs, CNV classes, polygenic scores, or rare sequencing variants identify outcome-relevant subgroups.
Questions About CNV Testing After This ALSPAC Analysis
Did Dennison et al. find that ADHD and autism stop mattering after accounting for CNVs?
No. ADHD and ASD difficulties were strongly associated with worse young-adult outcomes.
The null finding was about CNV moderation: whether CNV carrier status changed those ADHD/ASD-outcome links in a clinically useful way.1
Did neurodevelopmental CNVs worsen outcomes among children with ADHD or ASD?
Not clearly in this cohort. Every estimable neurodevelopmental-CNV interaction was non-significant, and several tests could not be estimated because too few CNV carriers fell into the relevant cells.
That is a weak prognostic signal, not proof that CNVs never influence outcomes.1
Should this study change genetic testing for a child with ADHD plus intellectual disability?
No. The study does not undercut genetic testing when intellectual disability, dysmorphic features, congenital anomalies, seizures, unusual medical presentations, or family-history patterns raise the pretest probability of a clinically meaningful finding.
Those indications are separate from routine prognosis in ADHD/ASD alone.4,5
Why can CNVs be important biologically but weak as a prognosis tool here?
Biological risk and clinical prediction are different tasks. A CNV can contribute to neurodevelopmental liability, cognition, or treatment response in some settings, while still failing to add useful outcome prediction in a broad population cohort once ADHD or ASD difficulties are already known.6,7
What study would make the prognostic question sharper?
A larger clinically ascertained ADHD/ASD sample with deeper genetic data, clearer diagnostic phenotyping, lower outcome missingness, and enough carriers of specific CNV classes to estimate interactions without collapsing the result into very wide CIs.
References
- Dennison CA, Flanagan M, Shakeshaft A, et al. Childhood ADHD and autism spectrum disorder difficulties: exploring the impact of copy number variants on young adult outcomes. BJPsych Open. 2026;12(3):e108. doi:10.1192/bjo.2026.11018
- Di Lorenzo R, Balducci J, Poppi C, et al. Children and adolescents with ADHD followed up to adulthood: a systematic review of long-term outcomes. Acta Neuropsychiatrica. 2021;33(6):283–298. doi:10.1017/neu.2021.23
- Steinhausen HC, Mohr Jensen C, Lauritsen MB. A systematic review and meta-analysis of the long-term overall outcome of autism spectrum disorders in adolescence and adulthood. Acta Psychiatrica Scandinavica. 2016;133(6):445–452. doi:10.1111/acps.12559
- Royal College of Psychiatrists. The Role of Genetic Testing in Mental Health Settings. Royal College of Psychiatrists; 2023. Royal College report
- Miller DT, Adam MP, Aradhya S, et al. Consensus statement: chromosomal microarray is a first-tier clinical diagnostic test for individuals with developmental disabilities or congenital anomalies. American Journal of Human Genetics. 2010;86(5):749–764. doi:10.1016/j.ajhg.2010.04.006
- Kendall K, Bracher-Smith M, Fitzpatrick H, et al. Cognitive performance and functional outcomes of carriers of pathogenic copy number variants: analysis of the UK Biobank. British Journal of Psychiatry. 2019;214(5):297–304. doi:10.1192/bjp.2018.301
- Tammimies K, Li D, Rabkina I, et al. Association between copy number variation and response to social skills training in autism spectrum disorder. Scientific Reports. 2019;9:9810. doi:10.1038/s41598-019-46396-1
- Grayton HM, Fernandes C, Rujescu D, Collier DA. Copy number variations in neurodevelopmental disorders. Progress in Neurobiology. 2012;99(1):81–91. doi:10.1016/j.pneurobio.2012.07.005
- Boyd A, Golding J, Macleod J, et al. Cohort profile: the “children of the 90s” — the index offspring of the Avon Longitudinal Study of Parents and Children. International Journal of Epidemiology. 2013;42(1):111–127. doi:10.1093/ije/dys064