A 2026 analysis of 174 people with non-affective first-episode psychosis found that cognitive reserve was tied to 3 signals available near illness onset: age at onset, family history of psychosis, and polygenic liability for educational attainment. Adding the education polygenic score raised the model’s adjusted R² from 13.5% to 17.7%, a real but modest gain that argues for genetic context without turning cognitive reserve into a DNA readout.1
Research Highlights
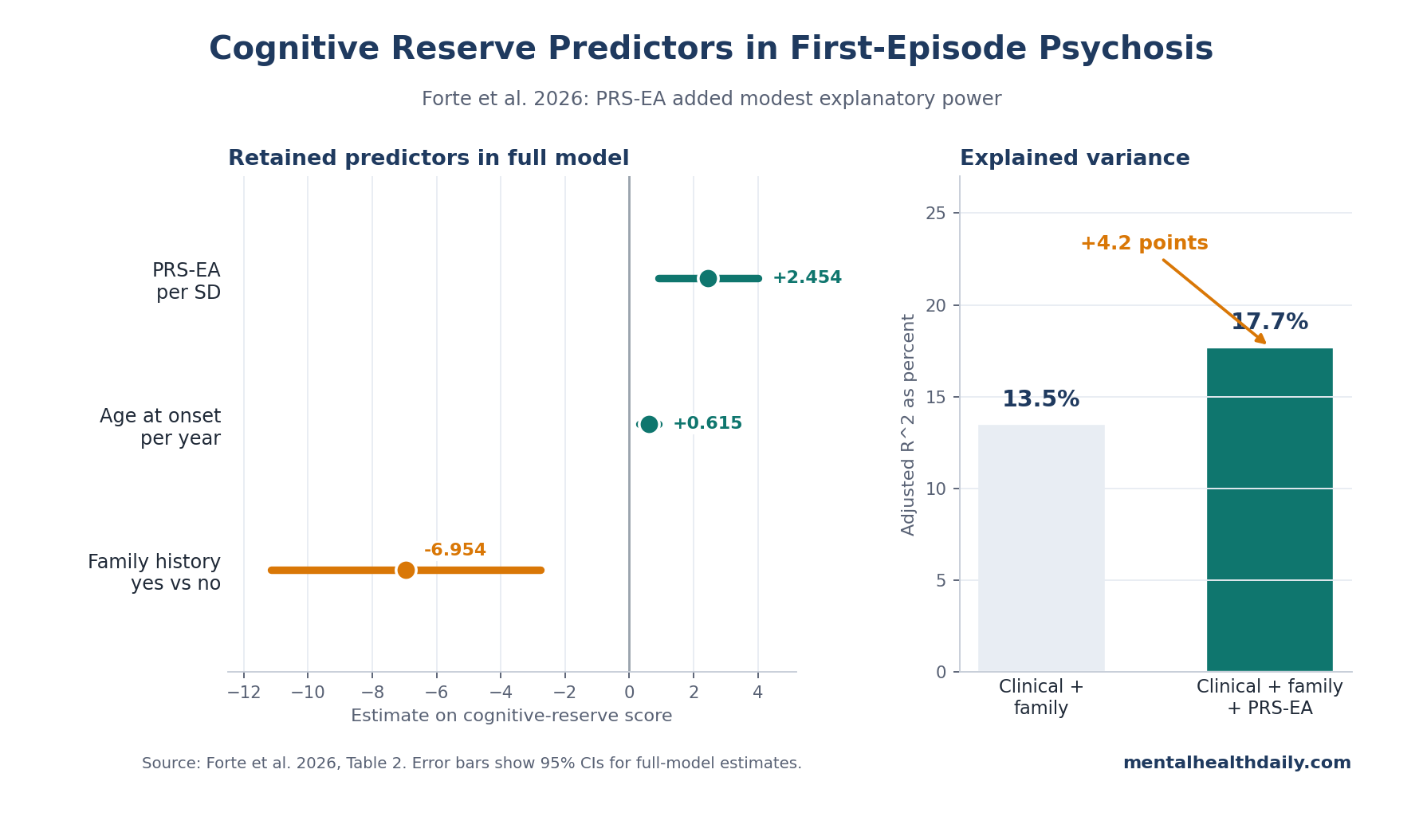
- PRS-EA added modest predictive value: the model with polygenic risk score for educational attainment, age at onset, and family history explained 17.7% of cognitive-reserve variance vs. 13.5% without PRS-EA.1
- Later psychosis onset tracked higher reserve: each additional year of age at onset was associated with a +0.615 cognitive-reserve score estimate in the full model (95% CI 0.324 to 0.905; p = 5.32 x 10^-5).1
- Family history pointed the other way: positive family history of psychosis was associated with a −6.954 cognitive-reserve estimate (95% CI −11.140 to −2.768; p = 0.00137).1
- Educational genetics beat narrower cognitive PRS: PRS for cognitive performance was significant alone (p = 0.024), but PRS-EA was the genetic term that survived the multivariable model (p = 0.002).1
- Reserve remains clinical, not deterministic: the best model left 82.3% of reserve variance unexplained, and the paper explicitly framed the genetic increment as exploratory rather than ready for clinical prediction.1
Cognitive reserve means the brain’s capacity to maintain function despite illness, injury, or developmental disruption. In psychosis research, the construct usually gets estimated from markers such as premorbid IQ, education, school performance, occupational or social engagement, and leisure activity.
Forte et al. did not show that cognitive reserve prevents psychosis, and the paper did not measure cognitive-domain trajectories after treatment. The study asked a narrower but useful upstream question: among people already presenting with non-affective first-episode psychosis, which genetic, clinical, and environmental variables help explain who has more or less reserve at baseline?1
Forte 2026: PRS-EA, Age at Onset, and Family History Predicted Reserve
The study drew from the Spanish PEPs cohort, a multicenter first-episode psychosis project. Researchers analyzed 174 people with non-affective first-episode psychosis who passed genetic quality control, were at least 16 years old, reported European ancestry, and had schizophrenia-spectrum diagnoses confirmed after follow-up.
Mean age was 25.5 years (SD 5.3), 29.3% were female, and 16.1% had a first-degree family history of psychosis.1
Polygenic risk scores (PRS) are summary measures of inherited liability for a trait, calculated by adding many small genetic associations across the genome. Forte et al. tested PRS for schizophrenia, intelligence, cognitive performance, educational attainment, occupational attainment, and physical activity.
They also tested clinical and environmental variables: age at onset, socioeconomic status, birth weight, and family history of psychosis.1
The paper’s hypothesis went beyond a generic genetics claim. Forte et al. predicted that all domains would contribute to cognitive reserve, while clinical and environmental influences would play the predominant role.
The result partially supports that prediction but does not confirm it cleanly. Age at onset and family history carried a large part of the model, yet PRS for educational attainment was the only polygenic score retained in the full multivariable model and added 4.2 percentage points of explained variance.1
Clinical Variables Explained Most Reserve Variance Before PRS-EA Was Added
The model without polygenic scores included age at onset and family history. It explained 13.5% of cognitive-reserve variance and had a root mean squared error (RMSE) of 10.508.
RMSE is a prediction-error metric: lower values mean predicted reserve scores were closer to observed scores.
Adding PRS-EA produced the full model: PRS-EA, age at onset, and family history. Explained variance rose to 17.7%, and RMSE improved to 10.220.
The extra genetic term therefore improved adjusted R² by 0.042 and RMSE by −0.288.1
That pattern is the calibrated read. The clinical/family model already did most of the measurable work, but the genetic term was not noise.
PRS-EA had an estimate of +2.454 (95% CI 0.909 to 3.999; p = 0.002), meaning higher inherited liability for educational attainment was associated with higher cognitive reserve after accounting for onset age and family history.1
Age at onset had an estimate of +0.615 per year (95% CI 0.324 to 0.905; p = 5.32 x 10^-5). Earlier onset therefore marked lower reserve, which fits a neurodevelopmental account: psychotic illness emerging earlier can interrupt schooling, social development, vocational training, and other reserve-building experiences before they have fully accumulated.1
Family history moved in the opposite direction. A first-degree family history of psychosis was associated with a −6.954 estimate on the cognitive-reserve score (95% CI −11.140 to −2.768; p = 0.00137).
That variable is not purely genetic. Family history can reflect inherited liability, but it can also capture family environment, parental functioning, stress exposure, and the developmental conditions around schooling and social engagement.1
Educational-Attainment PRS Outperformed Narrower Cognitive Scores
Univariate results looked broader than the final model. PRS for cognitive performance was associated with cognitive reserve on its own (estimate +1.936; 95% CI 0.268 to 3.604; p = 0.024).
PRS-EA was also associated with reserve (estimate +2.512; 95% CI 0.862 to 4.163; p = 0.003). PRS for intelligence, occupational attainment, physical activity, and schizophrenia did not show significant univariate associations in the main table.1
Once variables competed in the multivariable model, PRS-EA survived and PRS for cognitive performance did not. Forte et al. interpreted that as a clue about what the reserve measure was actually capturing.
Educational attainment genetics may index a wider bundle than raw test performance: sustained schooling, communication skills, persistence, social adaptation, family resources correlated with education, and access to cognitively demanding environments.
This is also why the finding should not be flattened into “education genes cause reserve.” PRS-EA is partly biological signal and partly a marker for the social machinery around education. Its association with cognitive reserve is meaningful, but the study design cannot separate inherited propensity from the environments that let that propensity turn into school years, skills, and social opportunity.
Earlier Psychosis Work Treated Reserve as Prognosis, Not a Baseline Target
The Forte paper fits a first-episode psychosis literature that has mostly used cognitive reserve to predict outcomes after illness onset. Amoretti et al. studied reserve as an outcome predictor in first-episode affective vs. non-affective psychosis, while Ayesa-Arriola et al. evaluated reserve as a moderator of 10-year outcomes across 5 first-episode psychosis clusters.2,3
Camprodon-Boadas et al. extended the same logic to 5-year follow-up in first-episode psychosis. Leeson et al. sharpened the IQ side of the issue: among 129 people with first-episode schizophrenia or schizoaffective disorder, 25% had stable low IQ, 31% had preserved average/high IQ, and 44% showed at least a 10-point IQ decline by first episode.
Over 3 years, they did not find continuing post-onset IQ decline; IQ at onset, rather than premorbid IQ alone, predicted more severe illness.4,5
That older result matters for interpreting Forte et al. Baseline reserve is more than a nostalgic estimate of pre-illness ability. In early psychosis, the reserve score sits at the collision point of inherited liability, developmental timing, family risk, schooling, social participation, and illness onset.
A low score may partly reflect vulnerability that existed before psychosis, and partly reflect opportunities disrupted as symptoms emerged.
What the Forte Analysis Cannot Prove
Cross-sectional design limits causality. Forte et al. measured associations at baseline, not changes produced by an intervention. The paper cannot prove that delaying onset, changing family context, or altering educational pathways would raise a patient’s cognitive reserve score.
The reserve score was a proxy. Cognitive reserve was built through principal component analysis using years of education, estimated premorbid IQ, school performance, leisure activity, interpersonal functioning, and parental education. Principal component analysis (PCA) is a statistical method that compresses correlated measures into a single score.
The approach is defensible, but it does not cover the full reserve construct as directly as newer instruments such as the Cognitive Reserve Assessment Scale in Health (CRASH).1,6
Generalizability is narrow. The genetic analysis was limited to self-reported European ancestry. PRS performance often shifts across ancestry groups because discovery datasets are uneven, linkage patterns differ, and educational attainment is socially structured.
A PRS-EA association in this cohort should not be treated as portable clinical prediction across populations.
Variable selection was exploratory. Stepwise Akaike Information Criterion (AIC) selection chooses predictors that optimize model fit while penalizing complexity. It can be useful, but it can also overfit a sample.
Forte et al. checked sensitivity across 14 additional imputed datasets, which helped: PRS-EA, age at onset, and family history were generally stable, while birth weight appeared only in a few sensitivity models.1
How Cognitive Reserve Should Be Used in First-Episode Psychosis
Reserve is most useful as a stratification concept. In first-episode services, a reserve profile can help clinicians and researchers ask whether a patient has enough cognitive and social scaffolding to benefit from standard early-intervention care, or whether rehabilitation needs to be more active from the start.
For a low-reserve patient, practical supports may need to be concrete: neuropsychological testing, supported education, vocational rehabilitation, cognitive remediation, family work, and help rebuilding daily structure. For a high-reserve patient, the risk is different.
Better baseline reserve can mask functional vulnerability if the person still cannot return to school, work, or social life after symptoms stabilize.
The Forte data also argue against using PRS as a shortcut. The genetic increment improved model fit, but the best model still left 82.3% of cognitive-reserve variance unexplained.
Age at onset, family history, school history, leisure activity, interpersonal functioning, and direct cognitive assessment remain the real clinical information. PRS-EA may help explain reserve architecture in research; it is not ready to replace assessment in an early psychosis clinic.1
Questions About Cognitive Reserve in First-Episode Psychosis
Did Forte et al. show that cognitive reserve prevents psychosis?
No. The study included people who already had non-affective first-episode psychosis.
It tested which variables were associated with cognitive reserve at baseline, not whether reserve prevented psychosis onset.1
Was the genetic finding large enough for clinical prediction?
No. Adding PRS-EA improved adjusted R² by 0.042 and RMSE by −0.288.
That is scientifically useful, but Forte et al. described the model as exploratory and not designed for individual clinical prediction.1
Why would later psychosis onset be linked to higher reserve?
Later onset leaves more time for schooling, social development, vocational skill-building, leisure activity, and other reserve-building experiences. Earlier psychosis can interrupt those pathways before they mature.1
Does a family history of psychosis mean low reserve is inevitable?
No. Family history was associated with lower reserve on average, but it was one predictor in a model that explained 17.7% of variance.
Most reserve variability remained outside the model, and family history itself mixes inherited and environmental pathways.1
What is the most direct clinical use of this evidence?
Measure reserve-relevant history early: education, premorbid functioning, school disruption, cognitive testing, family psychiatric history, and social engagement. Use that profile to target rehabilitation intensity, not to label a patient as genetically advantaged or disadvantaged.
References
- Forte MF, Segura AG, Serra-Navarro M, et al. Cognitive reserve in non-affective first-episode psychosis: contributions of polygenic scores, early clinical features, and environment. Psychological Medicine. 2026;56:e114. doi:10.1017/S0033291725101360
- Amoretti S, Cabrera B, Torrent C, et al. Cognitive reserve as an outcome predictor: first-episode affective vs non-affective psychosis. Acta Psychiatrica Scandinavica. 2018;138(5):441–455. doi:10.1111/acps.12949
- Ayesa-Arriola R, De La Foz VOG, Murillo-Garcia N, et al. Cognitive reserve as a moderator of outcomes in 5 clusters of first episode psychosis patients: a 10-year follow-up study of the PAFIP cohort. Psychological Medicine. 2023;53(5):1891–1905. doi:10.1017/S0033291721003536
- Camprodon-Boadas P, de la Serna E, Baeza I, et al. Cognitive reserve in patients with first-episode psychosis as outcome predictor at 5-year follow-up. European Child & Adolescent Psychiatry. 2021;30(12):1959–1967. doi:10.1007/s00787-020-01668-4
- Leeson VC, Sharma P, Harrison M, Ron MA, Barnes TRE, Joyce EM. IQ trajectory, cognitive reserve, and clinical outcome following a first episode of psychosis: a 3-year longitudinal study. Schizophrenia Bulletin. 2011;37(4):768–777. doi:10.1093/schbul/sbp143
- Amoretti S, Cabrera B, Torrent C, et al. Cognitive Reserve Assessment Scale in Health (CRASH): its validity and reliability. Journal of Clinical Medicine. 2019;8(5):586. doi:10.3390/jcm8050586