
A 2026 fMRI study of 84 medication-free adolescents found that reward uncertainty had its own phase-specific brain pattern: anxiety, depression, and anhedonia separated across different task phases and brain systems.1 The clearest clinical split was narrow but useful: anxiety tracked blunted striatum/thalamus activation during uncertain non-reward expectancy, while depression and anhedonia tracked higher visual/default-network activation during uncertain outcome resolution.
Research Highlights
- 84 adolescents completed fMRI: Liu et al. scanned 67 adolescents with current or past mood, anxiety, or related diagnoses plus 17 healthy controls while they completed a Reward Flanker Task.1
- Uncertainty slowed responses: uncertain cues produced slower reaction times than certain cues (697.88 vs. 685.73 ms; t(83) = 3.03; p = 0.003), while accuracy was not significantly different (87.26% vs. 85.99%; p = 0.06).1
- Anxiety mapped to blunted expectancy signals: higher MASC anxiety scores correlated with lower bilateral thalamus/caudate/putamen/accumbens activation during uncertain non-reward expectancy (peak T = −4.91; volume = 11,600 mm3).1
- Anhedonia mapped to outcome-resolution signals: lower TEPS scores, meaning more anhedonia, correlated with higher lateral occipital and retrosplenial/default-network activation during uncertain outcome attainment (peak T = −4.815 and −4.054).1
- Group contrasts were exploratory: mood/anxiety adolescents showed lower right caudate activation than 17 healthy controls during uncertain non-reward expectancy (peak T = 4.86), but the researchers estimated that group effects needed |d| ≥ 0.78 for 80% power.1
Reward uncertainty means not knowing whether effort will pay off or how large the payoff will be. That is different from ordinary reward anticipation, where the reward amount is known, and different from punishment uncertainty, where the unresolved outcome is threat or loss.
This distinction matters for adolescent mood and anxiety research because most reward-circuit studies ask whether depressed or anxious teens show less response to reward in general. Liu et al. asked a sharper question: what happens when the cue says “maybe reward, maybe nothing” and the adolescent has to act before the outcome is known?
How the Reward Flanker Task Isolated Uncertain Reward
The Reward Flanker Task is an fMRI task that separates cue expectancy from outcome attainment. Participants first saw a cue, completed a flanker task, and then received feedback about whether they earned money.
In this study, certain cues showed a known value: 0¢, 10¢, or 50¢. Uncertain cues showed ?¢, meaning a reward was possible but the amount was unknown.
Outcomes were predetermined and equally distributed across 0¢, 10¢, and 50¢ after both certain and uncertain cues, so the task could probe uncertainty without adding loss, punishment, or trial-by-trial learning as the main explanation.1
The analyzed sample included 84 adolescents aged 12–20 years, with a mean age of 15.3. The full sample was 62% female and psychotropic-medication-free at scanning; 56 of the 67 clinical participants were medication-naive, and 11 were medication-free after prior treatment exposure.1
- Depression severity: Children’s Depression Rating Scale-Revised (CDRS-R), with a full-sample mean of 31.93.
- Anxiety severity: Multidimensional Anxiety Scale for Children (MASC), with a full-sample mean of 41.49.
- Anhedonia: Temporal Experience of Pleasure Scale (TEPS), where lower scores mean less anticipatory or consummatory pleasure.
- Clinical diagnoses: 30 current major depressive disorder cases, 42 current anxiety disorder cases, 21 current ADHD cases, and smaller numbers with dysthymia, OCD, ODD, depressive disorder not otherwise specified, or bipolar II.
Anhedonia is reduced ability to feel pleasure or interest. Liu et al. separated anhedonia from broad depression or reward-response language by showing that lower TEPS scores were tied to a different uncertainty phase than anxiety scores were.
Uncertain Cues Slowed Responses Without Reducing Accuracy
Behaviorally, uncertainty made the task slower. Adolescents responded to flanker stimuli after uncertain cues in 697.88 ms on average, compared with 685.73 ms after certain cues.
That 12.15 ms difference was statistically significant (t(83) = 3.03; p = 0.003).1
Accuracy did not show the same reliable split. Accuracy after uncertain cues was 87.26%, compared with 85.99% after certain cues, and the difference did not reach conventional significance (t(83) = 1.91; p = 0.06).
More severe consummatory anhedonia was associated with lower accuracy before multiple-comparison correction, but those accuracy correlations did not survive correction.
The behavioral result is modest, but it keeps the imaging interpretation grounded. Uncertainty increased processing time without clearly impairing performance, so the fMRI contrasts are not easily dismissed as a simple accuracy artifact.
Uncertainty Shifted Expectancy Toward Default-Mode Activity
The default-mode network is a set of brain regions, including posterior cingulate and medial/lateral parietal regions, that tends to activate during internally focused thought, memory, self-reference, and rumination-like processing. In the whole sample, uncertain cues activated regions overlapping default-mode, somatomotor, and visual networks while suppressing fronto-parietal control regions relative to certain cues.1
During uncertain outcome expectancy, the largest positive cortical entry was right inferior parietal activation (peak T = 7.131; area = 7,332.965 mm2). Positive expectancy clusters also included right precuneus/POS1, a default-network region (peak T = 6.168; area = 752.223 mm2), plus visual and somatomotor regions.
Negative entries appeared in visual and fronto-parietal areas during the same contrast. The right lateral occipital entry had peak T = −8.236 and area = 1,698.799 mm2; right rostral middle frontal/fronto-parietal entries had peak T values of −6.338 and −6.433.1
Separate reward vs. non-reward contrasts added the key calibration: uncertain cues were not uniformly “low reward.” Fronto-striatal reward and salience networks responded in a graded pattern: certain reward > uncertain reward > certain non-reward during expectancy. That is a reward-discounting pattern, not a total absence of reward coding.
Uncertain Outcomes Activated Reward, Salience, and Visual Systems
When feedback arrived after uncertain cues, the pattern changed. Uncertain outcome attainment activated reward and salience regions, including bilateral thalamus, caudate, putamen, anterior insula, inferior frontal gyrus, dorsal anterior cingulate, posterior cingulate, visual cortex, and cerebellum.1
The largest subcortical attainment cluster covered bilateral thalamus, caudate, and putamen, with peak T = 7.42 and volume = 28,952 mm3. Other large attainment clusters appeared in cerebellar, lateral occipital, inferior parietal, fusiform, rostral middle frontal, insula, and precentral regions.
This is one reason the article should not flatten the paper into “reward circuits are blunted in anxious or depressed teens.” In the whole sample, uncertainty during feedback was strongly activating. The clinically relevant question is which phase and which symptom dimension changed that activation pattern.
Anxiety, Depression, and Anhedonia Split Across Different Uncertainty Phases
The clinically useful finding is the phase split. Anxiety was tied to the expectancy phase, especially when an uncertain cue might resolve into non-reward.
Depression and anhedonia were tied to the attainment phase, when the uncertain outcome was revealed.
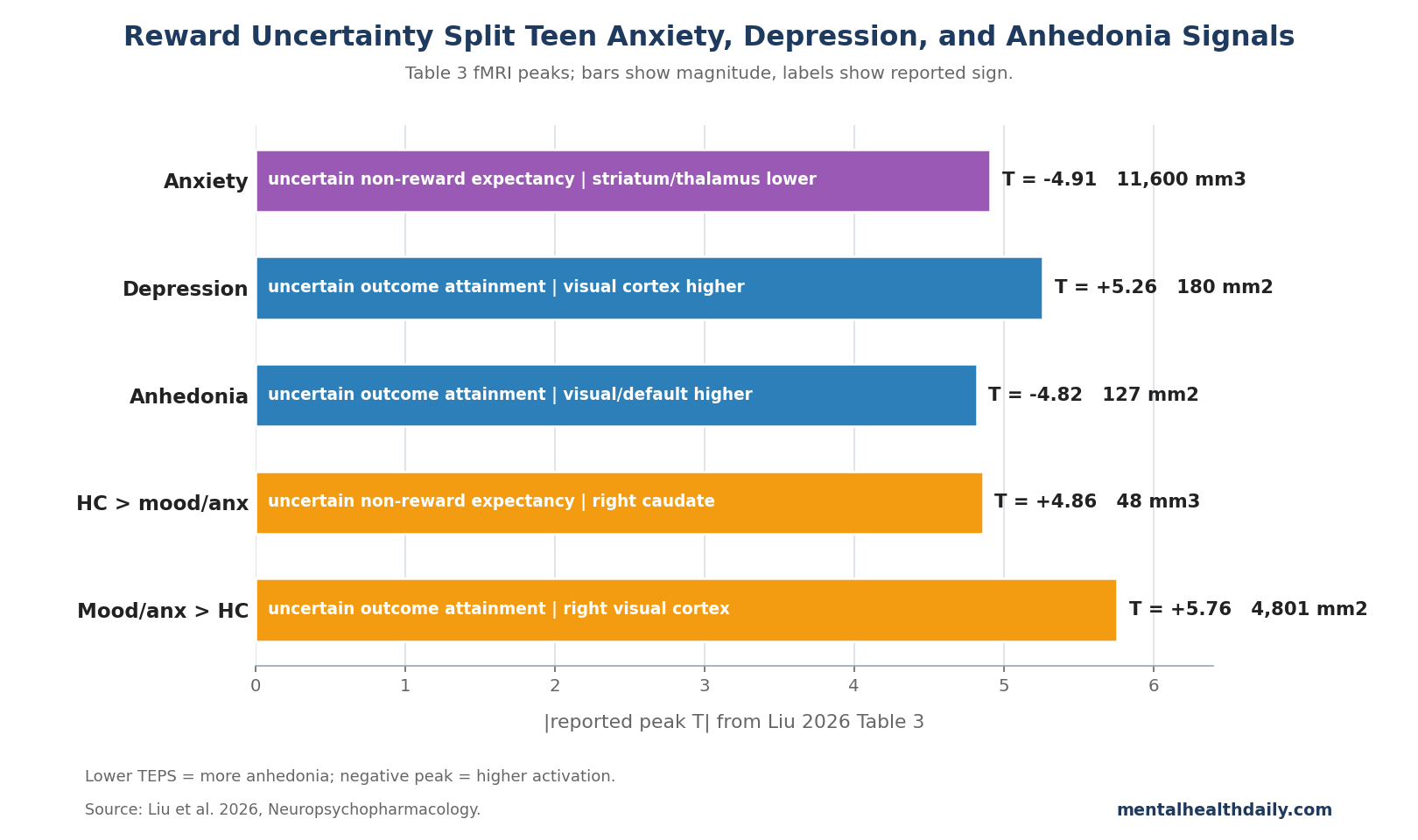
- Anxiety: higher MASC scores correlated with blunted bilateral thalamus, caudate, putamen, and accumbens activation during uncertain non-reward expectancy (peak T = −4.91; volume = 11,600 mm3). The striatum helps encode reward, salience, action selection, and prediction-learning signals, so this result points to weaker salience/reward preparation when non-reward is possible but not yet certain.1
- Depression: higher CDRS-R scores correlated with higher lateral occipital activation during uncertain outcome attainment, including a right lateral occipital cluster with peak T = 4.785 and area = 5,231.286 mm2.1
- Anhedonia: lower TEPS scores, meaning greater anhedonia, correlated with higher lateral occipital and retrosplenial/default-network activation during uncertain outcome attainment. The lateral occipital entry had peak T = −4.815 and area = 126.598 mm2; the isthmus cingulate/retrosplenial default-network entry had peak T = −4.054 and area = 144.394 mm2.1
The sign on the anhedonia result can be easy to misread. TEPS is scored so lower values mean more anhedonia.
A negative TEPS-brain correlation therefore means that greater anhedonia was associated with stronger activation in those visual/default-network regions, not weaker activation.
Mood/Anxiety Group Differences Were Exploratory, Not Diagnostic
The categorical comparison pointed in the same broad direction but was less powerful than the dimensional analysis. Compared with 17 healthy controls, the mood/anxiety subgroup showed lower right caudate activation during uncertain non-reward expectancy: HC > mood/anxiety, peak T = 4.86, volume = 48 mm3.1
During uncertain outcome attainment, the mood/anxiety subgroup showed higher activation than healthy controls in broad posterior visual regions. The largest left lateral occipital cluster had peak T = 5.16 and area = 7,130.991 mm2; the largest right lateral occipital cluster had peak T = 5.762 and area = 4,800.776 mm2.1
The researchers treated these group findings as exploratory for a good reason. Post hoc sensitivity analyses estimated 80% power to detect correlations as small as |rho| = 0.30 in the full sample, but group comparisons between the mood/anxiety subgroup and healthy controls needed effects of |d| ≥ 0.78.
That is a moderate-to-large threshold, so smaller diagnostic-group differences could have been missed.1
Generic Reward-Hyporesponsivity Misses the Uncertainty Phase Split
The adjacent literature helps calibrate the result. Earlier Reward Flanker Task work showed that this task family can map reward constructs in adolescents with diverse psychiatric symptoms, and a 2022 analysis of reward expectancy and attainment in a related dataset found phase-specific reward-function changes before this uncertainty-focused reanalysis.2,3
The broader depression literature still matters. Keren et al. reviewed fMRI and EEG reward-processing findings in depression and found that reward abnormalities are a real transdiagnostic signal, but that broad literature does not tell readers which part of uncertainty processing matters for a teenager with anxiety vs. anhedonia.4
Developmental uncertainty work also fits the result. Adolescents show distinctive tolerance for ambiguity and uncertainty during risky decision-making, and high familial risk for depression has been linked to reward-functioning abnormalities before full disorder expression in some youth samples.5,6
Liu 2026 adds a more specific fMRI claim: uncertainty during the cue phase and uncertainty during feedback resolution are not interchangeable.
The corrected framing is therefore narrower than the old draft’s featured-image logic. Anxiety mapped to blunted striatal/thalamic activation during uncertain non-reward expectancy.
Depression and anhedonia mapped to higher visual/default-network activation during uncertain outcome attainment.
What This Study Can and Cannot Support
Supported: in medication-free adolescents completing this task, reward uncertainty produced measurable phase-specific fMRI patterns, and symptom dimensions mapped to different uncertainty phases.
Not supported: a brain-based diagnostic test for teen anxiety, depression, or anhedonia. The study reports group-level and dimensional associations, not individual classification.
The healthy-control group was small, comorbidity was common, and the design was cross-sectional.
Untested: whether cognitive behavioral therapy, exposure-based uncertainty training, behavioral activation, or another intervention changes these fMRI patterns. Intolerance of uncertainty is a well-established anxiety/depression construct, but this paper did not directly measure intolerance of uncertainty or test a punishment-uncertainty condition.7,8
Clinically, the useful takeaway is conceptual rather than diagnostic: when a teen struggles with anxiety or anhedonia, “reward response” may be too broad a label. The phase of uncertainty may matter: anticipating possible non-reward is not the same brain state as resolving an uncertain outcome.
Questions About Teen Reward Uncertainty and fMRI
What did uncertain reward mean in the Reward Flanker Task?
Participants saw ?¢ instead of a fixed 0¢, 10¢, or 50¢ cue. They knew a reward was possible, but they did not know the value until feedback appeared after the flanker response.1
Did uncertain reward make teens perform worse?
Not clearly. Reaction time was slower after uncertain cues by about 12 ms, but accuracy after uncertain vs. certain cues was not significantly different (87.26% vs. 85.99%; p = 0.06).1
Was anxiety linked to stronger or weaker reward-circuit activity?
In this paper, higher anxiety was linked to weaker striatum/thalamus activation during uncertain non-reward expectancy. That is narrower than saying anxious teens have globally weak reward response or globally strong threat response.1
Why does the anhedonia result use a negative T value?
Because TEPS scores run in the opposite direction from symptom severity: lower TEPS means more anhedonia. A negative TEPS-brain correlation means greater anhedonia was associated with higher activation in the listed visual/default-network regions.1
Could this fMRI task diagnose a teenager?
No. The study is a group-level, cross-sectional imaging analysis.
It helps define a research mechanism, but it is not an individual diagnostic assay, treatment selector, or prognosis tool.1
References
- Liu Q, Nguyen TNB, Tobe RH, Stern ER, Ely BA, Gabbay V. Neural response to reward uncertainty in adolescents with mood and anxiety symptoms. Neuropsychopharmacology. 2026. doi:10.1038/s41386-026-02412-3.
- Bradley KAL, Case JAC, Freed RD, Stern ER, Gabbay V. Neural correlates of RDoC reward constructs in adolescents with diverse psychiatric symptoms: a Reward Flanker Task pilot study. Journal of Affective Disorders. 2017;216:36–45. doi:10.1016/j.jad.2016.11.042.
- Liu Q, Ely BA, Stern ER, Xu J, Kim JW, Pick DG, et al. Neural function underlying reward expectancy and attainment in adolescents with diverse psychiatric symptoms. NeuroImage: Clinical. 2022;36:103258. doi:10.1016/j.nicl.2022.103258.
- Keren H, O’Callaghan G, Vidal-Ribas P, Buzzell GA, Brotman MA, Leibenluft E, et al. Reward processing in depression: a conceptual and meta-analytic review across fMRI and EEG studies. American Journal of Psychiatry. 2018;175(11):1111–1120. doi:10.1176/appi.ajp.2018.17101124.
- van den Bos W, Hertwig R. Adolescents display distinctive tolerance to ambiguity and to uncertainty during risky decision making. Scientific Reports. 2017;7:40962. doi:10.1038/srep40962.
- Belleau EL, Kremens R, Ang YS, Pisoni A, Bondy E, Durham K, et al. Reward functioning abnormalities in adolescents at high familial risk for depressive disorders. Biological Psychiatry: Cognitive Neuroscience and Neuroimaging. 2021;6(3):270–279. doi:10.1016/j.bpsc.2020.08.016.
- Carleton RN. Into the unknown: a review and synthesis of contemporary models involving uncertainty. Journal of Anxiety Disorders. 2016;39:30–43. doi:10.1016/j.janxdis.2016.02.007.
- Grupe DW, Nitschke JB. Uncertainty and anticipation in anxiety: an integrated neurobiological and psychological perspective. Nature Reviews Neuroscience. 2013;14(7):488–501. doi:10.1038/nrn3524.