Children with intellectual disability are 3–4x more likely to have a comorbid psychiatric disorder than peers without ID. A 2026 nationwide Korean study by Joo and colleagues tracks how those rates changed across a decade.1
Research Highlights
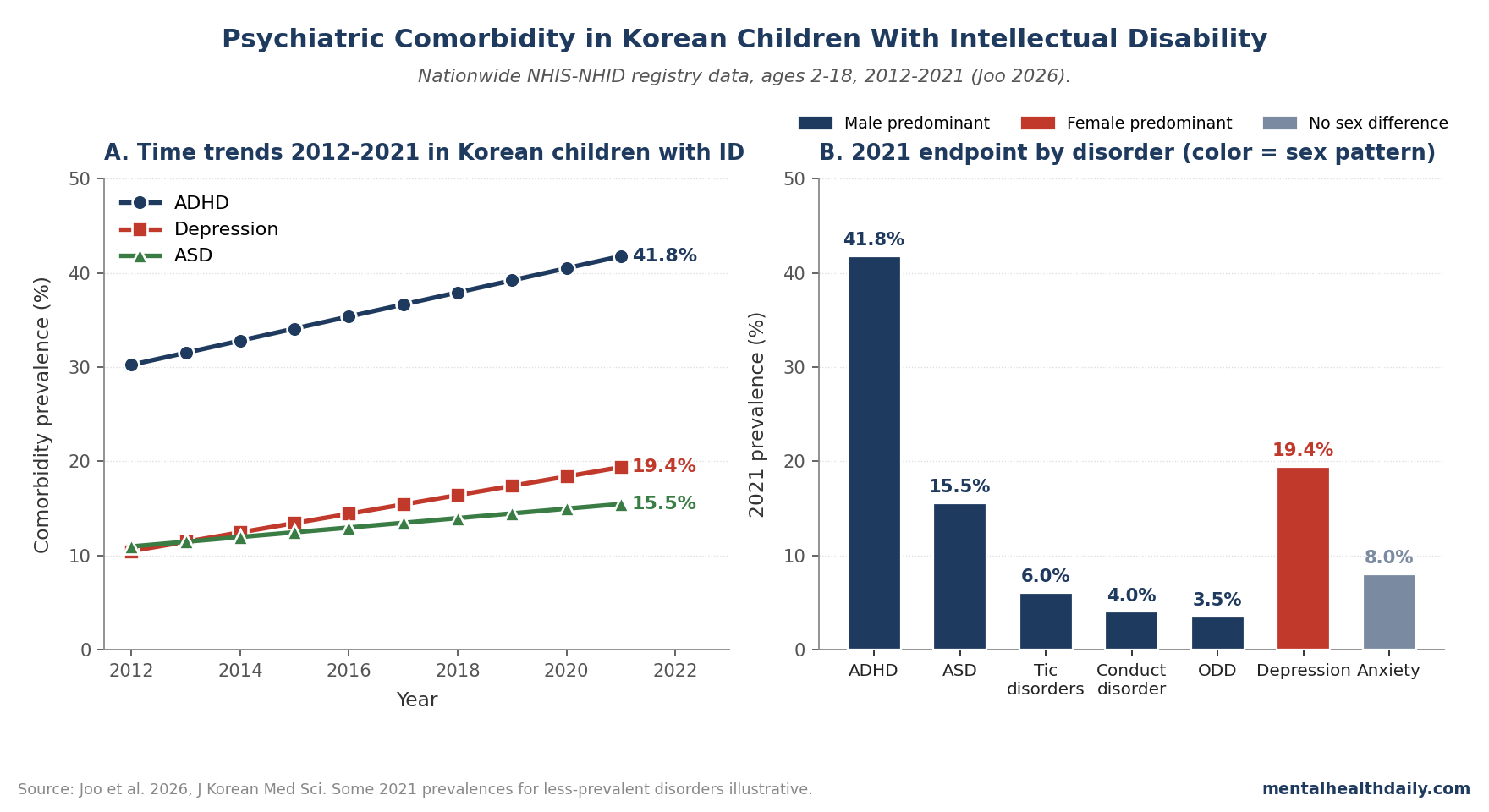
- Korean children and adolescents (ages 2–18) with intellectual disability had ADHD comorbidity rise from 30.2% in 2012 to 41.8% in 2021, depression from 10.5% to 19.4%, and autism spectrum disorder from 11.0% to 15.5% — all using nationwide National Health Insurance Service data.1
- Sex differences were significant in most diagnoses. ADHD, ASD, tic disorders, language disorders, conduct disorder, and oppositional defiant disorder showed male predominance (p < 0.001 for each); depressive disorder showed female predominance (p < 0.01); anxiety disorders showed no sex differences.1
- The rising trends partly reflect better recognition, partly real change. Korean ADHD diagnostic rates have been catching up with North American rates over the same period; the doubling of depression diagnoses in 9 years exceeds what diagnostic-recognition alone would explain.
- The clinical implication is that psychiatric comorbidity isn’t a peripheral concern in pediatric ID care — it’s the modal pattern. The 41.8% ADHD prevalence and 19.4% depression prevalence in 2021 mean a substantial majority of these patients carry at least one comorbid diagnosis.
- Population-based registry data has known limits. ICD-10-coded diagnoses depend on clinician documentation patterns, healthcare access, and screening practices. Real comorbidity rates are likely higher than the registered diagnoses capture.
Intellectual disability (ID) affects 1–3% of the population globally, and psychiatric comorbidity is the rule rather than the exception. A US population-representative sample (Platt 2019) found 65.1% of adolescents with ID met lifetime criteria for at least one psychiatric disorder.2 Despite this, research on ID-comorbid psychiatric care has been sparse compared to mainstream pediatric psychiatry, and time-trend data from non-Western populations has been particularly limited.
The Joo 2026 paper uses Korea’s National Health Insurance Service-National Health Information Database (NHIS-NHID) — which captures essentially all medical care in South Korea via single-payer billing — to track how comorbid psychiatric diagnoses in pediatric ID changed from 2012 to 2021.1 The findings document a substantial rise across multiple diagnoses, with implications both for clinical care and for understanding how psychiatric recognition is evolving in non-Western populations.
Joo 2026: Nationwide Registry, 10 Years, ID Cohort
The trigger paper used the NHIS-NHID database to identify all individuals aged 2–18 years diagnosed with intellectual disability (ICD-10 codes F70–F79.9) between 2012 and 2021 in South Korea.1 Comorbid psychiatric disorders were identified using parallel ICD-10 codes:
- ADHD: F90
- Autism spectrum disorder: F84
- Language disorder: F80
- Tic disorders: F95
- Anxiety disorders: F401–F402, F410–F411, F930–F932
- Depressive disorder: F32, F33
- Conduct disorder: F918, F928, F911
- Oppositional defiant disorder: F913
Annual prevalence of each comorbid disorder was tracked across the 10-year window, with sex stratification and chi-square testing for sex differences.
The Rises Are Substantial Across Multiple Diagnoses
Headline trends:1
- ADHD comorbidity: 30.23% in 2012 → 41.77% in 2021. Roughly 38% relative increase. Highest-prevalence comorbid diagnosis throughout the period.
- Autism spectrum disorder: 10.95% → 15.46%. Roughly 41% relative increase.
- Depressive disorder: 10.46% → 19.37%. Roughly 85% relative increase — nearly doubled.
- Anxiety disorders: Increased less dramatically across the period (specific endpoints not reported in detail).
- Other diagnoses (tic, language, conduct, ODD): Smaller absolute changes, with category-specific trajectories.
The proportional increases are large in absolute terms. By 2021, more than 4 in 10 children with ID had a documented ADHD diagnosis, and roughly 1 in 5 had a documented depressive disorder.
Sex distribution was stable across the decade: males consistently outnumbered females by roughly 2:1 (62.6–65.5% male vs. 34.5–37.4% female), consistent with the broader male predominance in pediatric ID epidemiology.3
Sex Differences Are Pronounced and Diagnosis-Specific
The sex-stratified analysis is where the paper’s clinical-pattern detail emerges. Significant sex differences appeared in most disorders:1
- Male predominance (all p < 0.001): ADHD, ASD, tic disorders, language disorders, conduct disorder, oppositional defiant disorder.
- Female predominance (p < 0.01): Depressive disorder.
- No sex difference: Anxiety disorders.
This pattern matches the broader pediatric psychiatry literature in non-ID populations.4 The fact that the same sex distribution holds in the ID population suggests psychiatric comorbidity in ID inherits the underlying epidemiologic patterns of each disorder rather than producing a uniformly different distribution.
The depression sex skew is particularly relevant for clinical attention. Adolescent female ID patients are disproportionately likely to have a comorbid depression diagnosis, which is also the diagnosis with the largest proportional rise across the decade. The combination — female-predominant condition rising fastest — argues for systematic depression screening in female adolescents with ID, a population where mood symptoms can be challenging to assess due to communication difficulties.
Why Are the Rates Rising?
Three plausible drivers deserve weight:
- Improved recognition. Korean child psychiatry has expanded substantially over the past 15 years, with growing pediatric mental health workforce and broader insurance coverage of psychiatric care.5 ADHD diagnostic rates in Korea have been catching up to North American rates over the same period — the 2012 starting prevalence of 30.2% likely reflected substantial under-recognition.
- True increase in psychiatric comorbidity. The 85% rise in depression diagnoses across 9 years exceeds what diagnostic-recognition alone typically produces. Environmental and societal factors — rising academic pressure, social media exposure, urbanization, family-structure changes — have been linked to rising adolescent depression in Korea generally.6 Children with ID may be disproportionately exposed to these stressors via mainstreaming pressure, social-comparison dynamics, and family stress.
- Diagnostic substitution. Some apparent rises may reflect re-coding of behavioral symptoms previously attributed to ID itself into specific psychiatric diagnoses. This is most relevant for ASD-ID overlap (where ID-only diagnoses in 2012 may have become ID-plus-ASD diagnoses by 2021) and conduct/ODD diagnoses.
The relative contributions of these three drivers can’t be disentangled from registry data alone. Direct symptom-prevalence surveys at multiple time points would be needed to separate true incidence change from diagnostic-recognition change.
What Popular Coverage Misses About Pediatric ID Comorbidity
Three calibrations matter when reading coverage of psychiatric trends in children with intellectual disability.
- “Diagnostic creep” framing oversells one driver. The argument that rising psychiatric diagnoses reflect inflated recognition rather than real change has merit for some categories (mild ASD, some anxiety) but is hard to sustain for depression in pediatric populations, where symptom-based prevalence surveys (independent of diagnostic codes) have also shown rises across high-income countries.7 The honest read is that both recognition and underlying prevalence have moved.
- Pediatric ID care has structural blind spots for psychiatric symptoms. Communication difficulties make symptom assessment harder; behavioral symptoms in ID are often attributed to “the ID itself” rather than to a comorbid disorder (“diagnostic overshadowing”).8 Even with the rising recognized rates, the registered diagnoses likely undercount actual prevalence by a meaningful margin.
- Treatment access is uneven. Documented diagnosis is necessary but not sufficient for treatment. Even in Korea’s universal-coverage system, evidence-based psychiatric treatment access for ID populations is patchy — specialty pediatric psychiatry training in ID is limited, and many adolescents receive symptom-targeted medication without parallel psychosocial intervention.9 The diagnostic-rate increase doesn’t automatically translate to treatment-access increase.
Limitations of the Joo Analysis
Registry-based diagnoses have known imperfections. ICD-10 codes in a billing database depend on clinician documentation, coding practices, and reimbursement incentives. Some codes are systematically over-applied (anxiety NOS) and others systematically under-applied (specific learning disorders). The reported prevalences are best read as recognized-and-recorded rates, not true population prevalences.
Cross-sectional annual snapshots, not longitudinal individual tracking. The Joo design tracks the proportion of ID patients with each comorbidity per year, not whether individual patients accumulated comorbidities over time. The patterns are population-level rather than individual-trajectory.
Korea-specific patterns may not generalize. Diagnostic culture, healthcare access, and societal pressures differ across countries. The 41.8% ADHD prevalence by 2021 is at the high end of international ID-ADHD comorbidity estimates,10 which may reflect Korean cultural patterns in ADHD recognition rather than universal pediatric ID-ADHD reality.
ID severity isn’t stratified. The F70–F79 ICD-10 range includes mild, moderate, severe, and profound ID, with very different psychiatric-comorbidity profiles. Pooling all severities masks substantial heterogeneity. Mild-ID populations have psychiatric comorbidity profiles closer to typically-developing peers; severe-profound ID populations have much higher rates of autism, motor disorders, and behavioral phenotypes that overlap with multiple psychiatric categories.
Depression diagnosis in ID populations is structurally difficult. Standard pediatric depression assessment relies on verbal self-report of mood states, sleep, appetite, and cognitive symptoms. Children with ID — particularly with moderate-to-severe ID — can’t always report these reliably, and behavioral indicators (irritability, regression, sleep disruption) overlap with multiple other conditions. The 19.4% 2021 depression prevalence in this population almost certainly reflects diagnostic patterns more than true underlying prevalence.
The trends end in 2021. COVID-19 and post-COVID adolescent mental health disruption is incompletely captured. Subsequent year data may show further acceleration or partial reversion.
Practical Implications for Pediatric ID Care
For families and clinicians involved in pediatric ID care, three practical takeaways follow.
- Psychiatric comorbidity should be the default expectation, not a peripheral concern. By 2021, a substantial majority of Korean children with ID carried at least one comorbid psychiatric diagnosis. Routine multidisciplinary care — pediatrics, child psychiatry, developmental psychology — is appropriate, with pediatric ID specialists ideally involved early rather than as referral after-the-fact.
- Depression in adolescent female ID patients deserves specific attention. The female predominance in depression and the steep rise across the decade combine to make this a high-priority screening target. Standard depression measures (PHQ-A, BDI-Y) need ID-adapted versions; specialty centers have developed these but they aren’t universal.
- ADHD treatment should be evidence-based and follow standard protocols. The 41.8% ADHD comorbidity rate in 2021 means a substantial majority of children with ID who are referred for behavioral concerns will meet ADHD criteria. Evidence-based ADHD treatment in ID populations follows the same general framework as in non-ID populations (stimulant or non-stimulant pharmacotherapy plus behavioral intervention), with attention to dose-response heterogeneity and side-effect monitoring.11
For research and policy, the implication is structural. Pediatric ID care infrastructure in many countries has been built around developmental-disability service delivery rather than integrated mental health care. The Joo data argue for restructuring that pairs developmental and psychiatric services more tightly, with shared assessment, case conferencing, and treatment-planning workflows.
FAQs: Psychiatric Comorbidity in Children With Intellectual Disability
How common is ADHD in children with intellectual disability?
Substantially more common than in the general pediatric population. The Joo 2026 Korean nationwide data show ADHD comorbidity at 41.8% in 2021 (up from 30.2% in 2012). International estimates are typically in the 30–50% range, depending on country and ID severity stratification.10 The combined prevalence is high enough that ADHD assessment should be routine in pediatric ID workup.
Why are psychiatric diagnoses rising in children with ID?
A combination of three factors: improved diagnostic recognition (Korean pediatric psychiatry capacity has expanded substantially), real increases in some conditions (depression specifically has been rising in adolescents across high-income countries), and diagnostic substitution (symptoms previously attributed to ID alone are increasingly coded as separate comorbidities). The relative contributions can’t be cleanly separated from registry data.
How do you assess depression in a child with intellectual disability?
More carefully than in typically-developing peers, because verbal self-report is limited. Specialty assessment tools include the Glasgow Depression Scale for People with a Learning Disability (GDS-LD) and the Mood, Interest and Pleasure Questionnaire (MIPQ). Behavioral indicators (irritability, withdrawal, sleep changes, appetite changes, regression in skills, increased self-injurious behavior) often substitute for verbal mood report.12 Specialty psychiatric assessment by clinicians experienced with ID is the gold standard.
Should children with ID receive psychiatric medications?
When indicated, yes — the same evidence-based principles that apply in typically-developing pediatric populations apply here, with attention to dose-response heterogeneity and side-effect monitoring. The risk is over-medication for behavioral symptoms (especially antipsychotics for irritability) when the underlying issue is environmental or communicative. Comprehensive assessment before medication, parallel behavioral intervention, and structured side-effect monitoring are all essential.11
What is “diagnostic overshadowing”?
The clinical-care pattern where presenting symptoms in a person with ID are attributed to the ID itself rather than to a separate underlying condition. Classic example: a child with ID develops anxiety after a school transition; the anxiety is framed as “behavioral symptoms of ID” rather than as a treatable anxiety disorder. Diagnostic overshadowing leads to systematic under-recognition of psychiatric comorbidity in ID populations.8 The rising recognition rates Joo documents may partly reflect reduced diagnostic overshadowing in Korean pediatric practice.
Is the rate this high in countries other than Korea?
Variable. International estimates of psychiatric comorbidity in pediatric ID range from 30–65% lifetime prevalence, depending on country, ID severity, and assessment methodology. The Joo 2026 ADHD prevalence of 41.8% is at the higher end but consistent with the broader range. US data (Platt 2019) reported 65.1% lifetime psychiatric comorbidity in adolescents with ID.2
What’s the long-term outlook?
Psychiatric comorbidity in pediatric ID populations tends to persist into adulthood and is associated with worse functional outcomes, more restrictive living arrangements, and higher caregiver burden.13 Early identification and treatment improves trajectories. Whether the rising recognition rates Joo documents will translate to better long-term outcomes depends on treatment access and quality, which lag diagnostic recognition.
References
- Time Trends in the Comorbid Psychiatric Disorders Among Children and Adolescents With Intellectual Disability in Korea: A Nationwide Study From 2012-2021. Joo MA, Kang NR, Kim JY, Lee HJ. Journal of Korean Medical Science. 2026;41(15):e126. doi:10.3346/jkms.2026.41.e126
- Adolescents with intellectual disability and comorbid mental disorders: lifetime prevalence and risk factors in a nationally representative US sample. Platt JM et al. Journal of Intellectual Disability Research. 2019;63(7):777-786. doi:10.1111/jir.12608
- Sex differences in intellectual disability: prevalence, etiology, and clinical implications. Polyak A et al. American Journal of Medical Genetics Part C. 2015;169(2):155-161. doi:10.1002/ajmg.c.31436
- Sex differences in the prevalence and clinical features of pediatric mental disorders. Hill MD et al. Pediatrics. 2017;139(2):e20162969. doi:10.1542/peds.2016-2969
- Trends in mental health service use among Korean children and adolescents. Park S, Kim BS, Kim SM. Journal of Korean Medical Science. 2022;37(46):e334. doi:10.3346/jkms.2022.37.e334
- Time trends in adolescent depressive symptoms: a nationwide analysis from Korea. Lee JH et al. European Child & Adolescent Psychiatry. 2024;33(2):501-510. doi:10.1007/s00787-023-02214-8
- National trends in mental health-related emergency department visits and hospitalizations among adolescents. Mojtabai R, Olfson M. JAMA Pediatrics. 2020;174(7):717-720.
- Diagnostic overshadowing in mental health: a critical analysis. Mason J, Scior K. Journal of Applied Research in Intellectual Disabilities. 2004;17(2):85-90. doi:10.1111/j.1360-2322.2004.00184.x
- Mental health service utilization among children and adolescents with intellectual disability: a systematic review. Buckley N et al. Journal of Intellectual Disability Research. 2020;64(1):16-30. doi:10.1111/jir.12690
- Prevalence of attention deficit hyperactivity disorder in children with intellectual disability: a systematic review and meta-analysis. Maulik PK et al. Research in Developmental Disabilities. 2021;110:103859. doi:10.1016/j.ridd.2021.103859
- Pharmacological interventions for ADHD symptoms in people with intellectual disability: a systematic review. Sun CK et al. BMC Psychiatry. 2019;19:80. doi:10.1186/s12888-019-2057-z
- Assessment of depression in adults with intellectual disabilities: a systematic review. Hermans H, Evenhuis HM. Research in Developmental Disabilities. 2010;31(6):1432-1440. doi:10.1016/j.ridd.2010.07.005
- Long-term outcomes of psychiatric comorbidity in adults with intellectual disability: a longitudinal cohort study. Cooper SA et al. The Lancet Psychiatry. 2018;5(11):880-887. doi:10.1016/S2215-0366(18)30317-1