The textbook story of social anxiety disorder is broken amygdala-prefrontal regulation — an overactive threat system the prefrontal cortex can’t calm down. A 2026 effective-connectivity study of 102 adults found something different: amygdala-prefrontal connectivity didn’t differ between social anxiety patients and controls, but connectivity between prefrontal regions did, particularly involving the pre-supplementary motor area.1
Research Highlights
- 102 adults completed an fMRI emotion-regulation task. 61 with social anxiety disorder (DSM-5 confirmed; mean Liebowitz Social Anxiety Scale 67.7) and 41 healthy controls. Participants viewed neutral and negative faces and either observed or chose their own strategy to downregulate.1
- Dynamic causal modeling (DCM) measures directed influence rather than correlation alone. Unlike standard functional connectivity, DCM estimates effective connectivity in hertz, with positive values indicating excitatory influence and negative values inhibitory.1
- Healthy controls showed the expected amygdala-vmPFC pattern. Observing negative faces produced amygdala-to-vmPFC excitation (+0.34 Hz, posterior probability 1.0) and vmPFC-to-amygdala inhibition (−0.68 Hz, posterior probability 1.0) — consistent with classical models of automatic top-down regulation.1
- Social anxiety patients did not differ from controls on amygdala-prefrontal connections. The expected fronto-amygdala dysregulation signature was absent. The differences sat entirely within prefrontal circuits.1
- The differences involved the preSMA. During observation, social anxiety patients showed stronger preSMA-to-dlPFC inhibitory connectivity than controls (−0.30 Hz). During regulation, patients showed bidirectional excitatory coupling between preSMA and vmPFC (+0.37 Hz and +0.31 Hz). Leave-one-out cross-validation showed the connectivity pattern significantly predicted diagnostic group (r = 0.24, p = 0.009).1
Social anxiety disorder (SAD) is a persistent fear of negative evaluation in social situations — lifetime prevalence around 12% in US samples — and it has been one of the most-imaged anxiety disorders for the past 2 decades.2 The dominant neural model has been straightforward: amygdala over-reacts to socially threatening cues, prefrontal cortex doesn’t inhibit it enough, the imbalance produces clinical symptoms.
That model has been built mostly on functional connectivity studies, which measure correlated activity between brain regions but cannot tell which region is influencing which. The Schrammen et al. study uses dynamic causal modeling to estimate directed connectivity, and the result challenges the simple fronto-amygdala account.
Why DCM Adds Something Functional Connectivity Cannot
Functional connectivity measures statistical correlation between activity in 2 brain regions. If amygdala and prefrontal cortex co-vary, you can call that a coupling, but you cannot tell whether one drives the other.3
Dynamic causal modeling (DCM) fits a generative model of neural activity, with each connection assigned a direction and a sign (excitatory or inhibitory) and a strength in hertz. The output is a posterior probability that each connection exists in the population, plus an estimate of how much each experimental condition modulates each connection.
A negative correlation between amygdala and vmPFC, in DCM, can decompose into either “vmPFC inhibits amygdala” or “amygdala suppresses vmPFC” (or both, asymmetrically).
Schrammen et al. modeled 5 nodes: amygdala, ventromedial PFC (vmPFC), dorsolateral PFC (dlPFC), ventrolateral PFC (vlPFC), and pre-supplementary motor area (preSMA), with bidirectional connections between all of them. Then they used parametric empirical Bayes to test how each connection’s strength was modulated by 2 task conditions: passively observing emotional faces, and actively downregulating with a self-chosen strategy.
What Healthy Controls Look Like in This Network
The healthy-control DCM provides the reference picture for what a normally functioning emotion-regulation network looks like.
During observation of negative faces:
- Amygdala → vmPFC excitatory (+0.34 Hz, posterior probability 1.0). The amygdala signals emotional salience to the vmPFC for evaluation.
- Amygdala → vlPFC inhibitory (−0.19 Hz, posterior probability 1.0). The amygdala dampens lateral PFC engagement when stimuli are mildly negative and don’t need full top-down control.
- vmPFC → amygdala inhibitory (−0.68 Hz, posterior probability 1.0). The vmPFC reciprocally dampens the amygdala — classical implicit emotion regulation.
- preSMA → amygdala excitatory (+0.52 Hz, posterior probability 1.0). The preSMA contributes to amygdala engagement, possibly reflecting attention or motor-readiness signals to salient stimuli.
During active emotion regulation, healthy controls showed broad negative modulation from the amygdala to all prefrontal regions (dlPFC −0.34 Hz, vlPFC −0.38 Hz, vmPFC −0.60 Hz, preSMA −0.54 Hz; all posterior probabilities 1.0). This was unexpected. Classical “top-down” models predict that the prefrontal cortex inhibits the amygdala during regulation; finding the reverse direction was striking.1
The interpretation Schrammen et al. propose is that with mildly negative stimuli, the amygdala is fine-tuning prefrontal engagement — preventing excessive cognitive control when it isn’t needed — rather than the prefrontal cortex commanding the amygdala. Recent meta-analyses have already pushed back on the strict top-down picture, supporting bidirectional and context-dependent dynamics.4
The Social Anxiety Differences Are All Prefrontal
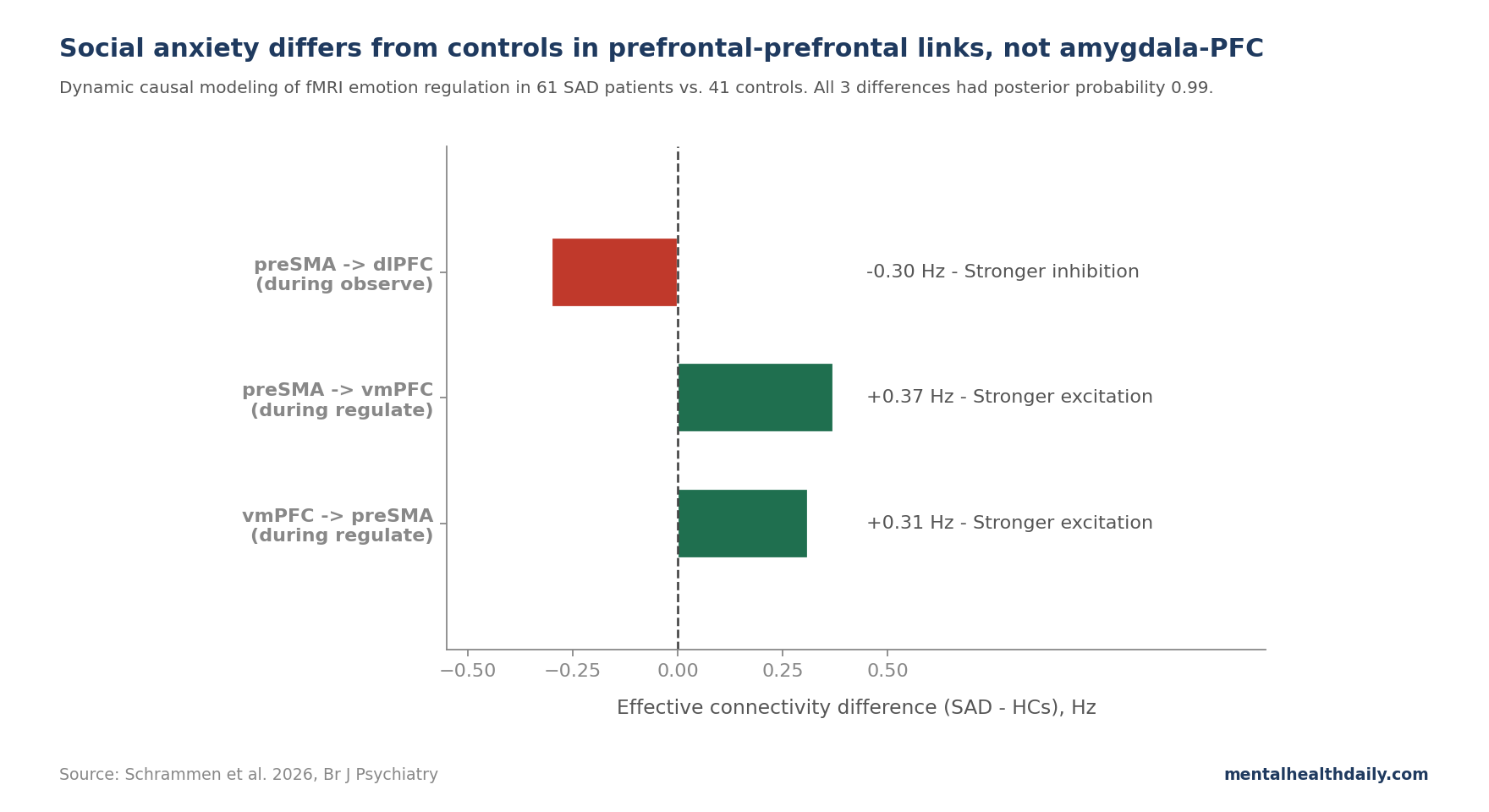
The contrast between groups produced 3 connections with strong evidence (posterior probability 0.99) for differing between social anxiety disorder patients and controls. None of them included the amygdala.
During observation of negative faces:
- preSMA → dlPFC: stronger inhibition in patients (−0.30 Hz). The preSMA pushed down on the dlPFC more in social anxiety patients than in controls when simply viewing emotional faces.
During active emotion regulation:
- preSMA → vmPFC: stronger excitation in patients (+0.37 Hz).
- vmPFC → preSMA: stronger excitation in patients (+0.31 Hz). The 2 regions were more tightly bidirectionally coupled in patients.
Leave-one-out cross-validation tested whether these 3 connectivity differences carried meaningful diagnostic information at the individual level. The pooled connectivity pattern significantly predicted diagnostic group (r = 0.24 between predicted and observed group, p = 0.009).
For symptom severity (Liebowitz Social Anxiety Scale), only the preSMA → dlPFC connection during observation was marginally predictive (r = 0.17, p = 0.048) with wide confidence intervals. For self-reported emotion regulation difficulties on the Cognitive Emotion Regulation Questionnaire, no significant prediction was found.1
What the preSMA Has to Do With Social Anxiety
The pre-supplementary motor area is traditionally a motor-planning region, but its role extends well into cognitive and affective control: conflict monitoring (when 2 response options compete), response inhibition, volitional behavioral adjustment, and preparing adaptive responses to salient stimuli.5
The Schrammen findings can be interpreted as follows:
- Stronger preSMA-to-dlPFC inhibition during simple observation in patients may reflect preemptive engagement of inhibitory control before any explicit regulation is required — a kind of premature, low-grade attempt to manage emotional responses to socially relevant stimuli, even when no instruction was given.
- Stronger bidirectional preSMA-vmPFC coupling during active regulation may reflect heightened recruitment of conflict-monitoring and behavioral-adjustment processes when explicitly regulating — a different way of doing emotion regulation, not a complete failure to do it.
Both groups successfully reduced negative ratings during regulation, and self-reported regulation success did not differ between groups (p = 0.44 for angry faces, p = 0.18 for fearful faces). The neural difference is not “patients can’t regulate” — it’s “patients regulate via different prefrontal circuits.”
Why the Amygdala-Prefrontal Story Has Been Less Consistent Than Textbooks Imply
The fronto-amygdala model of social anxiety has been built mainly on undirected functional connectivity studies. Their results have been less consistent than the model implies:
- A 2024 meta-analysis of seed-to-whole-brain functional connectivity in social anxiety disorder found no significant group effects with the amygdala as a seed region across studies, despite individual studies reporting findings.6
- A 2023 meta-analysis of fronto-amygdala connectivity in anxiety more broadly reported that effect sizes are small, heterogeneity is high, and replication across cohorts is weaker than the canonical model suggests.7
- Brühl et al. 2014 reviewed brain alterations in social anxiety and noted that the most consistent finding was amygdala hyperactivation to threat-related faces — an activation difference, not necessarily a connectivity difference.8
The Schrammen DCM result fits with this calibrated picture: amygdala-prefrontal connectivity differences in social anxiety may be real but small, inconsistent across studies, and possibly an artifact of measuring correlation rather than directed influence.
CBT and Pharmacotherapy Still Target Clinical Symptoms, Not Scan Patterns
If the right brain target in social anxiety is intra-prefrontal circuits (especially preSMA-vmPFC and preSMA-dlPFC) rather than amygdala-prefrontal regulation, the implications for treatment are subtle but worth considering:
- Cognitive-behavioral therapy already targets prefrontal processes. Cognitive restructuring, exposure with response prevention, attention training — all engage dorsal and lateral prefrontal regions. CBT works for social anxiety with effect sizes in the moderate-to-large range (SMD around 0.6–0.8 vs. waitlist).9 The neural target may match the existing intervention better than expected.
- SSRIs improve social anxiety without specifically targeting amygdala-prefrontal coupling. Furmark et al. 2002 showed that both citalopram and CBT reduced amygdala activation in social anxiety patients, but the brain changes did not correlate strongly with symptom change — consistent with the idea that fronto-amygdala biology may be less directly load-bearing than thought.10
- Neurostimulation candidates shift if the target shifts. If preSMA-vmPFC dynamics matter, that argues for stimulation protocols engaging these regions specifically, rather than the more commonly studied dorsolateral prefrontal cortex (rTMS in depression-style protocols). This is speculative; neurostimulation in social anxiety is at the early-trial stage.
- Don’t over-read 1 DCM study. A single 102-person fMRI analysis is hypothesis-strengthening, not definitive. Replication in independent cohorts using DCM with the same node selection is needed before treating intra-prefrontal connectivity as the new canonical target.
Limitations of the Schrammen Analysis
Single-site, single-task. 1 university center, 1 emotion-regulation paradigm, 1 stimulus set (Karolinska Directed Emotional Faces). Generalizability across sites, tasks, and stimulus types remains to be established.
Self-chosen regulation strategy. Allowing participants to pick their own strategy improves ecological validity but introduces variability — some used reappraisal, some used distraction, some used acceptance — and different strategies engage different prefrontal subregions. This may dilute amygdala-prefrontal differences specifically tied to reappraisal-based studies.
Mildly negative stimuli. The faces used were rated as mildly negative by controls. Stronger aversive stimuli — threat words, social-rejection scenarios, public-speaking imagery — might engage amygdala-prefrontal pathways more robustly and produce different group differences.
Mixed medication status. 18 of 61 patients were on antidepressants; healthy controls were medication-naive. Residual confounding from chronic antidepressant use is possible.
5 nodes is a simplification. Other regions implicated in emotion regulation (insula, anterior cingulate, hippocampus) were not modeled. The conclusion is “intra-prefrontal differences mattered more than amygdala-prefrontal differences in this 5-node network,” not that amygdala-prefrontal connectivity is unimportant in social anxiety.
Predictive accuracy is modest. An r of 0.24 for diagnostic group classification is statistically significant (p = 0.009) but not clinically diagnostic. The pattern carries information, but a brain scan is not yet a useful clinical tool for social anxiety.
First-Line Social Anxiety Treatment Still Starts With CBT or SSRIs
- Social anxiety disorder is real and treatable, regardless of which brain circuits matter most. CBT (especially with exposure) and SSRIs/SNRIs are first-line and well-supported. Effect sizes for CBT are moderate-to-large; SSRI response rates run around 50–65% in trials.9
- Treatment choice still rests on clinical trial evidence. The Schrammen finding leaves first-line CBT and SSRI/SNRI choices unchanged while sharpening the mechanistic account of why those treatments may work.
- Imaging findings are mechanistic, not diagnostic. A 2024 meta-analysis found no robust amygdala-seed connectivity differences in social anxiety;6 the Schrammen DCM also did not find them. A distributed, subtler brain signature fits the evidence better than a single broken amygdala-prefrontal pathway.
- If you are managing social anxiety, expect imperfect responses. Roughly 30–45% of patients do not respond fully to first-line treatment. Sequential trials, combination therapy, and adjunctive approaches (mindfulness-based therapy, attention bias modification, beta-blockers for situational performance anxiety) all have a place.
Questions About Social Anxiety, the Brain, and Treatment
So is the amygdala still important in social anxiety?
It is involved — the meta-analytic evidence for amygdala hyperactivation to threatening faces is more robust than the connectivity evidence.8 What the Schrammen DCM challenges is the more specific claim that amygdala-prefrontal connectivity is the key disrupted circuit. Activation differences and connectivity differences are different findings: the amygdala can be more reactive without the amygdala-prefrontal coupling being meaningfully different from controls.
What is dynamic causal modeling and why does it matter?
DCM estimates directed connectivity between brain regions: which region is influencing which, in which direction, and whether the influence is excitatory or inhibitory. Standard functional connectivity only measures correlation, which cannot distinguish those directions.3 It matters because clinical models of psychiatric disorders often invoke specific causal stories that correlation alone cannot test.
What treatments work best for social anxiety?
Cognitive-behavioral therapy with exposure (CBT) is the most evidence-supported psychological treatment, with moderate-to-large effect sizes (SMD around 0.6–0.8) vs. waitlist control.9 SSRIs (paroxetine, sertraline, escitalopram), SNRIs (venlafaxine), and pregabalin all have approval or evidence.
For specific performance situations (public speaking, musical performance), beta-blockers like propranolol can reduce physical symptoms acutely but do not treat the underlying disorder. Brain imaging remains a research and mechanism tool; clinical diagnosis stays with DSM-5 criteria and validated scales like the Liebowitz Social Anxiety Scale.
Can mindfulness or meditation help?
Mindfulness-based stress reduction and mindfulness-based cognitive therapy have RCT evidence in social anxiety, generally smaller effect sizes than full CBT but reasonable for patients who prefer them or use them adjunctively. Goldin & Gross 2010 reported that mindfulness-based approaches engaged different prefrontal-attentional circuits than CBT, with overlapping clinical benefit.11
How does this study change anything for patients?
Practically, very little. First-line recommendations (CBT and/or SSRI) are unchanged. The study reframes the mechanism those treatments may be acting on — possibly intra-prefrontal control circuits more than amygdala downregulation. For patients who have wondered if something is fundamentally broken in their amygdala based on popular brain-science writing, the brain differences in social anxiety are distributed across multiple regions and not reducible to a single overactive structure.
References
- Altered prefrontal effective connectivity during emotion regulation in social anxiety disorder. Schrammen E et al. British Journal of Psychiatry. 2026. doi:10.1192/bjp.2026.10628
- Lifetime prevalence and age-of-onset distributions of DSM-IV disorders in the National Comorbidity Survey Replication. Kessler RC et al. Archives of General Psychiatry. 2005;62(6):593-602. doi:10.1001/archpsyc.62.6.593
- Dynamic causal modelling. Friston KJ, Harrison L & Penny W. NeuroImage. 2003;19(4):1273-1302. doi:10.1016/S1053-8119(03)00202-7
- A meta-analysis on the neural correlates of emotion regulation. Berboth S & Morawetz C. Neuropsychologia. 2021;153:107767. doi:10.1016/j.neuropsychologia.2021.107767
- The pre-supplementary motor area as a key node for response inhibition and conflict monitoring. Nachev P, Kennard C & Husain M. Nature Reviews Neuroscience. 2008;9(11):856-869. doi:10.1038/nrn2478
- Functional brain alterations in social anxiety disorder: a meta-analytic seed-to-whole-brain connectivity analysis. Cremers HR et al. Translational Psychiatry. 2024;14:78. PubMed
- Disrupted fronto-amygdala connectivity in anxiety: a meta-analysis. Lago T et al. Neuroscience & Biobehavioral Reviews. 2017;73:80-88. doi:10.1016/j.neubiorev.2016.12.017
- Neuroimaging in social anxiety disorder: a meta-analytic review. Bruhl AB, Delsignore A, Komossa K & Weidt S. Neuroscience & Biobehavioral Reviews. 2014;47:260-280. doi:10.1016/j.neubiorev.2014.08.003
- Psychological and pharmacological interventions for social anxiety disorder in adults: a systematic review and network meta-analysis. Mayo-Wilson E et al. The Lancet Psychiatry. 2014;1(5):368-376. doi:10.1016/S2215-0366(14)70329-3
- Common changes in cerebral blood flow in patients with social phobia treated with citalopram or cognitive-behavioral therapy. Furmark T et al. Archives of General Psychiatry. 2002;59(5):425-433. doi:10.1001/archpsyc.59.5.425
- Effects of mindfulness-based stress reduction (MBSR) on emotion regulation in social anxiety disorder. Goldin PR & Gross JJ. Emotion. 2010;10(1):83-91. doi:10.1037/a0018441