A 97-dyad adolescent fMRI study found that trauma-exposed youth with high posttraumatic stress symptoms did not use parent-observed safety learning in the usual way: their arousal rose to a safety cue during vicarious extinction, F(1,159) = 4.81, p = 0.029, and parent-child physiological synchrony no longer predicted lower skin conductance during early safety learning.1 The useful interpretation is not that synchrony is always harmful; it is that trauma may change whether a parent’s body-state signal helps an adolescent downshift threat.
Research Highlights
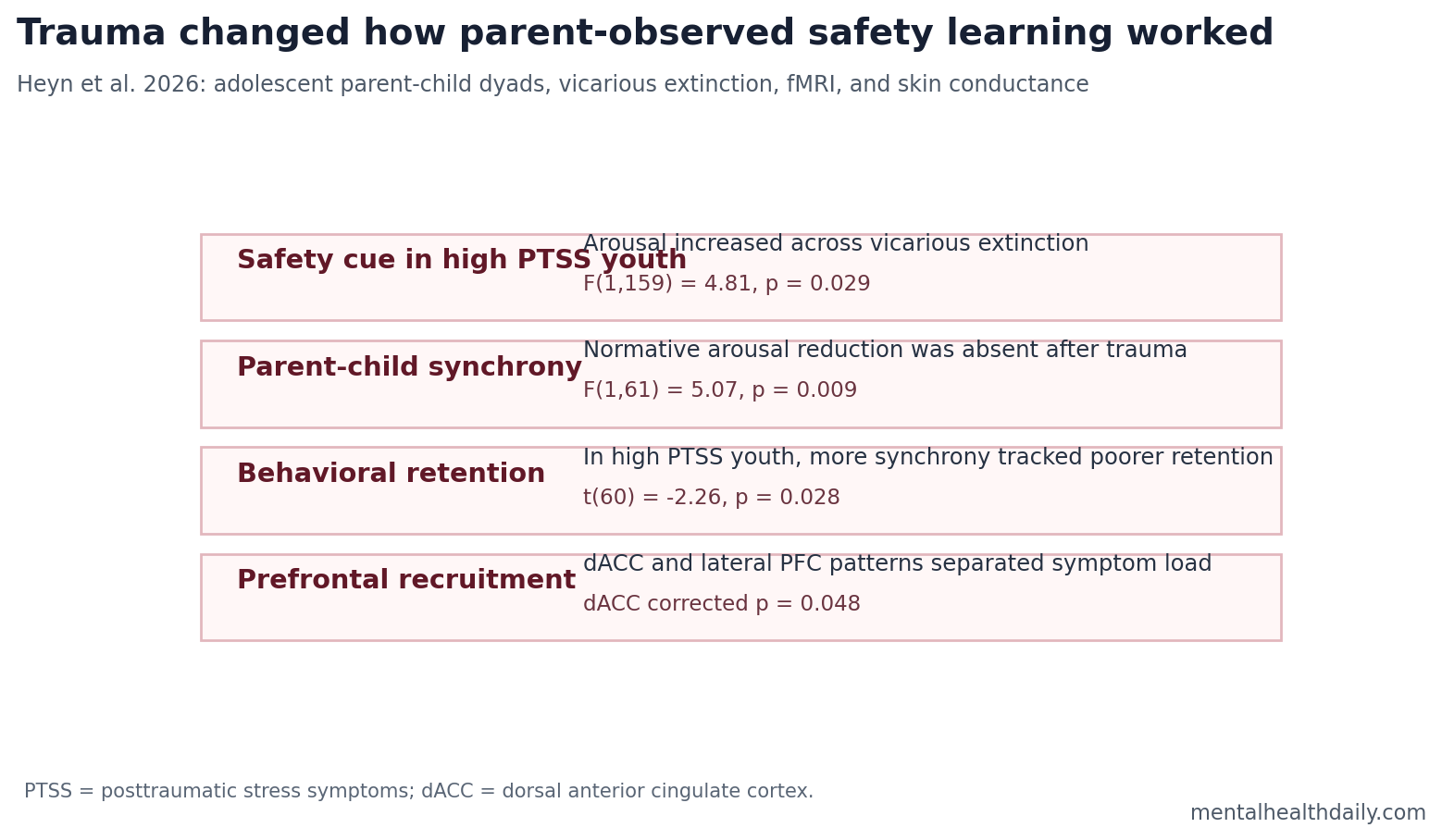
- High-symptom youth showed safety-cue arousal: During vicarious extinction, trauma-exposed youth with high PTSD symptoms had increasing skin conductance to the safety cue, F(1,159) = 4.81, p = 0.029.1
- Synchrony stopped working normally after trauma: The usual inverse link between parent-child autonomic synchrony and youth arousal was present in typically developing youth but absent in both trauma-exposed groups, F(1,61) = 5.07, p = 0.009.1
- Behavioral retention moved in the wrong direction: In high-symptom trauma-exposed youth, stronger synchrony was associated with lower behavioral retention of vicarious extinction than weaker synchrony, t(60) = -2.26, p = 0.028.1
- Prefrontal recruitment separated symptom load: Vicarious extinction produced group effects in dorsomedial PFC, dorsal anterior cingulate cortex, caudate/nucleus accumbens, and parietal regions, with dorsal anterior cingulate cortex reaching corrected p = 0.048.1
- This is a developmental mechanism study: The paradigm measured laboratory fear learning across 3 days, not treatment response, PTSD diagnosis, or real-world parent behavior quality.
Vicarious extinction means learning that a cue is safe by watching someone else go through extinction, rather than by directly experiencing repeated safe exposures. In this study, adolescents watched a video of their own parent completing direct extinction, while the youth underwent fMRI and skin-conductance recording.1
Posttraumatic stress symptoms (PTSSs) are intrusion, avoidance, arousal, mood, and cognition symptoms after trauma exposure. Heyn et al. split trauma-exposed youth into low- and high-symptom groups using the UCLA PTSD Reaction Index; the high-symptom group averaged 26.8 vs. 5.0 in the low-symptom trauma group and 5.4 in typically developing youth, p < 0.001.1
87 Parent-Child Dyads Completed a 3-Day Threat-Learning Paradigm
The study enrolled 97 youths aged 10-14 years with a primary caregiver. A total of 87 parent-child dyads at least partially completed the paradigm. Groups were typically developing youth, trauma-exposed youth with low PTSD symptoms, and trauma-exposed youth with high PTSD symptoms.1
- Day 1: youth and parents completed threat acquisition, where some colored lamp cues were paired with an aversive shock.
- Day 2: youth completed direct extinction and vicarious extinction by observing the parent complete direct extinction.
- Day 3: youth completed extinction recall and reinstatement, allowing the researchers to test whether safety learning held.
Skin conductance response (SCR) is a sweat-gland-linked marker of autonomic arousal. It is useful in fear-learning work because it changes when the body treats a cue as threatening even when a person can verbally describe the cue as safe.
Safety Cues Became Arousing in High-Symptom Trauma-Exposed Youth
Typically developing youth and low-symptom trauma-exposed youth showed stable or decreasing arousal across vicarious-extinction trials. High-symptom trauma-exposed youth decreased arousal to the previously threatening observed cue, but their arousal increased with each presentation of the safety cue, F(1,159) = 4.81, p = 0.029.1
Clinical translation: the body-level problem was impaired danger-safety discrimination in a social-learning context. The high-symptom youth treated the safety cue as arousing instead of using it as a calm-down signal.
Adult PTSD extinction studies often emphasize amygdala hyperreactivity and prefrontal regulatory problems during threat acquisition, extinction, and recall.3 Heyn et al. added a developmental layer: adolescents learned from direct cue exposure and from a parent’s visible safety experience.
Parent-Child Synchrony Was Not Automatically Protective
Autonomic synchrony means coordinated physiological change between parent and child. In typically developing youth, stronger synchrony with the parent during early vicarious extinction was linked to lower youth arousal to the observed threat cue. Trauma-exposed youth did not show that normative inverse relationship, F(1,61) = 5.07, p = 0.009.1
For high-symptom trauma-exposed youth, synchrony also related to worse behavioral extinction retention. The group-by-synchrony interaction was significant, F(2,58) = 3.67, p = 0.03, and the high-symptom group showed a negative association between synchrony and retention, t(60) = -2.26, p = 0.028.1
Calibrated read: the study does not show that parent-child synchrony is bad. It shows that after trauma, synchrony may no longer carry the same safety-learning function. A physiologically connected parent-child pair can still fail to produce a body-level reduction in threat response if the shared signal is arousal rather than regulation.
Prefrontal Timing Changed During Parent-Observed Safety Learning
During vicarious extinction, group differences appeared in right caudate/nucleus accumbens, parietal cortex, bilateral dorsomedial prefrontal cortex, and dorsal anterior cingulate cortex. The dorsal anterior cingulate effect survived false-discovery correction, F(2,282) = 5.98, corrected p = 0.048.1
Ventrolateral PFC is a lateral prefrontal region involved in interpreting emotional information and assigning meaning to others’ states. Typically developing youth showed high early ventrolateral PFC recruitment that dissipated over time, while trauma-exposed youth showed stable or increasing recruitment.
Dorsolateral PFC is involved in cognitive control and effortful processing. In high-symptom trauma-exposed youth, dorsolateral PFC activation started low and increased during vicarious extinction, t(56) = 2.32, p = 0.02. That late recruitment may be compensatory, but in this study it traveled with worse extinction retention rather than better learning.1
What This Means for PTSD Development Research
Fear-extinction models of PTSD have often focused on the individual’s amygdala, ventromedial PFC, and hippocampus.3 Adolescent trauma also unfolds inside caregiver learning environments. Children and teenagers often learn safety, threat, and emotional regulation through caregivers, and the caregiver’s physiological state becomes part of the learning environment.
Adjacent developmental studies of pediatric anxiety and threat learning also point to altered prefrontal recruitment during fear acquisition and regulation.4 Heyn et al. narrow the question: the disruption may appear when safety is socially transmitted through a caregiver, alongside safety learned alone.
What the Study Can and Cannot Support
Supported: trauma exposure and PTSD symptom load were associated with altered safety-cue arousal, disrupted synchrony-arousal coupling, and different prefrontal recruitment during parent-observed vicarious extinction.
Not supported: diagnosing PTSD from fMRI, blaming parents for adolescent PTSD symptoms, or assuming that more parent-child synchrony is always better. The design was observational, and trauma load was higher in the high-symptom group, although the significant group effects remained after controlling for cumulative trauma load.1
Best next test: longitudinal work should ask whether these dyadic extinction markers predict symptom persistence, treatment response, or improvement after family-based and exposure-based interventions.
The developmental timing is the reason the finding is more than an adult PTSD replication. Adolescents are still learning threat, safety, and self-regulation inside family systems, so parent-observed extinction can test a social-learning layer that individual fear-conditioning tasks miss. A parent who models calm during safety learning may help some youth downshift arousal, but the 2026 data suggest trauma and symptom severity can change whether that physiological signal is usable.
Clinical interpretation: the result points toward measurement rather than blame. Family-based PTSD treatment already works with caregiver responses, avoidance, and reassurance patterns, but this study does not say that parents caused the altered extinction profile.
It says the laboratory safety-learning process looked different in trauma-exposed youth with high symptoms, which is a plausible target for future therapy-mechanism studies.
Skin conductance: the autonomic findings anchor the social-learning claim in physiology rather than only in self-report. Skin conductance measures sweat-gland-linked arousal, so rising response to a safety cue suggests the body is still treating the cue as salient or threatening.
In high-symptom youth, that pattern makes the “safe” signal less reassuring. It also explains why symptom severity, trauma exposure, and parent-child synchrony need to be modeled together instead of treated as separate boxes.
The safest interpretation is mechanism-generating, not practice-changing. The study gives researchers a candidate pathway to test: trauma may alter how adolescents use caregiver-observed safety cues during extinction. It does not yet tell clinicians to select one therapy over another.
Therapy relevance: exposure-based PTSD care depends on learning that a feared cue can become safe under new conditions. If some trauma-exposed youth show rising arousal to a modeled safety cue, therapy studies need to ask whether caregiver involvement changes extinction learning, avoidance, or between-session retention.
That question is especially important for adolescents because parents often shape attendance, reassurance, sleep routines, and post-session recovery. The 2026 study does not test treatment, but it gives future trials a set of measurable targets: safety-cue arousal, parent-child physiological synchrony, and prefrontal recruitment during social safety learning.
Questions About Parent-Child Fear Extinction
Does this prove that parent behavior causes PTSD symptoms?
No. The study measured parent-child physiological coupling and youth neural responses during a laboratory task. It cannot separate inherited risk, trauma severity, parent distress, family context, and youth symptom burden into one causal chain.
Why does vicarious extinction matter?
Adolescents often learn safety by watching trusted adults navigate threat. If trauma changes how that social safety signal is encoded, exposure-based learning may need more explicit support for discrimination between danger and safety.
Is the finding ready for clinical use?
No. It is a mechanistic fMRI and physiology study. Its value is in clarifying one developmental pathway that may help future studies design better PTSD-risk and treatment-response measures.
References
- Heyn SA, DiMaio S, Herringa RJ. Neurobiological signatures of dyadic transmission of fear extinction in adolescent trauma exposure and posttraumatic stress. Biological Psychiatry: Global Open Science. 2026;6:100714. doi:10.1016/j.bpsgos.2026.100714
- Herringa RJ, et al. Parent-child vicarious extinction learning and adolescent safety learning. PubMed
- PTSD fear-conditioning and extinction meta-analysis literature. PubMed
- Pediatric anxiety threat-learning fMRI literature. PubMed
- Family functioning and pediatric posttraumatic stress literature. PubMed