A 2026 meta-analysis of 32 randomized trials involving 2,669 participants found that ultrasound-guided acupotomy reduced chronic spinal musculoskeletal pain, with pain intensity improving by SMD = −0.80 and disability by SMD = −0.99 on NDI/ODI measures.1 The direction is favorable, but all trials came from China and evidence certainty stayed moderate for pain and low for several other endpoints.
Research Highlights
- 32 RCTs were pooled: the review included 2,669 participants with cervical spondylosis, lumbar disc herniation, cervicogenic headache, ankylosing spondylitis, and related spinal disorders.1
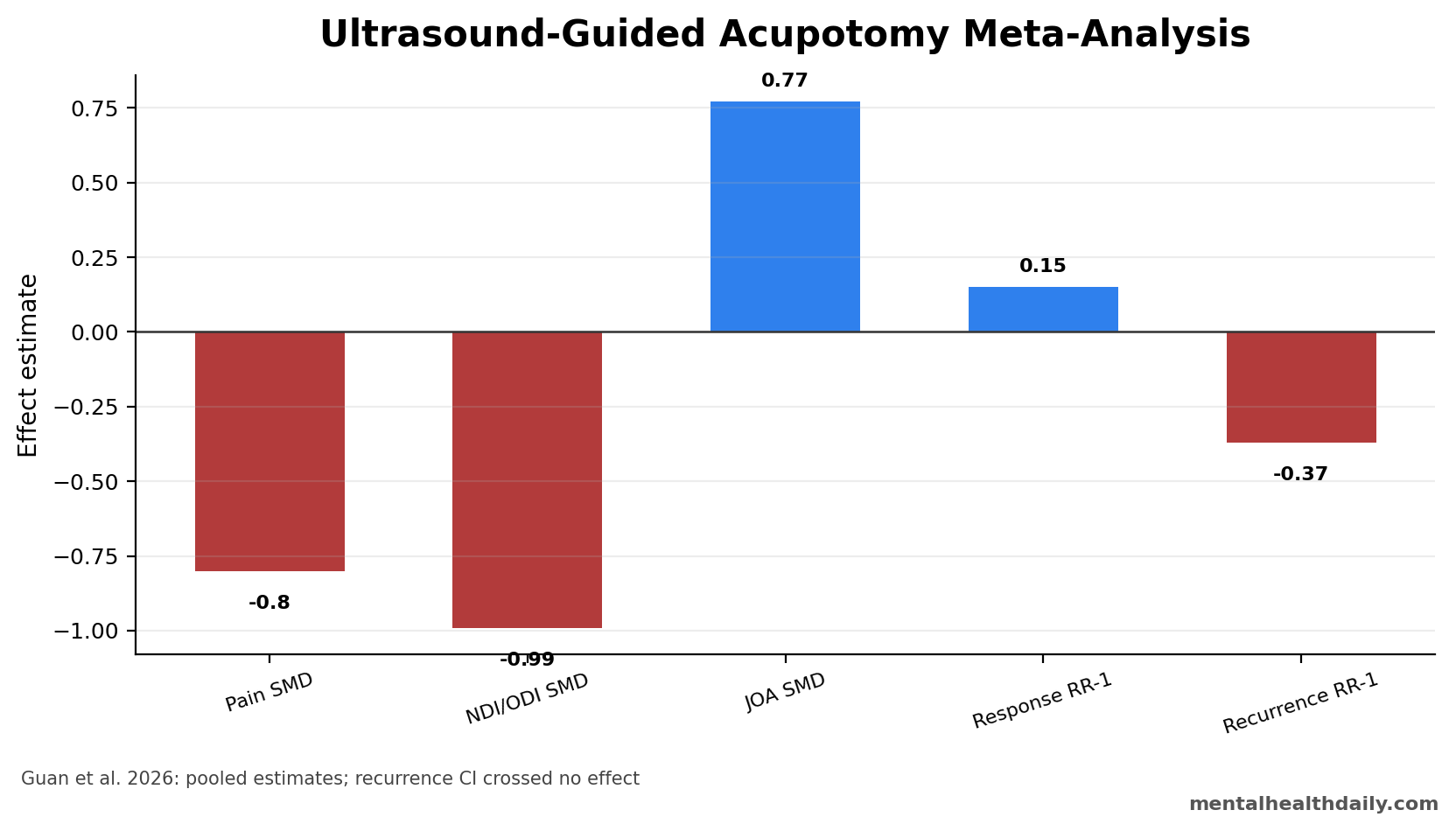
- Pain improved: visual-analog pain scores favored ultrasound-guided acupotomy with SMD = −0.80 (95% CI −0.97 to −0.64).1
- Disability improved: NDI/ODI outcomes favored treatment with SMD = −0.99 (95% CI −1.36 to −0.63), while JOA scores improved with SMD = 0.77.1
- Response rate increased: overall clinical response favored ultrasound-guided acupotomy with RR = 1.15 (95% CI 1.12 to 1.19).1
- Recurrence was uncertain: RR = 0.63 had a wide 95% CI from 0.27 to 1.43, so recurrence reduction was not statistically confirmed.1
Acupotomy is a minimally invasive needle-knife technique used to release soft-tissue adhesions or mechanically irritated structures. Ultrasound guidance adds real-time imaging so the operator can see tissue planes, vessels, nerves, and target depth during the procedure.
The clinical question is narrow: whether image-guided acupotomy adds useful pain and function benefit for chronic spinal musculoskeletal pain, not whether every chronic pain patient should receive it.
VAS Pain Improved by SMD = −0.80 Across 32 Trials
Guan et al. searched major English and Chinese databases through August 2025 and included randomized controlled trials of ultrasound-guided acupotomy for chronic spinal musculoskeletal pain. Conditions ranged from cervical spondylosis and lumbar disc herniation to cervicogenic headache and ankylosing spondylitis.1
Standardized mean difference (SMD) is used when studies measure the same concept on different scales. A negative SMD for VAS pain means the treated groups reported lower pain than comparison groups.
The pooled pain result was SMD = −0.80, with a 95% confidence interval from −0.97 to −0.64. That is a moderately large pooled signal, and the confidence interval did not cross 0.
Function and Clinical Response Moved in the Same Direction
Disability outcomes also favored ultrasound-guided acupotomy. The Neck Disability Index/Oswestry Disability Index pool was SMD = −0.99, and Japanese Orthopaedic Association score improvement was SMD = 0.77. Overall response rate favored treatment with RR = 1.15.1
Reader translation: pain and disability improved in the same direction, which makes the result more plausible than a pain-only signal. A response-rate RR of 1.15 means response was 15% more likely in the treatment groups than in the controls.
Recurrence was less settled. The point estimate favored ultrasound-guided acupotomy, but RR = 0.63 had a wide interval from 0.27 to 1.43. That interval includes both meaningful recurrence reduction and no reliable effect.
The disability result is clinically useful because chronic spinal pain is rarely just a pain-intensity problem. Neck Disability Index and Oswestry Disability Index scores try to capture daily movement, lifting, walking, sitting, sleep, personal care, and work limits. A procedure that lowers pain but leaves function unchanged is less persuasive than one that moves both endpoints in the same direction.
Comparator caution: the pooled response-rate result came from varied control conditions, not one uniform comparator. The included trials compared different background treatments, different spinal diagnoses, and different add-on combinations. That makes the positive direction harder to dismiss, but it also means the pooled number should be read as a mixed-comparator estimate rather than one clean head-to-head trial.
- Most persuasive signal: pain, disability, JOA score, and response rate all favored treatment.
- Least settled signal: recurrence reduction stayed statistically uncertain because the 95% CI crossed 1.
- Practical uncertainty: the review does not identify which diagnosis, technique, operator experience level, or control treatment explains the largest share of benefit.
All 32 Trials Came From China
The major limit is not hidden. Every included randomized trial was conducted in China, and the authors graded evidence quality as moderate for pain and response rate but low for other outcomes. Lack of blinding, heterogeneity, and protocol variation all weaken generalizability.1
Add-on signal: subgroup analysis suggested the strongest performance when ultrasound-guided acupotomy was added to other care. That matters because add-on trials can overstate what a procedure would do as a stand-alone intervention.
Adverse events were described as mild and less frequent in the ultrasound-guided acupotomy groups, ranging from 0% to 13.8%, compared with 0% to 51.7% in controls. Safety still depends heavily on operator skill, anatomy, sterile technique, and patient selection.
The geography limit matters for 3 reasons. First, acupotomy training and clinical expectations are more established in parts of China than in many Western pain clinics. Second, comparator care may differ from guideline-based physical therapy, exercise, medication, injection, or multidisciplinary pain programs used elsewhere. Third, publication and trial-registration norms can differ across research ecosystems.
Evidence-strength note: a 32-RCT meta-analysis sounds large, but the certainty rating is still the key constraint. GRADE started from randomized-trial evidence, then downgraded outcomes when blinding, heterogeneity, imprecision, or publication-bias concerns made the pooled estimate less secure. Moderate certainty for pain is meaningfully better than speculation; low certainty for several other endpoints means future trials could change the size or reliability of the effect.
That is the calibrated read: the pooled pain and function signals are directionally favorable, but the review is not strong enough to make ultrasound-guided acupotomy a universal chronic spinal pain default.
Safety Depends on Imaging, Anatomy, and Operator Skill
Ultrasound guidance is the main reason this version of acupotomy is different from blind needle-knife treatment. Real-time imaging can help the operator identify tissue depth, avoid vessels and nerves, and target the relevant soft-tissue plane. That is a plausible safety advantage, but it is not automatic.
Procedure risk: spinal pain procedures sit near nerves, vessels, fascia, muscle, and sometimes inflamed or degenerative tissue. A low adverse-event rate in trials does not remove the need for sterile technique, anatomy knowledge, image interpretation, informed consent, and a plan for post-procedure pain flare or bleeding risk.
Patient-selection risk: chronic spinal pain is not one disease. Lumbar disc herniation, cervical spondylosis, cervicogenic headache, ankylosing spondylitis, myofascial pain, and nonspecific chronic low-back pain can overlap clinically while responding differently to mechanical release, exercise, anti-inflammatory treatment, and behavioral pain care.
The review is therefore most useful for a narrow question: when an experienced operator uses ultrasound-guided acupotomy in a chronic spinal musculoskeletal pain population similar to the included trials, pain and disability usually move in the favorable direction.
The Result Should Be Compared With Real Chronic Pain Care
Chronic spinal pain usually needs layered care rather than a single procedural answer. Exercise, education, sleep repair, weight-bearing tolerance, psychological pain skills, anti-inflammatory strategies, medication review, and work modification can all affect outcomes. A procedure that improves pain can still disappoint if the patient remains deconditioned, fearful of movement, sleepless, or unable to return to ordinary activity.
Best-fit use case: ultrasound-guided acupotomy looks most plausible as an add-on option for selected chronic spinal musculoskeletal pain patients who have a mechanical soft-tissue target, access to a skilled operator, and a broader rehabilitation plan. That framing fits the subgroup result better than treating the procedure as a universal replacement for conservative care.
Worst-fit use case: nonspecific chronic pain with high central sensitization, severe sleep disruption, uncontrolled depression or anxiety, opioid instability, or unclear structural pain drivers may need broader pain-system management before a local tissue procedure is likely to carry the outcome.
The procedure also should not be interpreted as a test of “acupuncture” in general. Acupotomy is a needle-knife technique, and ultrasound guidance changes the procedural logic. The evidence here is about image-guided mechanical release in spinal musculoskeletal pain, not about ordinary acupuncture needles for all chronic pain syndromes.
What a Better Trial Would Need to Show
The next evidentiary step is a larger, cleaner trial rather than another small positive trial. A stronger trial would define the spinal diagnosis tightly, standardize the operator technique, use credible comparator care, blind outcome assessment when possible, and follow patients long enough to test recurrence and function rather than only short-term pain change.
A useful trial would also report adverse events in enough detail to separate expected post-procedure soreness from infection, bleeding, nerve irritation, vasovagal events, and symptom flares. Safety reporting matters because the clinical promise of ultrasound guidance is precision; the evidence has to show whether that precision changes real-world risk.
- Design need: multicenter trials outside a single research ecosystem.
- Comparator need: guideline-consistent physical therapy, exercise, medication, or sham/procedure controls when feasible.
- Outcome need: pain, disability, recurrence, adverse events, medication use, and return to activity.
Questions About Ultrasound-Guided Acupotomy for Spinal Pain
Is the pooled pain effect clinically meaningful?
Probably for selected patients, because SMD = −0.80 is not a trivial pooled effect. The certainty limit is trial quality and geography, not the direction of the pooled estimate.
Is add-on treatment the best-supported use?
Yes. The subgroup signal favored add-on ultrasound-guided acupotomy, which means the strongest evidence is for combining it with other care rather than treating it as a stand-alone replacement.
Did recurrence clearly decrease?
No. The recurrence point estimate favored treatment, but the 95% confidence interval crossed 1, so recurrence reduction was not statistically confirmed.
Who should interpret this cautiously?
Clinicians outside the Chinese treatment context should be cautious because training, technique, comparators, reimbursement, and patient expectations may differ substantially.
References
- Guan Y, Wang H, Zhang Z, Wang X, Zhao B. Efficacy and safety of ultrasound-guided acupotomy for chronic spinal musculoskeletal pain: a systematic review and meta-analysis of randomized controlled trials. Journal of Pain Research. 2026;19. https://doi.org/10.2147/jpr.s602089
- Furlan AD, Giraldo M, Baskwill A, Irvin E, Imamura M. Massage for low-back pain. Cochrane Database of Systematic Reviews. 2015. https://doi.org/10.1002/14651858.cd001929.pub3
- Treede RD, Rief W, Barke A, et al. Chronic pain as a symptom or a disease: the IASP Classification of Chronic Pain. Pain. 2019. https://doi.org/10.1097/j.pain.0000000000001384
- Qaseem A, Wilt TJ, McLean RM, Forciea MA. Noninvasive treatments for acute, subacute, and chronic low back pain. Annals of Internal Medicine. 2017. https://doi.org/10.7326/m16-2367