
A Kaiser Permanente Southern California cohort involving 294,937 children linked extreme prenatal nighttime heat to autism diagnosis by age 5, with stronger associations at the 99th percentile than the 90th percentile.1 Compared with nighttime minimum temperature, daytime maximum temperature did not show the same confirmed whole-pregnancy pattern.
Research Highlights
- Nighttime heat carried the main signal: among 294,937 children, whole-pregnancy 99th percentile minimum temperature was associated with autism diagnosis by age 5 (HR 1.382, 95% CI 1.062-1.797).1
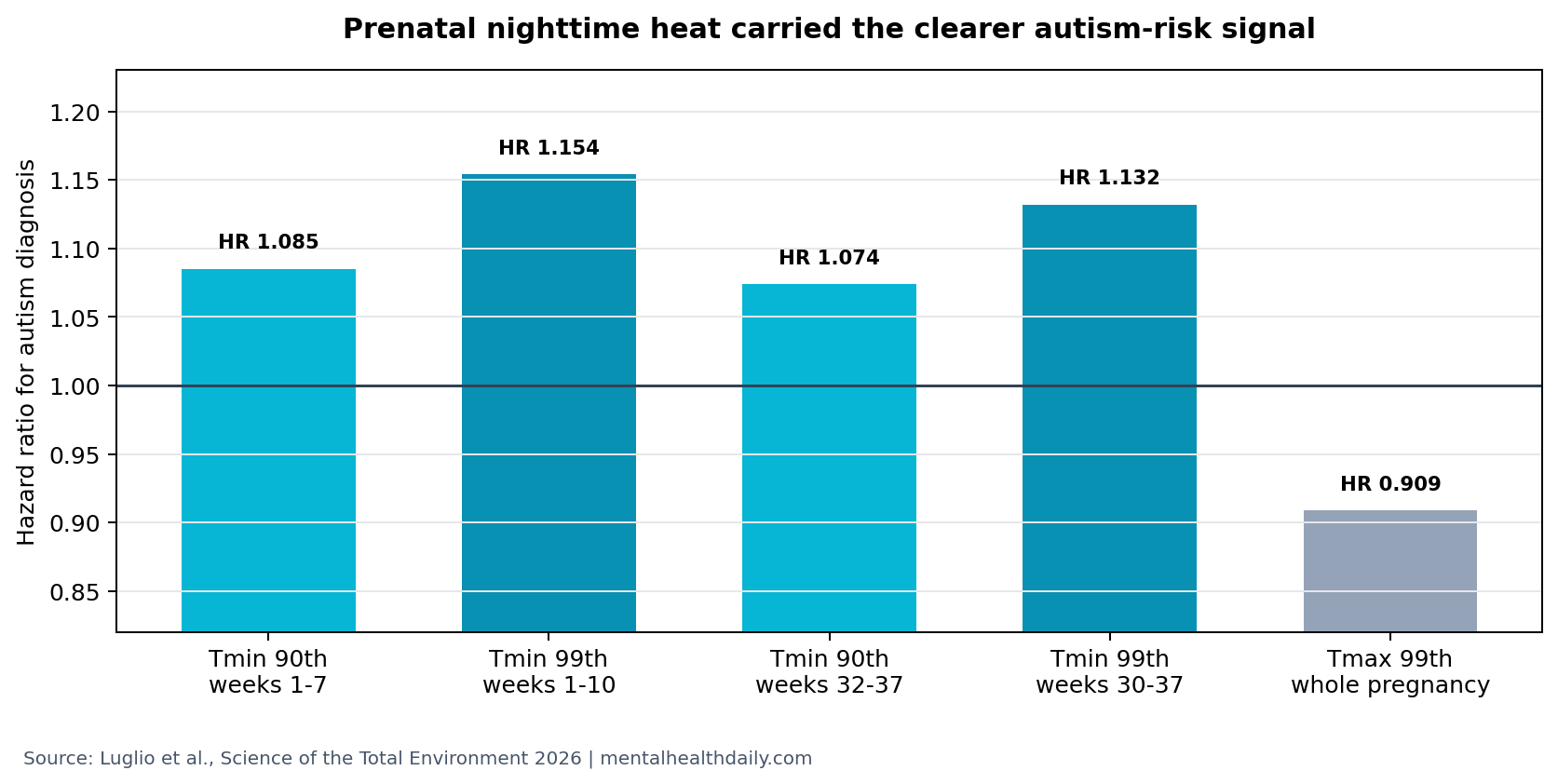
- Early pregnancy was one sensitive window: 99th percentile nighttime heat in weeks 1-10 had HR 1.154 (95% CI 1.040-1.288).1
- Late pregnancy also showed signal: 99th percentile nighttime heat in weeks 30-37 had HR 1.132 (95% CI 1.030-1.246).1
- Daytime maximum temperature was weaker than nighttime heat: whole-pregnancy 99th percentile maximum temperature had HR 0.909 (95% CI 0.662-1.247), not a confirmed positive association.1
- Causal proof is not available: the study modeled outdoor temperature exposure and recorded 4,076 autism diagnoses, but indoor heat, residual confounding, and diagnostic-pathway differences remain possible.1
Autism spectrum disorder is a neurodevelopmental condition involving differences in social communication, restricted or repetitive behaviors, sensory processing, and developmental trajectory. Environmental-risk studies do not explain autism as one cause. They ask whether exposures during brain-development windows shift diagnosis probability in a population.
Minimum temperature in this study was a nighttime heat proxy. That matters because hot nights can reduce recovery from daytime heat stress, disturb maternal sleep, and extend physiologic stress across a full 24-h cycle. Maximum temperature, the daytime proxy, was not the exposure with the clearest autism association.
294,937 Children Made This a Large Autism Heat Cohort
Luglio et al. analyzed Kaiser Permanente Southern California births and followed autism diagnosis by age 5. The cohort included 294,937 children and 4,076 autism diagnoses, with about 80% of autistic children male.1
The researchers used distributed lag nonlinear models. Distributed lag models estimate whether exposure during specific time windows, such as gestational weeks 1-7 or 30-37, is associated with later outcome risk. Hazard ratios compare diagnosis rates over time; HR 1.382 means the modeled rate was 38.2% higher than the reference exposure, not that any individual child had a certain outcome.
The strongest whole-pregnancy comparison was nighttime minimum temperature at the 99th percentile: HR 1.382, 95% CI 1.062-1.797. At the 90th percentile, whole-pregnancy minimum temperature was also elevated, HR 1.243, 95% CI 1.002-1.542. The confidence interval barely cleared 1.0 at the 90th percentile and was wider at the 99th percentile, so the result is meaningful but not mechanically precise.
Weeks 1-10 and 30-37 Were the Main Nighttime Heat Windows
The timing pattern was biologically plausible but not definitive. Early pregnancy includes implantation, placental development, early neural tube and brain-region patterning, and immune-endocrine shifts. Late pregnancy includes rapid fetal brain growth, sleep-wake development, and maternal physiologic strain.
Early window: at the 90th percentile, nighttime heat in weeks 1-7 had HR 1.085, 95% CI 1.011-1.165. At the 99th percentile, weeks 1-10 had HR 1.154, 95% CI 1.040-1.288.1
Late window: at the 90th percentile, nighttime heat in weeks 32-37 had HR 1.074, 95% CI 1.011-1.142. At the 99th percentile, weeks 30-37 had HR 1.132, 95% CI 1.030-1.246.1
The confidence intervals are modest, not dramatic. They support a population-level association, especially at extreme nighttime heat levels, but they do not justify a deterministic claim that heat exposure causes autism in a child.
Daytime Heat Did Not Show the Same Confirmed Pattern
Maximum temperature behaved differently from minimum temperature. Whole-pregnancy 90th percentile maximum temperature had HR 1.080, 95% CI 0.853-1.368, and 99th percentile maximum temperature had HR 0.909, 95% CI 0.662-1.247.1 Both intervals crossed 1.0.
That contrast limits overbroad climate-health headlines. The paper is not best read as “any heat during pregnancy raises autism risk.” The cleaner read is narrower: extreme nighttime heat showed the more consistent association, while daytime maximum temperature did not confirm a parallel signal in whole-pregnancy comparisons.
Prior prenatal environmental-risk studies have also found that exposure type and timing matter. California traffic-related air pollution and pregnancy PM2.5 studies reported associations with autism risk, but they did not imply that every environmental exposure operates through the same window or mechanism.2,3
Ozone Adjustment Complicates the Causal Story
Adjustment for ozone attenuated some nighttime-temperature associations. That can be interpreted in more than 1 way. Ozone may be a confounder if it tracks heat and independently contributes to risk. It may also sit partly on the pathway if extreme heat changes air chemistry and exposure patterns.
Outdoor exposure modeling: the study assigned temperature from residential geography rather than measuring the temperature inside each home. Air conditioning, building insulation, work setting, time outdoors, and nighttime cooling behavior could all change the heat dose a pregnant person actually experienced.
Diagnostic-pathway differences: autism diagnosis by age 5 depends on developmental surveillance, referral, insurance continuity, parental concern, clinician access, and local diagnostic practices. The Kaiser Permanente setting reduces some access variation, but it does not make diagnosis identical for every child.
Exposure mixture problem: heat does not travel alone. Hot periods can coincide with ozone, wildfire smoke, power-use patterns, sleep disruption, dehydration, medication changes, infection risk, and neighborhood-level differences in cooling access. A model can adjust for measured covariates, but it cannot prove that nighttime temperature itself is the sole active exposure.
Evidence-strength note: this was an observational exposure-modeling study. It can estimate associations in a large health system, but it cannot assign pregnant people to heat exposure, measure indoor temperature for each home, or fully separate heat from housing, neighborhood, air pollution, access to cooling, and diagnostic ascertainment.
Cooling Access Is the Practical Signal, Not Individual Blame
The calibrated public-health implication is practical: pregnancy heat protection should pay attention to nights as well as extreme daytime highs. A hot night can extend heat strain across sleep hours, reduce recovery, and leave fewer hours for the body to cool down before the next day.
Climate-health reviews already link heat and air pollution to adverse pregnancy outcomes, including preterm birth, low birth weight, and stillbirth.4 Autism risk is a more complex neurodevelopmental endpoint, but the pregnancy-protection logic overlaps: cooling access, indoor-temperature reduction, and heat-warning systems are easier to justify when they protect several maternal-child outcomes at once.
The result also argues against fear-based counseling. A hazard ratio of 1.382 at the 99th percentile describes a population association under extreme modeled conditions. A single hot week should not be treated as destiny for a child’s neurodevelopment or as a reason to turn pregnancy into an impossible temperature-control project.
For clinicians and public-health systems, the useful target is structural: identify pregnant people without reliable cooling, treat nighttime heat as a real exposure, and avoid reducing climate-related neurodevelopment research to a parent-blame message.
How to Read the Hazard Ratios Without Overstating Them
A hazard ratio is a relative-rate estimate, not an absolute-risk forecast. The study recorded 4,076 autism diagnoses among 294,937 children, so the outcome was uncommon even in a large cohort. A higher hazard ratio at extreme nighttime heat levels means the modeled diagnosis rate was higher than the reference exposure rate after adjustment, while most exposed children in the population still did not develop autism.
That denominator is the safeguard against both minimization and panic. A whole-pregnancy 99th percentile minimum-temperature HR of 1.382 is too large to ignore as a public-health signal, especially because the early- and late-pregnancy windows pointed in the same direction. The observational, exposure-modeled design makes the result better suited to population planning than individual prediction.
The strongest practical interpretation is risk reduction at the margins. If hot nights are one small contributor among many neurodevelopmental risk factors, improving nighttime cooling during pregnancy could still be worthwhile because it is low-regret maternal-health infrastructure. Extreme nighttime heat deserves a place in prenatal environmental-risk planning without being treated as a complete explanation for autism.
A useful next study would separate several exposure layers in the same pregnancy cohort:
- Indoor heat exposure: home temperature, air conditioning access, building insulation, and neighborhood heat-island conditions.
- Co-exposures: ozone, wildfire smoke, sleep disruption, dehydration risk, and maternal health conditions.
Until then, nighttime heat should be treated as a credible environmental signal with unresolved mechanism, not as a settled causal pathway.
Questions About Prenatal Heat and Autism Risk
Does this prove hot nights cause autism?
No. The study found population-level associations between modeled prenatal nighttime heat and autism diagnosis. It cannot prove causation for an individual child.
Why focus on nighttime temperature?
Nighttime heat may reduce recovery from daytime heat stress and disrupt maternal sleep. In this cohort, nighttime minimum temperature produced clearer autism-risk associations than daytime maximum temperature.
What is the practical public-health implication?
Cooling access during pregnancy, especially during hot nights, is a plausible prevention target for maternal and child health. The autism-specific evidence supports more careful study rather than panic or individual blame.
References
- Luglio DG, et al. Prenatal exposure to extreme heat and autism in children. Science of the Total Environment. 2026. doi:10.1016/j.scitotenv.2026.181373
- Becerra TA, Wilhelm M, Olsen J, Cockburn M, Ritz B. Ambient air pollution and autism in Los Angeles County, California. Environmental Health Perspectives. 2013. doi:10.1289/ehp.1205827
- Raz R, Roberts AL, Lyall K, et al. Autism spectrum disorder and particulate matter air pollution before, during, and after pregnancy. Environmental Health Perspectives. 2015. doi:10.1289/ehp.1408133
- Bekkar B, Pacheco S, Basu R, DeNicola N. Association of air pollution and heat exposure with preterm birth, low birth weight, and stillbirth in the US. JAMA Network Open. 2020. PubMed