A 2026 medRxiv preprint involving 65 early subacute stroke survivors found that a composite cerebral small-vessel disease MRI score predicted 90-day cognitive recovery more reliably than any single input marker.1 Lower baseline burden predicted higher follow-up Montreal Cognitive Assessment scores (β = −0.19; p = 0.009) and remained associated after baseline cognition was included (β = −0.12; p = 0.042).
Research Highlights
- 65 stroke survivors were analyzed: baseline MRI and cognition were measured within 21 days, with follow-up cognition at 90 days.
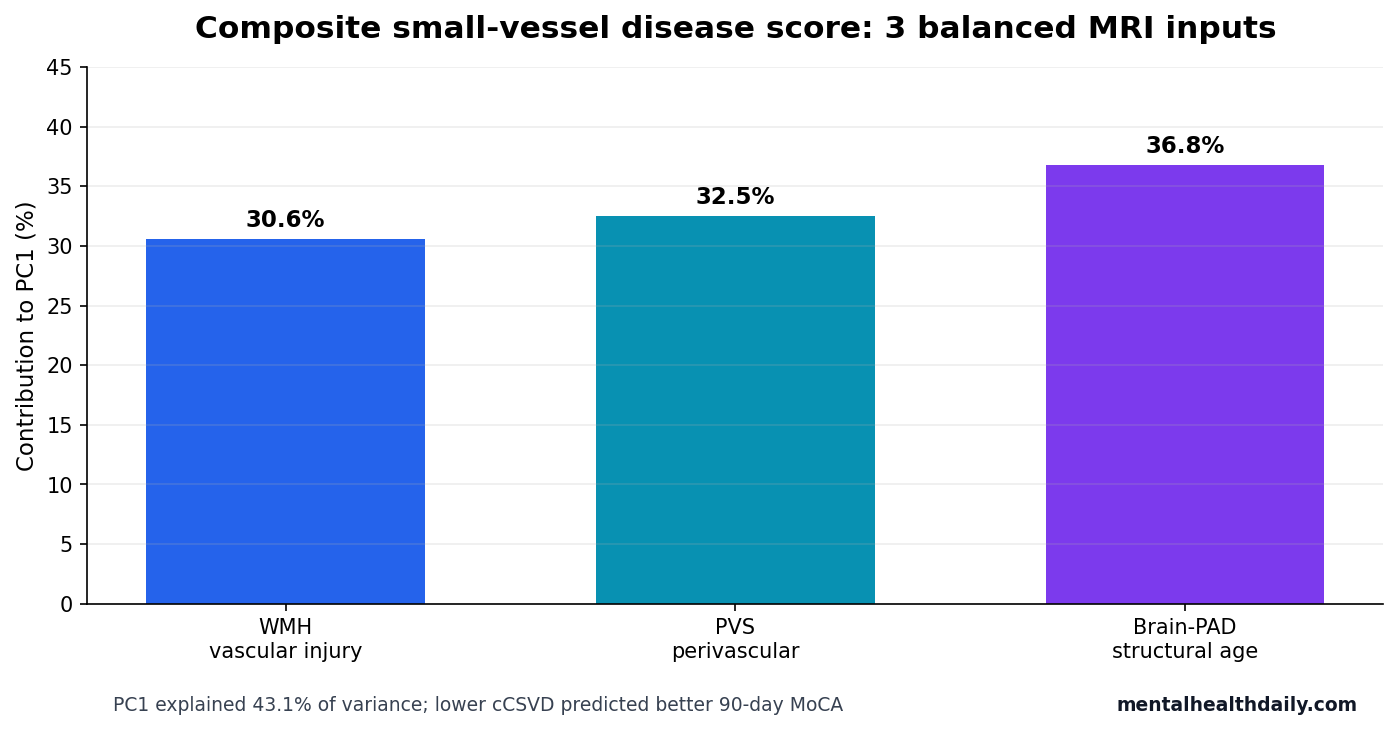
- 3 MRI markers formed 1 composite: PC1 explained 43.1% of variance across white matter hyperintensity volume, perivascular-space count, and brain-PAD.
- Inputs were balanced: WMH, PVS, and brain-PAD contributed 30.6%, 32.5%, and 36.8% to the composite score.
- Lower burden predicted higher 90-day MoCA: the follow-up association was β = −0.19 (p = 0.009), and β = −0.12 (p = 0.042) after baseline MoCA adjustment.
- Recovery-to-unimpaired status was more likely: lower cCSVD predicted improvement to MoCA ≥26 (OR = 0.34; p = 0.036).
Cerebral small-vessel disease means damage involving the brain’s small arteries, arterioles, capillaries, venules, and surrounding tissue. On MRI, it often appears as white matter damage, enlarged perivascular spaces, small infarcts, microbleeds, and tissue loss.
Brain-PAD means brain-predicted age difference: the gap between a person’s chronological age and the age predicted from structural MRI features. A higher value suggests an older-appearing brain structure than expected for age.
A 3-Marker T1 MRI Score Captured 43.1% of Shared Burden
Khan et al. used baseline T1-weighted MRI scans to quantify 3 automated markers: white matter hyperintensity volume, perivascular-space count, and brain-PAD. Each marker was residualized for age, sex, days since stroke, and intracranial volume before principal component analysis.
Principal component analysis is a method that compresses correlated variables into a smaller number of dimensions. Here, the first principal component became the composite small-vessel disease score, or cCSVD.
The composite was not dominated by one marker. White matter hyperintensity volume contributed 30.6%, perivascular-space count contributed 32.5%, and brain-PAD contributed 36.8%. That balance is the point: the score was intended to summarize a shared whole-brain burden rather than a single lesion type.
Lower cCSVD Predicted Better MoCA at 90 Days
MoCA is the Montreal Cognitive Assessment, a 30-point screening test covering domains such as attention, memory, language, executive function, and orientation. Scores below 26 are commonly used as a screening threshold for cognitive impairment, though the threshold is not a diagnosis by itself.
Lower baseline cCSVD predicted better follow-up MoCA scores at 90 days (β = −0.19; p = 0.009). The association persisted after baseline MoCA adjustment (β = −0.12; p = 0.042), which is the more relevant test because it asks whether early whole-brain structural burden still adds information after initial cognition is known.
- Baseline cognition: cCSVD did not become useful merely by rediscovering the first MoCA score.
- Follow-up cognition: lower composite burden tracked better 90-day cognitive status.
- Change status: lower burden predicted improvement to cognitively unimpaired status.
Individual Biomarkers Lost to the Composite Score
The central comparison was not MRI vs. no MRI. It was composite MRI burden vs. single MRI markers. In the authors’ stability-selection models, the cCSVD score outperformed white matter hyperintensity volume, perivascular-space count, brain-PAD, infarct volume, age, sex, education, comorbidities, and days since stroke for the cognitive outcomes tested.
White matter hyperintensities are bright MRI regions that often reflect chronic vascular injury, demyelination, edema, or gliosis. Perivascular spaces are fluid-filled spaces around blood vessels and may reflect vascular, drainage, or glymphatic integrity. Brain age summarizes broader cortical and subcortical structure.
Post-stroke cognition is distributed across networks, so a broad structural-burden score has a plausible advantage over a single lesion-type count. A person can have modest injury in several domains that together reduce recovery capacity even when no one marker looks extreme.
The Odds Ratio Needs Directional Care
For participants who had baseline cognitive impairment, lower cCSVD predicted improvement to cognitively unimpaired status at 3 months (OR = 0.34; p = 0.036). Because higher cCSVD means worse structural burden, an odds ratio below 1 for the score means higher burden was linked to lower odds of recovery.
Plain-language direction: less composite small-vessel burden at baseline meant better odds of crossing back above the MoCA impairment threshold by 90 days. The number should not be read as “0.34 times better”; it reflects the model direction for a burden score.
That directional clarity is important for readers. Stroke recovery models often mix positive recovery outcomes with negative burden predictors, and a reversed sign can make a real association look backward if the article does not name the direction.
Why the Composite May Beat Single MRI Markers
White matter hyperintensity volume, perivascular-space count, and brain-PAD each capture a different slice of chronic brain vulnerability. White matter hyperintensity volume leans toward visible vascular tissue injury. Perivascular-space burden may carry information about small-vessel, drainage, or glymphatic dysfunction. Brain-PAD summarizes whether global brain structure looks older than expected for chronological age.
A stroke survivor can have modest abnormality across all 3 domains without one marker looking dramatic. A composite score is designed for that pattern. It asks whether shared low-grade burden across vascular injury, perivascular structure, and whole-brain aging explains recovery better than any single measurement. In Khan et al., that shared-burden approach explained 43.1% of marker variance and outperformed the individual candidates in stability-selection models.
Reader-facing interpretation: the MRI score is not measuring the stroke lesion itself. It is measuring the condition of the brain that has to recover after the stroke. That distinction is why the finding is clinically plausible: 2 people with similar acute strokes may recover differently if one brain already carries more chronic small-vessel and structural-aging burden.
What External Validation Would Need to Prove
A useful clinical prediction score has to work outside the cohort that created it. For this cCSVD score, external validation would need to show that the same MRI pipeline predicts 90-day cognition in larger stroke samples, across scanner types, stroke subtypes, rehabilitation settings, and baseline cognitive ranges. It would also need calibration: predicted risk should match observed recovery rates and rank patients from lower to higher risk.
Comparator testing would be essential. The score should be tested against standard clinical predictors such as age, education, stroke severity, lesion location, lesion volume, baseline MoCA, vascular risk factors, depression symptoms, delirium, and rehabilitation intensity. A biomarker that adds little after those variables may still be biologically interesting, but it would be weaker as a triage tool.
Near-term use: the result is strongest as a research enrichment signal. Future trials could use cCSVD to stratify participants or test whether people with high structural burden need different rehabilitation intensity, longer follow-up, or added vascular-risk management. That is different from using the score to deny therapy or predict an individual patient’s ceiling.
Preprint Evidence Is Promising but Not a Clinical Triage Rule
Evidence-strength note: this is a medRxiv preprint. It has not been certified by peer review and should not guide clinical practice on its own. The sample was also small for predictive modeling, with 65 stroke survivors drawn from rehabilitation-focused cohorts.
The model is still useful as a research signal. Stroke prognosis often overweights focal lesion features even though cognition depends on distributed networks and preexisting brain health. A T1-based automated composite could eventually become scalable if external cohorts reproduce the association.
Prior imaging evidence supports the model’s ingredients without proving this exact composite. White matter hyperintensity burden has been linked to poorer stroke and dementia outcomes, perivascular-space measures have been studied as vascular or glymphatic markers, and brain-PAD has been used as a whole-brain aging marker in stroke recovery research.2
Workflow advantage: T1 MRI is widely acquired in stroke imaging, and the study deliberately used markers that can be derived from routine structural scans. That makes the approach more scalable than a model requiring specialized research sequences. Scalability is only one requirement, though. Automated segmentation must still be robust across scanner vendors, motion artifacts, lesion locations, and real-world clinical image quality.
Decision boundary: a high cCSVD score would be most useful if it changed what clinicians do next: earlier cognitive follow-up, targeted rehabilitation planning, vascular-risk optimization, family counseling, or trial stratification. A biomarker that predicts risk but does not change care can become an explanatory label rather than a useful tool. The next validation step should therefore test both prediction and actionability.
For now, high structural burden should prompt closer cognitive monitoring, practical recovery planning, and careful follow-up interpretation.
Questions About Small-Vessel Disease MRI Scores After Stroke
Does this mean a T1 MRI can predict stroke recovery for one patient?
No. The study developed and tested an association in a 65-person preprint cohort. Individual clinical prediction needs independent validation and calibration.
Why combine 3 markers instead of using white matter hyperintensities alone?
Cognition depends on distributed brain integrity. A composite can capture shared vascular injury, perivascular-space structure, and global brain aging in one burden score.
What would make the score more convincing?
Replication in larger, peer-reviewed, multi-site stroke cohorts with prespecified thresholds, external validation, and comparison against standard clinical predictors.
References
- Khan MH, Chakraborty S, Marin-Pardo O, et al. A composite measure of cerebral small vessel disease predicts cognitive change after stroke. medRxiv. 2026. doi:10.64898/2026.04.23.26351403
- PubMed search: white matter hyperintensity stroke cognitive recovery brain age perivascular spaces. https://pubmed.ncbi.nlm.nih.gov/?term=white+matter+hyperintensity+stroke+cognitive+recovery+brain+age+perivascular+spaces
- PubMed search: cerebral small vessel disease post stroke cognition MoCA. https://pubmed.ncbi.nlm.nih.gov/?term=cerebral+small+vessel+disease+post+stroke+cognition+MoCA
- PubMed search: brain predicted age difference stroke recovery cognition. https://pubmed.ncbi.nlm.nih.gov/?term=brain+predicted+age+difference+stroke+recovery+cognition