
A 2026 cross-sectional schizophrenia study found no meaningful association between antipsychotic dose and Montreal Cognitive Assessment (MoCA) performance in young, clinically stable outpatients. Cognitive scores related more strongly to symptom burden, illness duration, education, and age at diagnosis than to daily or 1-year cumulative antipsychotic exposure.1
Research Highlights
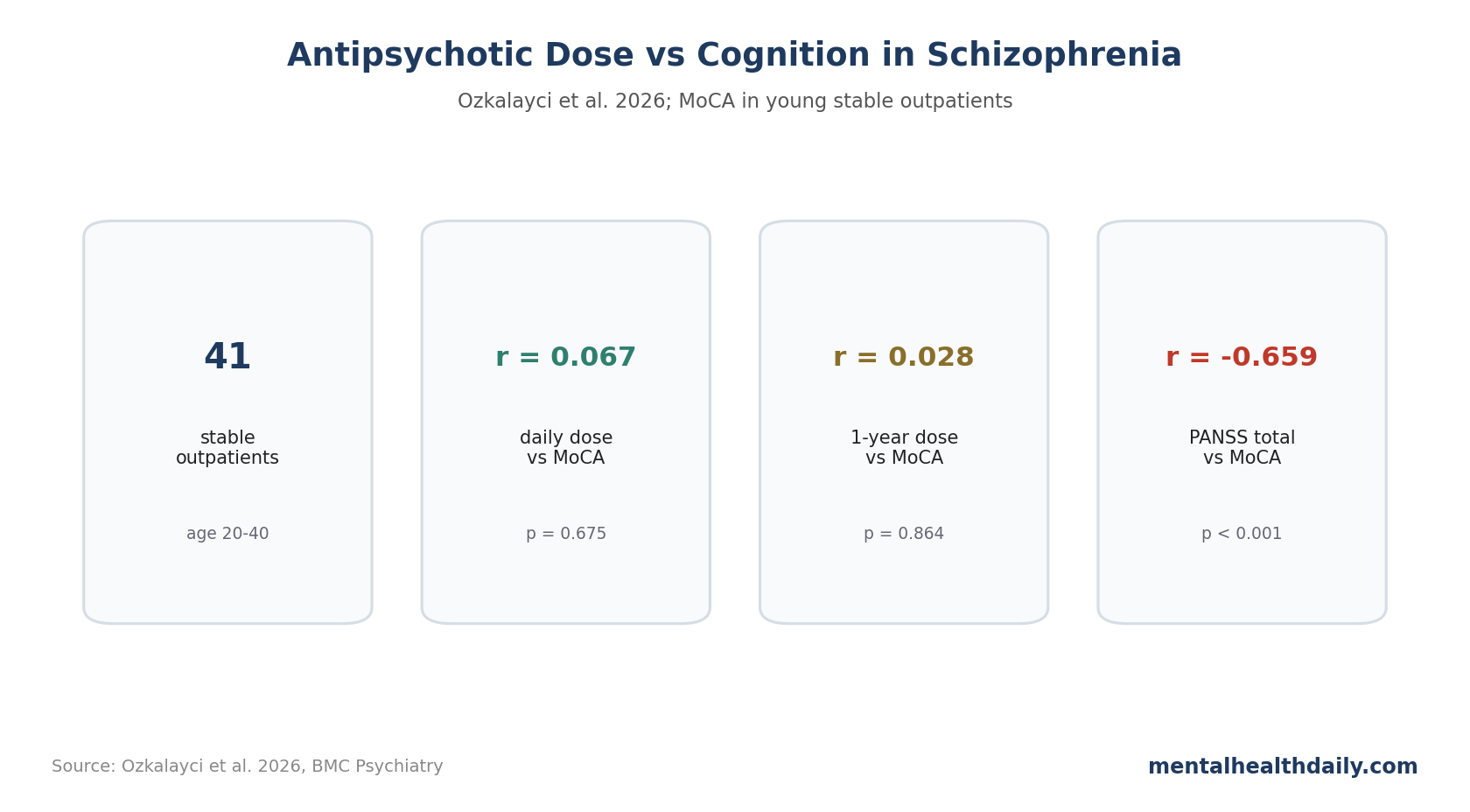
- Daily dose was not linked to MoCA: daily antipsychotic dose in olanzapine equivalents correlated weakly with Montreal Cognitive Assessment score, r = 0.067, p = 0.675.1
- 1-year exposure was also near zero: cumulative antipsychotic exposure had r = 0.028, p = 0.864, with Bayesian evidence not supporting a dose-cognition signal.1
- Symptoms tracked cognition more clearly: Positive and Negative Syndrome Scale (PANSS) total score correlated with MoCA at r = −0.659, p < 0.001.1
- 41 stable outpatients set the boundary: participants were 20-40 years old, clinically stable, and mostly receiving second-generation antipsychotics, so the result does not settle older, sedated, inpatient, or polypharmacy-heavy care.1
- Dose review still has 5 targets: relapse prevention, positive symptoms, sedation, anticholinergic co-prescribing, and daily function all belong in medication decisions even when MoCA is not dose-linked.
Antipsychotic cognition debates are difficult because schizophrenia itself is strongly associated with cognitive impairment. Medication dose, anticholinergic burden, sedation, illness severity, negative symptoms, education, and chronicity can all point in the same direction.
Ozkalayci et al. tried to reduce that noise by using a relatively homogeneous group, estimating both daily and cumulative antipsychotic dose, and testing symptom severity alongside medication exposure.
MoCA Was Tested Against Daily and 1-Year Dose Exposure
The researchers recruited 41 clinically stable outpatients with schizophrenia from a community mental health center. All were 20-40 years old. Most were taking second-generation antipsychotics (SGAs), and only 1 patient was receiving a first-generation antipsychotic (FGA) in combination with an SGA.1
- Cognition measure: Montreal Cognitive Assessment (MoCA), a brief screening tool for cognitive impairment.
- Symptom measure: Positive and Negative Syndrome Scale (PANSS), including positive, negative, general, and total scores.
- Dose conversion: antipsychotic doses were converted into olanzapine equivalents.
- Exposure windows: daily dose at interview and retrospectively estimated 1-year cumulative dose.
MoCA is not a full neuropsychological battery. It is useful for broad cognitive screening, but it can miss specific deficits in processing speed, verbal memory, working memory, and social cognition.
Antipsychotic Dose Correlations Were Near Zero
The headline finding is straightforward. MoCA score did not correlate significantly with daily antipsychotic dose: r = 0.067, p = 0.675. It also did not correlate with number of antipsychotics used, r = 0.166, p = 0.301, or with 1-year cumulative exposure, r = 0.028, p = 0.864.1
Biperiden dose, antidepressant dose, and daily anticholinergic burden were not significantly associated with MoCA either. The regression model likewise found no daily-dose effect after accounting for PANSS total score, illness duration, and age.
PANSS Total and Illness Duration Were the Stronger Cognitive Correlates
MoCA correlated negatively with PANSS positive, negative, general, and total scores. The strongest relationship was PANSS total: r = −0.659, p < 0.001. PANSS general was r = −0.564, PANSS negative was r = −0.524, and PANSS positive was r = −0.327 before correction.1
Education and age at diagnosis were positively correlated with MoCA, while illness duration was negatively correlated. In the regression model, PANSS total and illness duration significantly predicted cognitive performance; daily antipsychotic dose did not.
The pattern fits a broader schizophrenia literature in which cognitive impairment often predates treatment, appears around first episode, and relates to illness course and symptom dimensions.3
Sedation, Relapse Risk, and Side Effects Still Belong in Dose Decisions
The result should reduce one simplistic fear: in this young stable outpatient sample, higher antipsychotic dose was not the obvious driver of poorer MoCA performance.
It should not become an equally simplistic reassurance that dose never affects cognition. Higher doses can increase sedation, extrapyramidal symptoms, anticholinergic co-prescribing, metabolic burden, subjective dulling, and adherence problems in some patients.
The useful clinical target is optimization, not reflexive dose minimization: use enough antipsychotic medication to prevent relapse and reduce psychosis, while avoiding unnecessary polypharmacy, avoidable anticholinergic burden, and doses that add side effects without functional gain.
Clinical Decisions Should Track Function, Relapse, and Side Effects Together
The dose-cognition result is most useful when placed inside a broader medication decision. Antipsychotic dose cannot be optimized by MoCA alone, and it cannot be optimized by relapse prevention alone.
A practical medication review should separate 5 questions that can blur together during short visits:
- Relapse prevention: whether the current dose has kept psychosis stable across sleep disruption, stress, missed doses, or substance exposure.
- Positive symptoms: whether hallucinations, delusions, agitation, or disorganization are still driving cognitive failure.
- Sedation and akathisia: whether the medication is making attention, restlessness, sleep timing, or daytime energy worse.
- Anticholinergic load: whether biperiden, benztropine, sedating antidepressants, hypnotics, or other add-ons are contributing to memory and concentration complaints.
- Daily function: whether the dose supports work, school, social contact, self-care, and adherence rather than only improving a rating scale.
Cognition should also be measured with the right tool. MoCA is a short screen; it is not designed to dissect processing speed, working memory, verbal learning, attention/vigilance, and social cognition. If cognition is the treatment target, a fuller battery or functional cognitive assessment is better.
Polypharmacy deserves special attention. This sample had relatively little benzodiazepine or mood-stabilizer confounding, which helps interpretation. In routine care, cognitive complaints often arise in medication stacks that include anticholinergics, sedatives, hypnotics, antidepressants, and substances.
Individualized dose review is still the target. It weakens the blanket assumption that higher antipsychotic dose automatically explains poorer cognition in stable young outpatients, but it does not remove the need to minimize avoidable cognitive and functional side effects.
Bayesian Results Help Interpret Null Dose Findings
Ozkalayci et al. did more than report non-significant p-values. Bayesian analyses suggested evidence for the null hypothesis for daily antipsychotic dose and daily anticholinergic burden, while evidence for PANSS total was strong.
Bayesian evidence is useful here because a non-significant p-value alone can mean several things: no effect, small sample, noisy measurement, or underpowered design. The Bayesian analysis gives a more direct way to ask whether the data support no association in this sample.
Even so, sample size matters. With 41 patients, the study can rule out large simple correlations better than subtle nonlinear effects, medication-specific effects, or vulnerable subgroups.
The next step is not a bigger version of the same MoCA-only design. It is longitudinal measurement before and after dose changes, with medication-specific data, relapse control, side-effect ratings, and a cognitive battery that captures domains schizophrenia patients actually struggle with.
Symptom Reduction Can Indirectly Support Cognition
Psychosis itself can impair attention, memory encoding, motivation, sleep, and task persistence. If antipsychotic treatment reduces hallucinations, delusions, agitation, insomnia, or relapse risk, cognition may improve indirectly even when the medication has side effects.
That tradeoff is why dose decisions are rarely simple. Too little treatment can leave psychosis active and cognitively disruptive. Too much medication can add sedation or motor side effects. The clinical target is the lowest effective dose for stability and functioning, judged against symptoms, adverse effects, and daily function.
Cognitive Remediation Remains a Separate Treatment Question
If cognition is not primarily explained by dose in stable outpatients, then medication adjustment alone may not be enough. Cognitive remediation, supported employment, sleep treatment, aerobic exercise, social-cognitive training, and negative-symptom treatment may be more direct functional targets.
Medication review should therefore sit beside cognition-specific rehabilitation, not replace it. After psychosis is stabilized, the more useful question is whether the patient has access to evidence-based supports for attention, memory, social cognition, work functioning, sleep, and negative symptoms.
Medication-Specific Effects May Be Hidden in Total Dose
Olanzapine equivalents solve one problem and create another. They let researchers compare total antipsychotic dose across drugs, but they can hide medication-specific profiles: sedation, anticholinergic activity, prolactin effects, metabolic effects, and subjective cognitive dulling differ by agent.
A future study should test medication class, receptor profile, dose, serum level when available, and side-effect burden together. Cognition may depend less on total dopamine blockade alone and more on the whole medication package surrounding the patient.
Patient-reported cognition belongs in follow-up for the same reason. A normal MoCA with subjective cognitive dulling still deserves review of sedation, sleep, depression, anticholinergic load, and daily functioning.
Evidence strength is limited by the design. This was a small cross-sectional outpatient analysis, so it can weaken a simple dose-equals-cognitive-impairment claim in stable young patients, but it cannot show what happens after dose increases, medication switches, relapse prevention, or long-term exposure in higher-risk groups.
Questions About Antipsychotics and Cognition
Does this mean antipsychotics have no cognitive side effects?
No. It means dose was not associated with MoCA in this small stable outpatient sample. Cognition can still be affected by sedation, anticholinergic drugs, relapse, sleep, depression, substance use, and specific medication tolerability.
Why use olanzapine equivalents?
Different antipsychotics use different milligram scales. Olanzapine-equivalent conversion lets researchers compare total dose across medications, though no conversion system is perfect.
What should be measured next?
Larger longitudinal studies should use full cognitive batteries, symptom tracking, anticholinergic burden, sedation ratings, medication changes, relapse history, and functional outcomes.
References
- Antipsychotic dose is not associated with cognitive function in patients with schizophrenia. Ozkalayci et al. doi:10.1186/s12888-026-08086-x
- International consensus study of antipsychotic dosing using olanzapine equivalents. Gardner et al. doi:10.1176/appi.ajp.2009.09060802
- Schizophrenia cognition and antipsychotic dose studies. PubMed search. PubMed search
- PANSS, MoCA, and cognition in schizophrenia. PubMed search. PubMed search