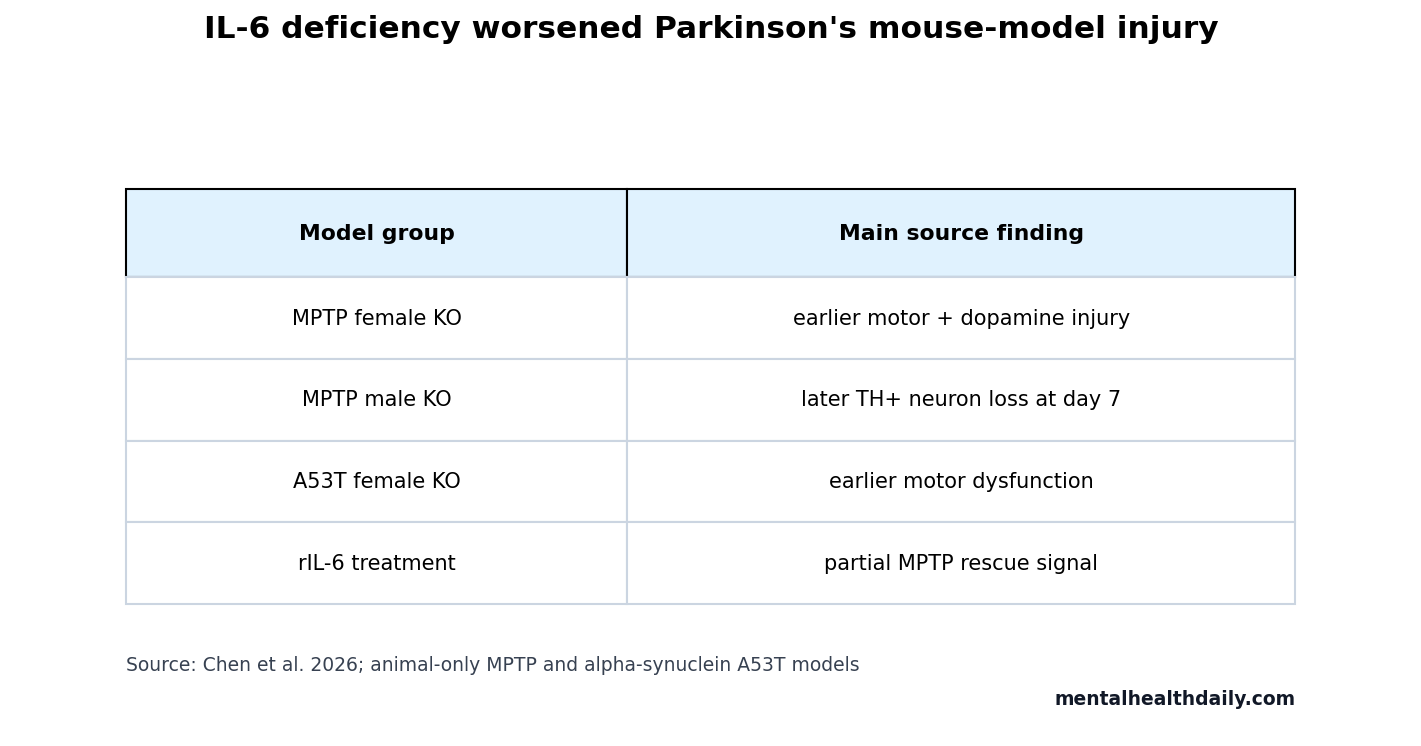
A 2026 mouse study found that complete IL-6 deficiency worsened motor dysfunction and dopaminergic injury in MPTP and alpha-synuclein A53T Parkinson’s disease models, with earlier and broader vulnerability in female knockout mice.1 The result cuts against a simple “less inflammation is always better” frame: recombinant IL-6 partly improved MPTP-induced motor dysfunction and striatal dopaminergic terminal depletion in both wild-type and knockout mice.
Research Highlights
- 2 Parkinson’s models were tested: Chen et al. used acute MPTP toxin exposure and alpha-synuclein A53T overexpression in mice.
- MPTP dosing was intensive: mice received 15 mg/kg MPTP 4 times at 2-hour intervals to produce nigrostriatal dopaminergic injury.
- Female knockout injury appeared earlier: female Il6 knockout mice showed more severe motor dysfunction and dopaminergic damage by 3 days after MPTP.
- Male knockout injury was delayed: male Il6 knockout mice showed more severe TH-positive neuron loss at 7 days, not at 1 or 3 days.
- Recombinant IL-6 partly rescued injury: 500 ng rIL-6 doses partly improved MPTP-induced motor dysfunction and striatal dopaminergic terminal depletion.
Interleukin-6 (IL-6) is a cytokine, a signaling protein used by immune and non-immune cells to coordinate inflammation, repair, and stress responses. In the brain, IL-6 can participate in damaging inflammation, but it can also activate survival and repair pathways depending on timing, receptor route, and cell type.
MPTP is a toxin used to model Parkinson’s-like dopaminergic injury in animals. It damages the nigrostriatal dopamine system, but it is not the same disease process as ordinary human Parkinson’s disease.
IL-6 Loss Worsened MPTP Motor Dysfunction in Both Sexes
Chen et al. compared Il6 knockout, Il6 heterozygous, and wild-type mice. Female mice were tested 3 days after MPTP administration. Male mice were tested at 1, 3, and 7 days after MPTP, giving the study a time-course view of sex-dependent injury.
The MPTP regimen was 15 mg/kg given 4 times at 2-hour intervals. Behavioral tests included the pole test, wire hanging test, open field test, rotarod test, and tape removal test. These assays are imperfect proxies, but together they cover movement speed, coordination, limb strength, exploratory activity, and sensorimotor response.
Female knockout pattern: MPTP-treated female Il6 knockout mice took longer to turn, climb down, and complete the pole test than their saline controls, and their wire hanging scores were lower than wild-type MPTP mice.
Male knockout pattern: male Il6 knockout mice also showed worse MPTP-related motor dysfunction, but the dopaminergic-neuron injury signal was clearest later, at 7 days after toxin exposure.
Female Knockout Mice Showed Earlier Dopaminergic Injury
Tyrosine hydroxylase (TH) is the rate-limiting enzyme for dopamine synthesis and is commonly used as a marker of dopaminergic neurons and nerve fibers. Lower TH signal after MPTP suggests worse dopaminergic injury.
Both female and male mice showed lower striatal TH protein after MPTP. The sex-dependent part was timing and severity. Female Il6 knockout mice had a more pronounced decrease in striatal TH protein than wild-type mice at 3 days, along with lower TH-positive fiber density in striatum and fewer TH-positive neurons in the substantia nigra pars compacta.
Male Il6 knockout mice lacked the same early knockout-vs.-wild-type separation at 1 or 3 days, but they did show greater TH-positive neuron loss at 7 days. The male knockout effect emerged later in the measured window.
Astrocyte Activation Was Stronger in Female Knockout Mice
Astrocytes are support cells that regulate metabolism, synapses, blood-brain barrier function, and inflammatory signaling. In injury states, they can become reactive, and GFAP is one common marker used to track that activation.
MPTP raised GFAP in both sexes, but female knockout mice showed a stronger glial-reaction pattern than female wild-type mice. GFAP protein in female knockout striatum trended higher than wild-type after MPTP (P = 0.067), and GFAP-positive cell counts in nigrostriatal regions were more elevated.
The male glial pattern was less knockout-selective. Male mice showed MPTP-related astrocyte activation, but differences between MPTP-treated male wild-type and knockout mice were not the main driver of the paper’s sex-dependent claim.
Alpha-Synuclein A53T Confirmed a Female-Vulnerability Pattern
Alpha-synuclein is the protein that accumulates in Lewy bodies, a pathological hallmark of Parkinson’s disease. The A53T mutation is a disease-linked variant often used in models to create toxic alpha-synuclein stress.
Chen et al. injected AAV alpha-synuclein A53T into the substantia nigra of 3-month-old female mice. The viral titer was 1.29 x 10^13 v.g/mL, and the injection volume was 200 nL. Behavioral testing began at 14 days after injection and continued weekly until day 35.
Female Il6 knockout mice developed earlier motor dysfunction and aggravated dopaminergic neurodegeneration in this alpha-synuclein model too. That second model matters because it reduces the chance that the entire result is an MPTP-only toxin artifact.
Recombinant IL-6 Rescue Keeps the Inflammation Story Calibrated
Recombinant IL-6 was administered intraperitoneally at 500 ng doses around MPTP exposure, and in the alpha-synuclein model from day 33 to day 35 after virus injection. In the MPTP model, rIL-6 partly ameliorated motor dysfunction and striatal dopaminergic terminal depletion in both wild-type and knockout mice.
Pathway caution: IL-6 signals through classical signaling, trans-signaling, and trans-presentation pathways, with downstream JAK-STAT, RAS-MAPK, PI3K-AKT, and NF-kappa B activity. Those routes can produce different effects, so a broad “IL-6 good” or “IL-6 bad” conclusion would be biologically sloppy.
Sex Differences Changed the Timing, Not the Direction, of the Signal
The sex-dependent result is easy to overread. Female Il6 knockout mice showed earlier and broader vulnerability, but the study did not show that IL-6 matters only in females. Male knockout mice also worsened after MPTP, especially by the later 7-day dopaminergic-neuron measure. The cleaner read is that IL-6 loss shifted vulnerability in both sexes, while female mice showed the injury pattern sooner in the measured window.
Timing: a single endpoint can make a pathway look sex-specific when the biology is partly time-dependent. Chen et al. avoided that trap by testing male mice at 1, 3, and 7 days after toxin exposure.
The male pattern looked weaker early and clearer later, which supports a delayed injury trajectory rather than a complete absence of male susceptibility.
Hormone and pathway caution: the paper discussed possible interaction with estradiol and inflammatory signaling, but the experiment did not isolate one hormone pathway as the cause. IL-6 can interact with glial activation, neuronal survival signaling, and sex-linked endocrine context. The study narrows the question; it does not solve the mechanism of female vulnerability in Parkinson’s disease.
Why the rIL-6 Result Does Not Make IL-6 a Treatment
Recombinant IL-6 partly rescued several MPTP outcomes, but that rescue was short-term, experimentally timed, and delivered in a controlled mouse injury model. Human Parkinson’s disease develops over years, involves heterogeneous genetic and environmental drivers, and already contains inflammatory signals that may be adaptive in one compartment and damaging in another.
Pharmacology: giving a cytokine systemically can affect immune cells, liver signaling, vascular tone, metabolism, and brain-adjacent inflammatory pathways. Blocking IL-6 can also have different effects depending on whether classical signaling or trans-signaling is the target.
The study is best read as pathway calibration: complete Il6 deficiency worsened dopaminergic vulnerability, while systemic IL-6 escalation remains a separate safety, targeting, and dose-control problem.
Clinical boundary: no patient should infer that IL-6 augmentation, cytokine injection, or avoidance of IL-6 blockade treats Parkinson’s disease from this paper. The result belongs in the preclinical risk map for neuroinflammation, sex differences, and dopaminergic survival.
For human translation, the useful question is more precise: which IL-6 signaling route, in which cell type, at which disease stage, protects dopaminergic neurons without amplifying harmful inflammation elsewhere?
Model triangulation: the paper’s use of both MPTP and alpha-synuclein A53T strengthened the inference. MPTP is an acute toxin model that stresses nigrostriatal dopamine neurons quickly. A53T alpha-synuclein overexpression is slower and closer to protein-aggregation biology, although still artificial. Seeing worse vulnerability in both settings makes complete Il6 deficiency look like a broader modifier of dopaminergic resilience rather than a quirk of one injury method.
What remains unresolved: the experiments did not identify whether neurons, astrocytes, microglia, peripheral immune cells, or endocrine pathways carried the decisive IL-6 signal. GFAP data point toward astrocyte involvement, and the recombinant IL-6 rescue points toward pathway responsiveness, but neither proves the critical cell type. Future work needs conditional knockouts or receptor-specific tools before the mechanism becomes clinically actionable.
Evidence-strength note: this was an animal-only mechanistic study. MPTP and alpha-synuclein A53T models are useful for dopaminergic injury and pathway testing, but they do not recreate the full human Parkinson’s disease process. Recombinant IL-6 is not a clinical Parkinson’s treatment based on this evidence.
Questions About IL-6 and Parkinson’s Mouse Models
Did this study show inflammation protects the brain?
No. It showed that complete IL-6 deficiency worsened model pathology and that rIL-6 partly rescued some MPTP effects. Other inflammatory pathways can still be harmful.
Were female mice more vulnerable?
Yes, in these models. Female Il6 knockout mice showed earlier and broader motor, dopaminergic, and glial injury than male knockout mice.
Does this support IL-6 therapy for Parkinson’s disease?
No. The finding is preclinical and cytokine manipulation can be risky. Human treatment claims need separate pharmacology, safety, and clinical trial evidence.
References
- Chen F, Duan Y, Wang M, et al. Sex-dependent impact of Il6 deficiency in Parkinson’s disease mice. Genes & Diseases. 2026;13:101986. https://doi.org/10.1016/j.gendis.2025.101986
- PubMed search: IL-6 Parkinson disease MPTP dopaminergic neurons. https://pubmed.ncbi.nlm.nih.gov/?term=IL-6+Parkinson+disease+MPTP+dopaminergic+neurons
- PubMed search: Parkinson disease sex differences neuroinflammation IL-6. https://pubmed.ncbi.nlm.nih.gov/?term=Parkinson+disease+sex+differences+neuroinflammation+IL-6
- PubMed search: alpha-synuclein A53T mouse model IL-6 dopaminergic neurodegeneration. https://pubmed.ncbi.nlm.nih.gov/?term=alpha-synuclein+A53T+mouse+model+IL-6+dopaminergic+neurodegeneration