A 2026 review concluded that GLP-1 receptor agonists have plausible stroke biology and modest prevention signals, but current human evidence does not support routine use as acute ischemic stroke neuroprotection.1 The useful clinical split is prevention in cardiometabolic patients vs. acute brain-rescue treatment after stroke onset.
Research Highlights
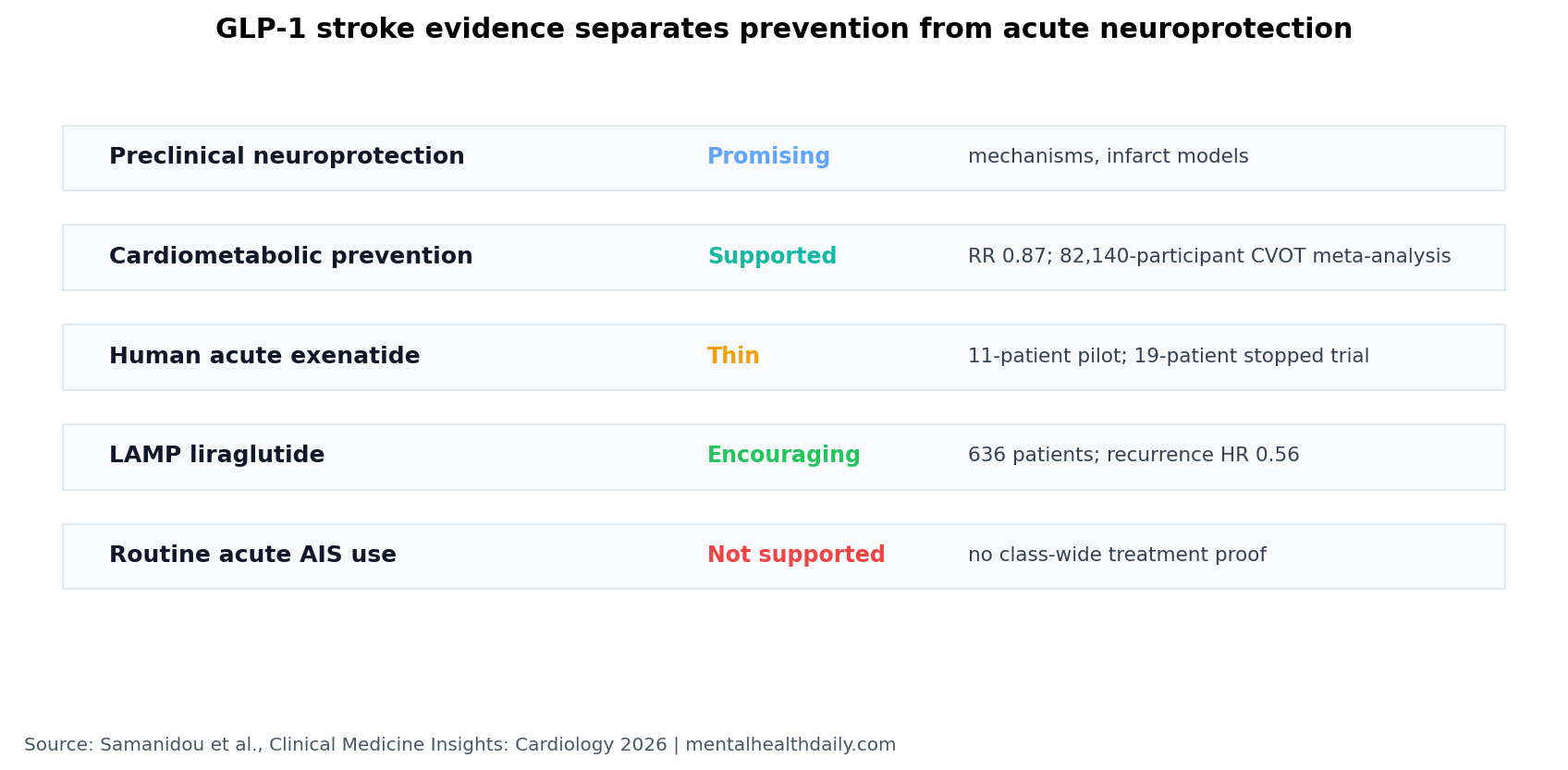
- Acute neuroprotection is not established: the 2026 review found no current basis for routine GLP-1 receptor agonist use as acute ischemic stroke treatment.1
- Prevention evidence is stronger than acute-treatment evidence: a 2018 meta-analysis reported total-stroke RR 0.87 (95% CI 0.78-0.98, P 0.021) in cardiometabolic populations.1
- Large CVOTs point in the same direction: an 11-trial cardiovascular-outcome meta-analysis with 82,140 participants reported a 16% relative stroke reduction.1
- Individual trials vary: REWIND dulaglutide reported stroke HR 0.76, while SUSTAIN-6 semaglutide reported nonfatal stroke HR 0.61.2,3
- Human acute-stroke trials remain thin: exenatide studies involved 11 and 19 patients, while LAMP enrolled 636 patients and reported encouraging liraglutide outcomes.1
GLP-1 receptor agonists are drugs that mimic or amplify glucagon-like peptide-1 signaling, a gut-hormone pathway involved in insulin secretion, appetite, weight, inflammation, and vascular biology. Semaglutide, liraglutide, dulaglutide, and exenatide are the familiar examples.
Acute ischemic stroke happens when a blocked blood vessel deprives part of the brain of oxygen and glucose. A neuroprotective drug would need to preserve threatened brain tissue during or shortly after that injury; long-term vascular-risk reduction months earlier is a different clinical target.
Stroke Prevention Signals Are Stronger Than Acute Neuroprotection Signals
Samanidou et al. reviewed evidence from cell and animal models, observational studies, randomized trials, cardiovascular outcome trials, and meta-analyses through January 2026.1 The pattern is uneven but interpretable: GLP-1 drugs have better human evidence for reducing stroke incidence in cardiometabolic populations than for rescuing brain tissue after acute stroke.
Prevention signal: the review cited a 2018 meta-analysis reporting a 13% total-stroke reduction, RR 0.87, 95% CI 0.78-0.98, P 0.021. It also cited an 11-CVOT meta-analysis with 82,140 participants and a 16% relative stroke reduction.1
REWIND reported lower stroke risk with dulaglutide, HR 0.76, 95% CI 0.61-0.95, P 0.01.2 SUSTAIN-6 reported lower nonfatal stroke with semaglutide, HR 0.61, 95% CI 0.38-0.99, P 0.04.3 Those trials were not acute stroke-rescue trials; they were cardiovascular-outcome trials in patients with diabetes or cardiometabolic risk.
That distinction changes how the data should be used. A cardiovascular-outcome trial asks whether years of metabolic and vascular treatment reduce future events.
An acute neuroprotection trial asks whether a drug given around a blocked artery preserves threatened brain tissue after injury has already started. The second question needs time-to-treatment windows, infarct imaging, reperfusion status, edema and bleeding monitoring, and functional recovery endpoints.
Several trial rows point in the same direction without proving a uniform class effect:1
- LEADER liraglutide: total stroke HR 0.86, with a confidence interval crossing 1.0.
- EXSCEL exenatide: total stroke HR 0.85, with a confidence interval crossing 1.0.
- SELECT semaglutide: nonfatal stroke HR 0.93 in adults with overweight or obesity but without diabetes.
In plain terms: the prevention signal is real enough to study and clinically relevant when GLP-1 drugs are otherwise indicated, but it does not show that every agent strongly prevents stroke in every high-risk population.
Preclinical Brain-Protection Biology Has Not Translated Cleanly
Animal and cell studies give GLP-1 drugs a plausible stroke-neuroprotection rationale. Reported pathways include reduced excitotoxicity, apoptosis, oxidative stress, neuroinflammation, blood-brain barrier disruption, and support for angiogenesis or neurogenesis.1
Excitotoxicity means excessive glutamate-driven neuronal activation that can injure cells after ischemia. Blood-brain barrier disruption means the vascular wall separating blood from brain tissue becomes leaky, allowing inflammatory and fluid shifts that can worsen injury.
The translation problem is timing, dose, patient selection, and outcome measurement. A mouse model can receive a controlled drug dose around an induced stroke. A human patient arrives with unknown onset time, mixed comorbidity, reperfusion treatment decisions, edema risk, infection risk, glucose variation, and rehabilitation variables.
Mechanistic plausibility is still useful because it identifies what future trials should measure. The review’s proposed pathways fall into a few practical buckets:
- Cell-survival signaling: less excitotoxicity, apoptosis, and oxidative stress after ischemic injury.1
- Inflammation control: lower neuroinflammatory signaling in experimental models, which could matter because post-stroke inflammation can expand injury beyond the initially blocked-vessel territory.1
- Vascular-barrier effects: less blood-brain barrier disruption, a pathway that could affect edema, hemorrhagic transformation risk, or downstream immune-cell entry.1
- Repair biology: signals of angiogenesis and neurogenesis, meaning new blood-vessel growth and neural repair processes, though those are harder to separate from general recovery in human trials.1
A clean stroke trial needs the 90-day modified Rankin Scale and intermediate imaging or biomarker endpoints that tell whether GLP-1 treatment changed infarct growth, perfusion, blood-brain barrier injury, inflammation, or recovery biology. Without those intermediate checks, a positive functional result could still be metabolic, vascular, rehabilitation-related, or selection-driven rather than direct neuroprotection.
Exenatide Trials Were Too Small to Settle Acute Stroke Treatment
Human acute ischemic stroke evidence remains thin. The review describes an exenatide pilot with 11 patients and a prehospital exenatide trial stopped at 19 patients.1 Those sample sizes can establish feasibility signals, dosing tolerability, and protocol problems. They cannot establish a routine acute-stroke indication.
TEXAIS tested exenatide within 9 h of stroke onset and did not improve 7-day neurological impairment. That negative or non-confirming result is important because it is closer to the acute neuroprotection claim than the cardiovascular-outcome trials are.
Evidence-strength note: the review is not a new pooled analysis, and the underlying acute-stroke studies are heterogeneous. The class may still contain a useful agent, dose, or subgroup, but current evidence does not support routine acute use outside trials.
LAMP Makes Liraglutide Interesting, Not Settled
The LAMP liraglutide trial enrolled 636 patients and reported lower recurrence, HR 0.56, 95% CI 0.34-0.91, P 0.02, plus better 90-day outcomes, OR 1.95, 95% CI 1.28-3.00, P 0.002.1 That is the human stroke-treatment signal that deserves attention.
It still does not convert the entire class into proven acute neuroprotection. Liraglutide, semaglutide, dulaglutide, and exenatide differ in pharmacokinetics, dosing, trial populations, and outcomes. A recurrence or functional-outcome signal also needs separation from glucose, weight, vascular, and rehabilitation effects.
Agent-level differences matter: a weekly semaglutide prevention trial, a daily liraglutide post-stroke protocol, and a small exenatide acute-treatment study are not interchangeable tests of the same clinical action. Drugs in the same class can differ in half-life, central nervous system penetration, nausea or dehydration risk, glucose effects, and practical fit with thrombolysis, thrombectomy, swallow status, and early inpatient care.
The review’s most useful conclusion is therefore calibrated rather than dismissive. GLP-1 receptor agonists are not ready to be added to routine acute ischemic stroke protocols as brain-rescue drugs. They are also not irrelevant to stroke: patients with diabetes, obesity, chronic kidney disease, or established cardiovascular disease may already have reasons to use them, and the long-term event-reduction literature makes stroke prevention part of that risk-benefit discussion.
This framing avoids overreading the class. If a patient already meets a metabolic or cardiovascular indication, stroke-risk reduction can be part of the expected benefit profile. If the only reason for treatment is acute ischemic stroke neuroprotection, the evidence base is still investigational and should be tested with stroke-specific protocols rather than borrowed from diabetes and obesity trials.
Future Trials Need Timing, Reperfusion, and Safety Answers
Stroke-dedicated trials need to answer 3 questions before the acute-treatment claim becomes credible.
- When should treatment start? A neuroprotective effect that requires very early exposure may fail in ordinary practice if most patients arrive outside the useful biological window.
- How does treatment interact with reperfusion? Thrombolysis and thrombectomy already change infarct evolution. GLP-1 trials need to show whether benefit appears before, during, or after vessel reopening, and whether bleeding or edema risks change.
- Which patients are plausible responders? Diabetes status, obesity, baseline glucose, stroke subtype, infarct size, kidney function, nausea risk, and route of administration could all decide whether the drug is useful or impractical.
Those are not academic details. If a trial enrolls a broad stroke population and misses the subgroup most likely to respond, a real signal could disappear. If it enrolls only highly selected patients, the result may not generalize to emergency stroke pathways. The prevention evidence justifies better trials; it does not remove the need for them.
Questions About GLP-1 Drugs and Stroke
Should GLP-1 drugs be started during an acute stroke?
Routine acute ischemic stroke use is not supported by current evidence. Any acute neuroprotection role should remain inside clinical trials or highly specific research protocols.
Are GLP-1 drugs useful for stroke prevention?
They may reduce stroke risk in patients who already have cardiometabolic indications such as type 2 diabetes or obesity-related vascular risk. That prevention signal is stronger than the acute-treatment evidence.
What is the most defensible clinical position?
Use GLP-1 receptor agonists for established metabolic and cardiovascular indications. Do not market them as acute stroke neuroprotectants until larger stroke-specific trials confirm timing, dose, safety, and outcomes.
References
- Samanidou E, et al. GLP-1 Receptor Agonists in Acute Ischemic Stroke: Current Evidence and Future Directions. Clinical Medicine Insights: Cardiology. 2026. doi:10.1177/11795735261444425
- Gerstein HC, Colhoun HM, Dagenais GR, et al. Dulaglutide and cardiovascular outcomes in type 2 diabetes. Lancet. 2019. doi:10.1016/s0140-6736(19)31149-3
- Marso SP, Bain SC, Consoli A, et al. Semaglutide and cardiovascular outcomes in patients with type 2 diabetes. New England Journal of Medicine. 2016. doi:10.1056/nejmoa1607141
- Liraglutide after acute ischemic stroke trial investigators. Liraglutide and post-stroke outcomes. New England Journal of Medicine. 2025. doi:10.1056/nejmoa2501006