A 2026 randomized study involving 80 people with schizophrenia found that adding high-frequency repetitive transcranial magnetic stimulation to risperidone improved PANSS cognitive-factor scores and aggressive-behavior ratings more than risperidone alone over 4 weeks.1
Research Highlights
- Design was randomized but short: 80 patients were assigned to risperidone alone or risperidone plus rTMS, 40 per group, with no dropouts during 4 weeks.1
- Cognitive-factor score improved more: After treatment, the combination group scored 11.39 ± 2.44 vs. 12.84 ± 2.13 in the risperidone-only group (p = 0.006).1
- Aggression score improved more: MOAS scores were 14.12 ± 2.75 with combination therapy vs. 15.77 ± 2.62 with risperidone alone (p = 0.007).1
- 5 biomarkers moved in the expected direction: TNF-alpha and IL-18 were lower, while IL-10, BDNF, and VEGF-A were higher in the combination group after treatment.1
- Blinding was weak: The study was single-center, lasted 4 weeks, and acknowledged that participants and assessors knew treatment allocation, which limits confidence in subjective ratings.1
Repetitive transcranial magnetic stimulation is a noninvasive neuromodulation method that uses magnetic pulses to change cortical excitability. In this study, stimulation targeted the left dorsolateral prefrontal cortex, a frontal control-network region involved in working memory, impulse control, and top-down regulation of behavior.
20 Hz Left-DLPFC rTMS Was Added to 4-6 mg/day Risperidone
All participants received risperidone, started at 1 mg/day and titrated to a 4–6 mg/day maintenance range. The combination group also received 20 Hz rTMS over the left dorsolateral prefrontal cortex at 100% motor threshold.
- Session structure: 20 trains, each lasting 4 seconds, separated by 56-second intervals.
- Schedule: 1 daily session, 5 days per week, for 4 weeks.
- Target logic: Left-DLPFC stimulation is meant to strengthen executive control networks that are often impaired in schizophrenia.
The study measured cognition using PANSS negative-symptom items N5, N6, and N7: impaired abstract thinking, lack of spontaneity and flow of conversation, and stereotyped thinking. That is narrower than a full neuropsychological battery. It measures cognitive-expression features inside a symptom scale, not memory, processing speed, or attention across standardized cognitive tests.
Cognitive-Factor and Aggression Scores Separated After 4 Weeks
At baseline, cognitive scores were nearly identical: 15.62 ± 2.47 in the risperidone-only group and 15.71 ± 2.65 in the combination group. After 4 weeks, scores were lower in both groups, but lower still with rTMS: 12.84 ± 2.13 vs. 11.39 ± 2.44.1
The Modified Overt Aggression Scale showed a similar pattern. Baseline scores were 23.76 ± 3.45 and 23.72 ± 3.59. After treatment, the risperidone-only group averaged 15.77 ± 2.62, while the rTMS group averaged 14.12 ± 2.75.1
Clinical interpretation: the between-group gaps were statistically significant, but modest in raw points. The finding is best read as an add-on signal, not proof that rTMS transforms cognition or violence risk in schizophrenia.
- Cognition endpoint: PANSS-derived interview items, not a full cognitive battery.
- Aggression endpoint: MOAS scale scores, not incident-level safety events.
- Duration endpoint: 4 weeks, with no maintenance or relapse information.
Inflammatory and Neurotrophic Markers Shifted With Combination Treatment
BDNF is brain-derived neurotrophic factor, a protein involved in synaptic plasticity and neuronal adaptation. TNF-alpha and IL-18 are inflammatory cytokines; IL-10 is an anti-inflammatory cytokine.
After 4 weeks, the combination group had lower TNF-alpha (11.25 ± 1.81 vs. 12.76 ± 1.64 pg/mL) and IL-18 (4.20 ± 1.07 vs. 5.39 ± 1.12 pg/mL). It also had higher IL-10 (11.66 ± 2.95 vs. 10.33 ± 2.62 pg/mL), BDNF (14.39 ± 2.52 vs. 13.14 ± 2.44 pg/mL), and VEGF-A (235.36 ± 23.88 vs. 220.72 ± 23.25 pg/mL).1
Those shifts fit a plausible neuromodulation story: stimulation may alter cortical network activity, which may secondarily influence inflammatory and plasticity pathways. They do not establish mediation. The study did not show that cytokine changes caused symptom improvement.
Adjunctive rTMS Evidence in Schizophrenia Remains Mixed
Earlier evidence-based rTMS guidelines gave schizophrenia negative-symptom protocols only limited support, and large sham-controlled trials have not produced uniformly positive results.2,4 Cognitive findings are also target- and domain-specific. A 2019 meta-analysis found small cognitive benefits for high-frequency prefrontal rTMS, but heterogeneity remained a major limitation.3
- Signal: Zhou et al. adds a randomized 80-patient add-on result with symptom-scale cognition, aggression, and biomarker movement.
- Weakness: no blinding, 4-week endpoint, single center, and no full cognitive battery.
- Next test: a blinded sham-controlled trial with MCCB cognition, aggression events, functional outcomes, and 3- to 6-month follow-up.
What the Cognitive Score Did and Did Not Measure
The study’s cognitive endpoint came from PANSS negative-symptom items, not a dedicated cognitive battery. That choice has consequences. PANSS N5, N6, and N7 capture clinician-rated abstract thinking, conversation spontaneity, and stereotyped thinking. They are relevant to schizophrenia function, but they do not directly measure processing speed, working memory, verbal learning, visual memory, attention, or social cognition.
Clinical implication: the result supports improvement in cognitive-expression symptoms during clinical interview. It does not prove broad cognitive remediation. A future trial should include the MATRICS Consensus Cognitive Battery or another standardized neuropsychological package, plus functional outcomes such as work readiness, social functioning, and independent living skills.
- PANSS cognitive-factor strength: easy to collect during symptom assessment.
- PANSS cognitive-factor weakness: vulnerable to interviewer expectation, sedation, negative symptoms, and general clinical improvement.
- Neuropsychological strength: better domain separation.
- Functional-outcome strength: closer to what patients and families actually notice.
Blinding Is the Central Method Problem
rTMS produces scalp sensation, sound, appointment intensity, therapist contact, and a sense that something active is happening. Those features can influence subjective outcomes even when the magnetic stimulation has no specific neural effect. Zhou et al. acknowledged that participants and assessors knew treatment allocation.1
- Subjective-rating risk: aggression ratings and PANSS interview items can shift with expectation.
- Biomarker risk: inflammation and plasticity markers can move with sleep, activity, adherence, diet, and infection.
- Cleaner test: sham-controlled stimulation, blinded raters, registered primary outcomes, and adverse-event tracking.
The signal still deserves follow-up because cognition, aggression, inflammation, and neurotrophic markers all moved in a coherent direction. The next trial should make that coherence harder to explain by expectation or ordinary clinical contact.
A stronger design would also separate the stimulation-specific question from the extra-care question. Add-on rTMS means more appointments, more staff contact, more symptom monitoring, and a visible procedure.
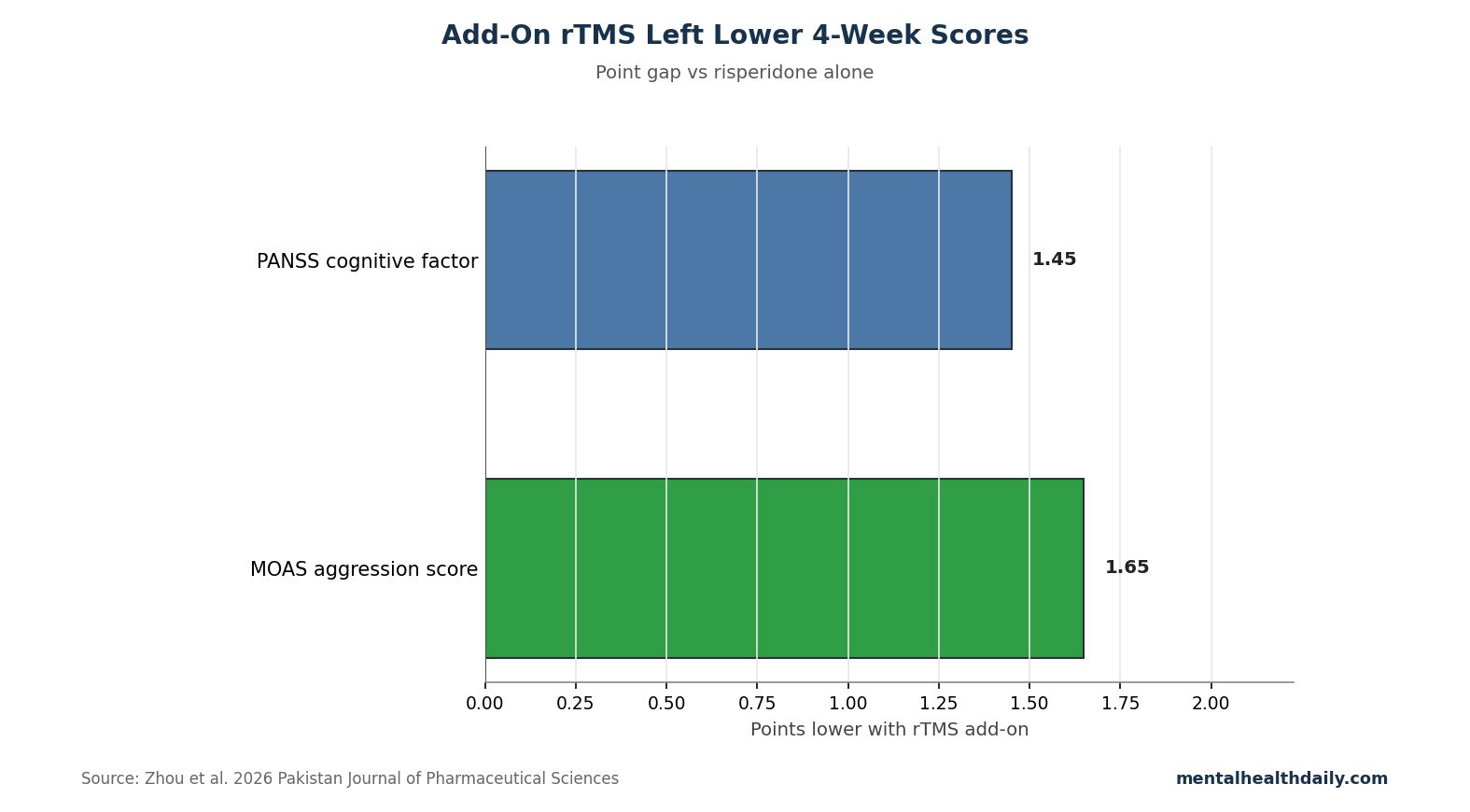
Those elements can improve adherence or clinician attention even if the magnetic protocol itself contributes little. A credible sham condition and blinded outcome ratings are the only way to tell whether the 1.45-point PANSS cognitive-factor gap and the 1.65-point MOAS aggression gap came from cortical stimulation rather than the treatment package around it.
Where the Result Could Fit Clinical Research
The most reasonable research niche is early adjunctive treatment for patients whose positive symptoms improve on antipsychotics while cognitive disorganization, poor impulse control, or aggression risk remain active. That is different from using rTMS as a broad schizophrenia treatment. The study tested add-on stimulation during risperidone treatment, not stimulation as monotherapy.
Trial design target: future work should separate symptom domains at baseline, pre-register cognition and aggression endpoints, use credible sham stimulation, and measure whether any score change translates into fewer aggression incidents, shorter hospitalization, better family safety, or improved occupational functioning.
Safety Reporting Needs More Detail
The article did not present a detailed adverse-event table. For rTMS trials in schizophrenia, safety reporting should include headache, scalp pain, dizziness, sleep disruption, seizure, symptom worsening, agitation, medication changes, and discontinuation reasons. Because aggression was an outcome, trials should also specify whether aggression incidents were staff-rated events, family reports, ward incidents, or scale-only changes.
Interpretive guardrail: a lower MOAS score is encouraging, but incident-level reporting would tell readers whether daily safety actually changed.
Replication priority: the next study should also report medication dose, smoking status, sleep, baseline inflammation, and anticholinergic burden, because each can influence cognition and inflammatory markers in schizophrenia.
That reporting detail matters for clinical translation. A patient with fewer ward incidents, fewer emergency restraints, or better family safety is different from a patient whose aggression scale moved modestly while daily risk stayed the same. The 2026 trial is best read as a signal-generating adjunctive-treatment result, not proof that rTMS should be added routinely to risperidone for cognition or aggression.
The key question is durability: whether 4-week score differences remain after stimulation stops or require maintenance sessions.
Questions About rTMS Plus Risperidone
Is this enough to recommend rTMS for schizophrenia cognition?
No. The study supports further trials. It does not establish routine clinical use because it lacked blinding and used a narrow PANSS-derived cognition score.
Did rTMS replace risperidone?
No. rTMS was an add-on. Every participant received risperidone.
Why target the left DLPFC?
The left dorsolateral prefrontal cortex supports executive control, working memory, and inhibition. Those systems are relevant to cognitive symptoms and aggression risk in schizophrenia.
References
- Effects of repetitive transcranial magnetic stimulation combined with risperidone on improving cognitive function and aggressive behavior in patients with schizophrenia and its effects on serum indicators. Zhou S, Tu H, Lin J. Pakistan Journal of Pharmaceutical Sciences. 2026;39(5):1452–1459. doi:10.36721/PJPS.2026.39.5.15520.1
- Evidence-based guidelines on therapeutic use of repetitive transcranial magnetic stimulation. Lefaucheur JP, Aleman A, Baeken C, et al. Clinical Neurophysiology. 2020;131(2):474–528. doi:10.1016/j.clinph.2019.11.002
- Effects of high-frequency transcranial magnetic stimulation for cognitive deficit in schizophrenia: a meta-analysis. Jiang Y, Guo Z, Xing G, et al. Frontiers in Psychiatry. 2019;10:135. doi:10.3389/fpsyt.2019.00135
- Left prefrontal high-frequency rTMS for schizophrenia with predominant negative symptoms. Wobrock T, Guse B, Cordes J, et al. Biological Psychiatry. 2015;77(11):979–988. doi:10.1016/j.biopsych.2014.10.009