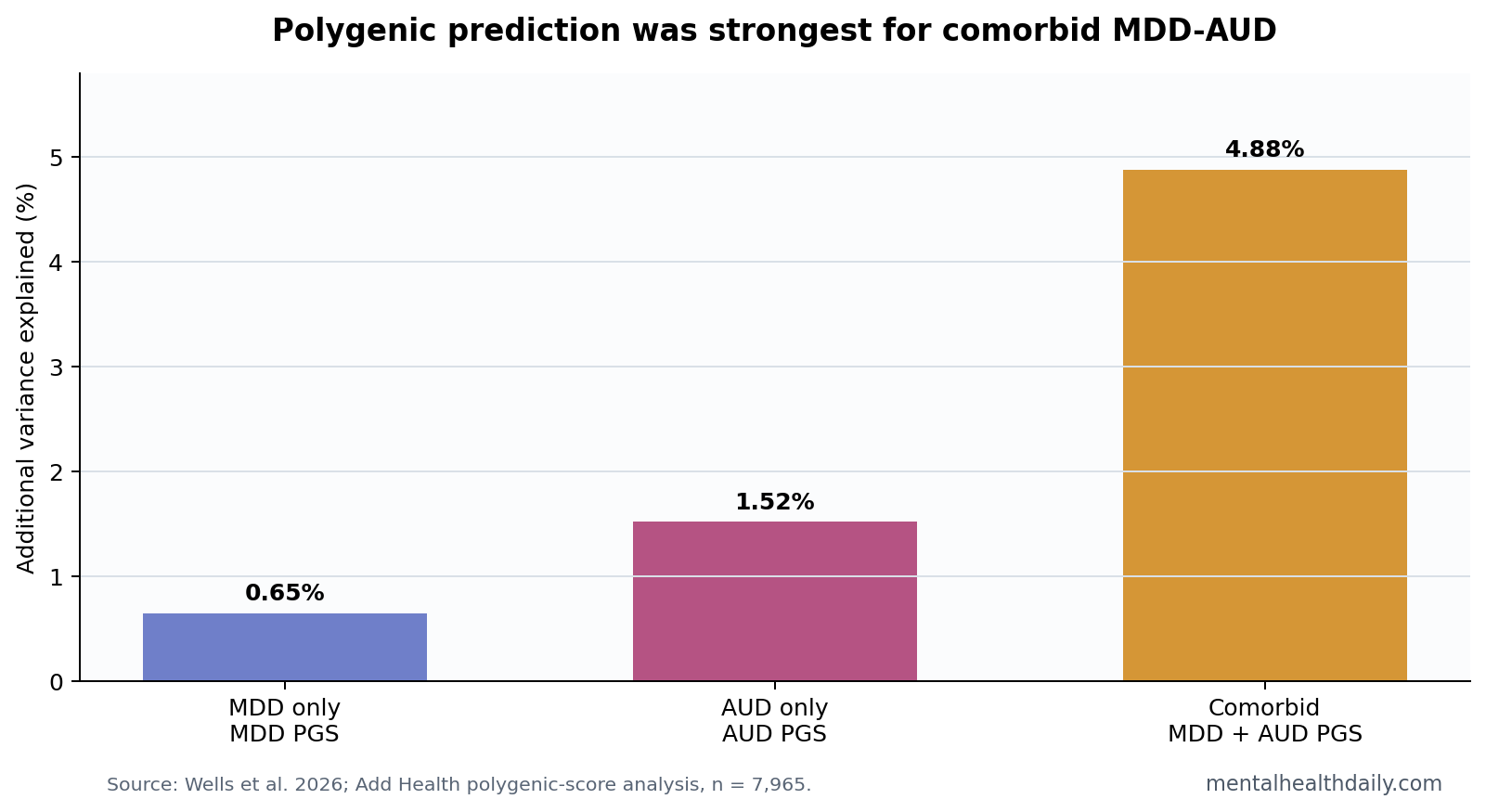
A 2026 Add Health analysis found that combining major-depression and alcohol-use-disorder polygenic scores added 4.88% variance for comorbid MDD-AUD prediction, while same-trait scores added only 0.65% for MDD and 1.52% for AUD alone.1 The genetic signal is strongest where the clinical problem is hardest: depression plus alcohol-use disorder, not either diagnosis in isolation.
Research Highlights
- Comorbidity signal: In 7,965 Add Health participants, the combined MDD and AUD polygenic-score model added 4.88% variance for comorbid MDD-AUD.1
- Single-disorder ceiling: The best MDD-only model added 0.65% variance, while the best AUD-only model added 1.52% variance.1
- Two scores mattered together: In the comorbid model, the MDD PGS had OR 1.26 and the AUD PGS had OR 1.77, both independently associated with MDD-AUD.1
- Prediction stayed modest: The comorbid model added 4.88% variance beyond covariates, so this is not a clinical diagnostic test.
- Comorbidity looked genetically heavier: The pattern fits a higher shared-liability subtype more than a new genetic architecture unique to MDD-AUD.1
Polygenic scores add up many small genetic associations across the genome into a single risk index. They are not “depression genes” or “alcoholism genes”; they are statistical summaries built from genome-wide association studies, where thousands or millions of variants each contribute tiny amounts of predictive information.
Major depressive disorder (MDD) and alcohol use disorder (AUD) often travel together clinically. The comorbid form carries more than 2 labels on a chart: people with both conditions often have more severe symptoms, harder treatment courses, and higher relapse or resistance risk than people with either condition alone.2
Combined MDD-AUD Scores Added More Signal Than Either Disorder Alone
Wells et al. tested whether polygenic scores for MDD and AUD improved prediction of MDD-only, AUD-only, and comorbid MDD-AUD in the National Longitudinal Study of Adolescent to Adult Health. The analytic sample included 7,965 participants across European, African, and Admixed American ancestry groups.1
The headline result was not that genetic scores are now clinically powerful. The result was more specific: a 2-score model was more informative for the comorbid phenotype than for either single diagnosis.
Comorbid MDD-AUD: the best whole-sample model included both MDD and AUD polygenic scores. The MDD score was associated with comorbidity at OR 1.26, 95% CI 1.16 to 1.35, p = 2.69 x 10^-6. The AUD score was stronger, OR 1.77, 95% CI 1.66 to 1.87, p = 3.49 x 10^-28. Together, the scores added 4.88% variance beyond sociodemographic covariates.1
MDD alone: the best MDD model included the MDD polygenic score, OR 1.25, 95% CI 1.17 to 1.33, p = 2.05 x 10^-8, and added 0.65% variance.1
AUD alone: the best AUD model included the AUD polygenic score, OR 1.37, 95% CI 1.32 to 1.43, p = 1.25 x 10^-28, and added 1.52% variance.1
What 4.88% Added Variance Means Clinically
Variance explained is the portion of outcome differences captured by a model. A 4.88% increment is meaningful for psychiatric genetics, where most common-variant scores remain modest. It is not large enough to support direct individual diagnosis.
Model scope: the result detects stronger genetic loading in people with both MDD and AUD while keeping most liability outside these 2 scores.
Environment, development, trauma exposure, alcohol access, psychiatric history, social context, measurement error, rare variants, and many unmeasured pathways still carry most of the prediction burden.
The most practical interpretation is risk stratification for research, not screening in ordinary care. A research cohort enriched for high MDD-AUD polygenic liability might help test mechanisms or prevention hypotheses. A clinic should not tell a patient that a score predicts depression plus AUD with enough accuracy to guide diagnosis.
Reader calibration: the odds ratios are per-score increases, not absolute-risk promises. OR 1.77 for the AUD score in the comorbid model means higher AUD genetic liability was associated with higher odds of MDD-AUD in this dataset; absolute individual risk still depends on baseline risk, environment, symptoms, drinking trajectory, and clinical history.
Risk communication has to keep those layers separate.
Otherwise, association turns into genetic fatalism.
Comorbidity Looked Like Higher Load, Not a Separate Genetic Disorder
The researchers also tested whether the MDD and AUD scores interacted. A strong interaction would suggest that carrying both forms of liability creates something qualitatively different from adding the 2 risks together. The interaction was not statistically significant.1
That points toward a simpler model: comorbid MDD-AUD may represent heavier combined liability for depression and alcohol problems rather than a genetically separate condition. The clinical syndrome can still behave differently, but the common-variant architecture did not need a special interaction term to explain the pattern.
- Supported: people with comorbid MDD-AUD carried stronger combined polygenic signal than people defined by either single diagnosis.
- Not supported: the 2026 analysis did not establish a deterministic MDD-AUD genotype.
- Still unresolved: how much polygenic liability improves prediction when paired with family history, early alcohol exposure, trauma, symptoms, and treatment response.
Prior Genetics Explains Why the AUD Score Was So Informative
AUD genetics has become more useful because discovery samples have grown. Walters et al. reported genome-wide work on alcohol dependence that helped establish common-variant liability for alcohol-related disorder risk.3 Zhou et al. later expanded cross-ancestry discovery for problematic alcohol use, strengthening the base from which AUD polygenic scores are derived.4
Those discovery studies matter because a polygenic score cannot be stronger than the data used to build it. Larger and more diverse discovery sets usually improve signal, but psychiatric and substance-use phenotypes remain noisy. Diagnostic definitions vary, self-report can misclassify drinking problems, and ancestry imbalance can make scores travel poorly across populations.
Wells et al. used PRS-CSx, a cross-ancestry method designed to borrow information across ancestry-specific genome-wide association results. That is an improvement over older Eurocentric scoring, but it is not a full solution. Genetic prediction still tends to perform differently across ancestry groups because discovery data, linkage disequilibrium patterns, environmental exposure, and diagnosis practices differ.
Ancestry caveat: cross-ancestry modeling reduces one old failure mode, but it cannot erase the social and statistical unevenness of psychiatric genetics. If a future model performs well in one ancestry group and weakly in another, a pooled average would hide the exact problem clinicians and researchers need to see.
Comorbid MDD-AUD Is the Right Target for Better Prediction
Briere et al. showed why MDD-AUD comorbidity deserves its own lane: lifetime depression and alcohol problems often co-occur, and the combination can carry worse symptom course than either condition alone.2 The 2026 genetic result adds a biological clue to that clinical literature: the comorbid group may be more genetically loaded for both traits.
Evidence-strength note: this was an observational genetic prediction analysis. It can estimate association and incremental prediction. It cannot show that the measured variants cause one person’s depression, alcohol-use disorder, or comorbidity, and it cannot decide treatment.
For clinicians and researchers, the result supports a more precise question: when depression and alcohol-use disorder cluster in the same person, are prevention and treatment studies underpowered because they treat comorbidity as a nuisance variable instead of a risk-enriched subgroup?
That question is more useful than asking whether polygenic scores should enter routine psychiatric intake. The current numbers are too modest for that. They are better suited to study design: define the comorbid subgroup clearly, measure drinking trajectory and depressive course together, and test whether combined liability predicts relapse, chronicity, or response to integrated treatment.
How to Use the Finding Without Genetic Determinism
Polygenic scores can be abused when they are described as destiny. The numbers here do not justify that. Even the strongest comorbid model added less than 5% variance, leaving most prediction unexplained.
The constructive use is narrower:
- Research enrichment: identify groups with higher combined genetic liability for mechanistic studies.
- Subgroup analysis: test whether high MDD-AUD liability predicts treatment resistance, relapse, or course severity.
- Model integration: combine genetics with family history, symptoms, stress exposure, and alcohol-use trajectory.
- Equity check: report score performance by ancestry rather than assuming one pooled result works everywhere.
The calibrated read is direct: MDD and AUD polygenic scores are more informative together when the outcome is comorbidity. That makes the comorbid phenotype biologically interesting, but it does not make polygenic screening ready for psychiatric practice.
Questions About MDD-AUD Polygenic Scores
Does a high polygenic score mean someone will develop MDD-AUD?
No. A polygenic score shifts probability; it does not determine an individual’s outcome. The 2026 model added 4.88% variance for comorbid MDD-AUD, which is useful for research but far from deterministic.
Why did the combined model work better for comorbidity?
Comorbid MDD-AUD appears to concentrate liability for both depression and alcohol problems. The MDD and AUD scores each added independent signal when the outcome was the combined condition.
Can this guide treatment?
Not yet. The analysis did not test medication, psychotherapy, relapse prevention, or sequencing of care. It supports better subgroup research, not a treatment algorithm.
References
- Wells M, et al. The Contributions of Multiple Polygenic Scores in Predicting Liability for Major Depressive Disorder and Its Comorbidity with Alcohol Use Disorder. Behavior Genetics. 2026. https://doi.org/10.1007/s10519-026-10263-3
- Briere FN, Rohde P, Seeley JR, Klein D, Lewinsohn PM. Comorbidity between major depression and alcohol use disorder from adolescence to adulthood. Journal of Affective Disorders. 2014. https://doi.org/10.1016/j.jad.2013.11.019
- Walters RK, et al. Transancestral GWAS of alcohol dependence reveals common genetic underpinnings with psychiatric disorders. Nature Neuroscience. 2018. https://doi.org/10.1038/s41593-018-0275-1
- Zhou H, et al. Multi-ancestry study of the genetics of problematic alcohol use. Nature Genetics. 2023. PubMed search