A 99-patient randomized trial found that adding esketamine to sufentanil patient-controlled analgesia lowered postoperative depression and anxiety scores at 24 and 72 hours after colorectal cancer surgery, while resting and activity pain scores did not differ by group.1 That pattern makes the result more interesting than simple pain relief: the mood signal was partly independent of analgesia.
Research Highlights
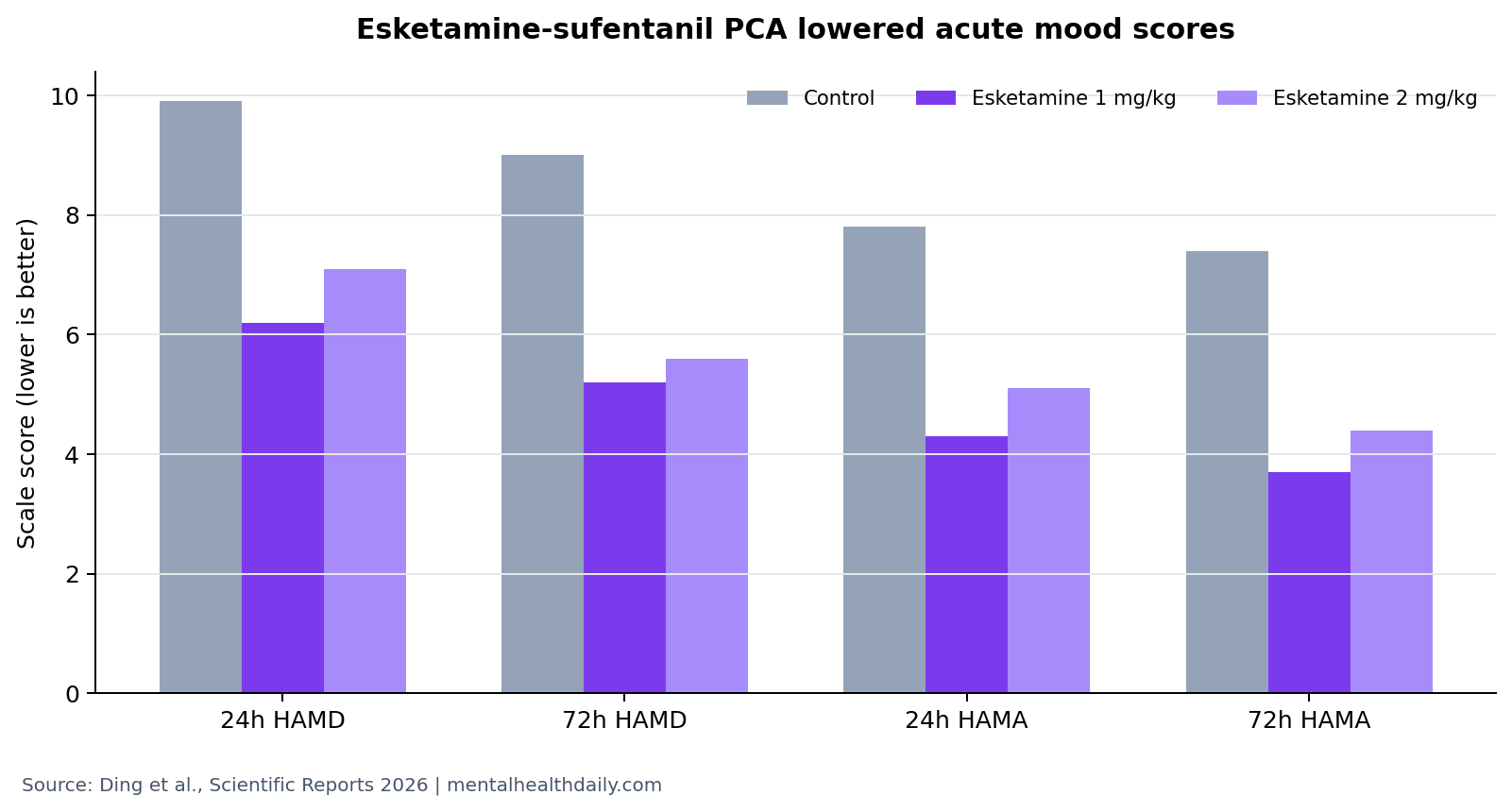
- Depression scores fell by 24 hours: HAMD-17 scores were 9.9 in control vs. 6.2 with esketamine 1 mg/kg and 7.1 with esketamine 2 mg/kg (p < 0.001 overall).1
- Anxiety scores moved similarly: HAMA scores at 24 hours were 7.8 in control vs. 4.3 and 5.1 in the 2 esketamine groups.1
- Pain did not explain the effect: resting VAS had no group effect (F = 0.872, p = 0.422), and activity VAS had no group effect (F = 0.681, p = 0.509).1
- Safety looked comparable: 24-hour adverse events were 26.7%, 22.6%, and 16.7% in control, ES1, and ES2 groups, respectively.1
- Follow-up was short: the trial measured acute mood state through 72 hours, not long-term prevention of major depression after surgery.1
Esketamine is the S-enantiomer of ketamine, a glutamatergic anesthetic and antidepressant-related drug that can affect NMDA receptor signaling, synaptic plasticity, and rapid mood pathways. Sufentanil is a potent opioid analgesic used for postoperative pain control.
Patient-controlled analgesia (PCA) lets patients self-administer controlled doses of pain medication within preset safety limits. In this trial, the key question was whether adding esketamine to sufentanil PCA improved postoperative mood beyond ordinary analgesic recovery.
HAMD Scores Were Lower at 24 and 72 Hours With Esketamine
Ding et al. randomized elderly colorectal cancer resection patients to 3 PCA regimens: sufentanil-only control, sufentanil plus esketamine 1 mg/kg, or sufentanil plus esketamine 2 mg/kg. The planned enrollment was 99 patients, with 33 per group; 8 were lost after randomization, leaving fewer analyzed participants.1
HAMD-17 is the 17-item Hamilton Depression Rating Scale, a clinician-rated measure of depressive symptom severity. Preoperative HAMD scores were not significantly different across groups. At 24 hours, scores were 9.9 in control, 6.2 in ES1, and 7.1 in ES2. At 72 hours, scores were 9.0 in control, 5.2 in ES1, and 5.6 in ES2.1
The 1 mg/kg and 2 mg/kg esketamine groups were both lower than control at the postoperative timepoints. The trial did not show a clean dose-response advantage for 2 mg/kg; if anything, the low-dose group looked at least as good for several mood scores.
Anxiety Scores Followed the Same Acute Pattern
HAMA is the Hamilton Anxiety Rating Scale. Baseline HAMA scores were similar across groups: 5.7 in control, 5.8 in ES1, and 6.2 in ES2. At 24 hours, the scores were 7.8, 4.3, and 5.1. At 72 hours, they were 7.4, 3.7, and 4.4.1
That anxiety pattern matters because postoperative distress includes more than pain. Cancer surgery, anesthesia, sleep disruption, inflammation, uncertainty, opioid exposure, and delirium risk can all shape mood state in the first days after surgery.
Clinical interpretation: the trial supports an acute mood-state effect in a specific postoperative setting. It does not prove that esketamine prevents major depressive disorder or long-term anxiety after cancer surgery.
Pain Scores Did Not Improve More With Esketamine
Resting visual analog scale pain scores showed a strong time effect as patients recovered, but no group effect (F = 0.872, p = 0.422) and no group-by-time interaction (F = 0.941, p = 0.454). Activity pain scores were similar: time changed, but group and interaction effects did not.1
PCA bolus demands also did not differ significantly: 4.69 in control, 4.16 in ES1, and 5.77 in ES2 (F = 0.884, p = 0.417). Correlations between 24-hour pain scores and HAMD scores were not significant for resting VAS (Kendall tau-b = −0.080, p = 0.336) or activity VAS (tau-b = −0.024, p = 0.767).1
Why this matters clinically: if mood improvement were only better pain relief, analgesic differences would be the obvious explanation. Here, pain measures failed to separate groups, so glutamatergic mood biology, stress-response modulation, sleep, or expectancy-related recovery experience becomes more plausible.
Safety and Satisfaction Favored Feasibility, Not Certainty
Adverse events were comparable. At 24 hours, adverse events occurred in 8 control patients (26.7%), 7 ES1 patients (22.6%), and 5 ES2 patients (16.7%); the group comparison was not significant (p = 0.643). At 48 hours, rates were 20.0%, 3.2%, and 10.0%, with p = 0.109.1
Satisfaction differed more clearly. “Very satisfied” responses were reported by 50.0% of control patients, 77.4% of ES1 patients, and 90.0% of ES2 patients, with chi-square = 12.669 and p = 0.002. Satisfaction is a softer endpoint than HAMD or HAMA, but it matches the mood-score direction.
Earlier ketamine and esketamine trials established rapid antidepressant effects in psychiatric contexts.2,3 Perioperative esketamine studies have also suggested reduced postoperative depressive symptoms in some surgical settings.4 Ding et al. add a colorectal-cancer surgery PCA context and explicitly separate mood from pain-score improvement.
What This Trial Can and Cannot Support
Supported: in elderly colorectal cancer surgery patients, esketamine-sufentanil PCA lowered acute HAMD and HAMA scores at 24 and 72 hours compared with sufentanil-only PCA, without clear pain-score superiority or higher adverse-event rates.
Not supported: routine esketamine use for every postoperative patient, durable depression prevention, or superiority of the 2 mg/kg dose over 1 mg/kg for mood. The follow-up window was short, and the sample was narrow.
Best next test: larger multicenter trials should track delirium, sleep, opioid exposure, inflammation, pain trajectories, major depressive episodes at 30 and 90 days, and whether patients with preoperative depressive symptoms benefit more.
Evidence strength: this is randomized evidence, which is stronger than an uncontrolled postoperative mood series. The same design still leaves several uncertainties because the analyzed sample was 91 patients, the setting was elderly colorectal cancer surgery, and the outcome window ended at 72 hours. A statistically clean short-term HAMD/HAMA separation can justify more perioperative trials, but it is not the same as proving durable psychiatric prevention.
Scope: the result applies most directly to older patients receiving sufentanil PCA after colorectal cancer resection. It should not be generalized to non-cancer surgery, younger surgical patients, outpatient ketamine treatment, or routine antidepressant prescribing without trials that measure those groups directly. The useful claim is narrower, but still clinically testable.
Why the 72-Hour Window Is Both Useful and Limited
The first 72 postoperative hours are clinically important. Sleep is disrupted, inflammation rises, opioids and anesthetic residues can affect cognition, and patients are processing pain, immobility, cancer-related fear, and loss of control. A mood intervention that works in that window could improve early recovery experience even if it does not prevent long-term depression.
That same window also limits interpretation. HAMD and HAMA scores measured 24 hours after surgery can capture acute distress, sleep loss, nausea, sedation, delirium risk, or physical discomfort in addition to depressive and anxious mood. Ding et al. partly addressed this by showing no pain-score explanation, but acute postoperative scales remain different from a psychiatric diagnosis.
Practical interpretation: the trial supports an acute postoperative mood-state effect. It should be read as perioperative neuropsychiatry evidence rather than long-term prevention evidence for major depressive disorder after cancer surgery.
The Low-Dose Signal Is Clinically Relevant
The 1 mg/kg esketamine group performed at least as well as the 2 mg/kg group on several mood readouts. That matters because perioperative esketamine use has to balance mood benefit, psychotomimetic effects, blood pressure, nausea, sedation, dissociation, and interactions with the rest of the anesthetic plan.
A higher dose did not clearly outperform the lower dose when the endpoint was mood in an older surgical population. The trial’s pattern points toward a dose-finding question: what is the lowest esketamine exposure that produces mood benefit without adding recovery-room complexity?
Next design detail: future trials should compare dose levels with prespecified noninferiority or dose-response logic and then test whether any esketamine arm beats control.
That question is especially important in older surgical patients, where small medication burdens can change blood pressure, cognition, sleep, mobilization, and discharge planning.
Questions About Esketamine PCA After Surgery
Did esketamine work by reducing pain?
The trial does not support that as the main explanation. Pain scores and PCA bolus demands did not differ significantly by group, while mood scores did.
Was the higher esketamine dose better?
Not clearly. Both esketamine groups improved mood scores versus control, and the 1 mg/kg group often looked similar to or better than 2 mg/kg on acute mood scales.
Does this prove esketamine prevents postoperative depression?
No. The trial measured acute depression and anxiety scores through 72 hours. Preventing a later depressive episode is a different outcome.
What is the practical use of the finding?
It supports studying esketamine as a perioperative mood-modulating adjunct in high-risk surgical groups, especially where opioid PCA is already being used and mood outcomes are measured directly.
References
- Ding L, Wang G, et al. Esketamine-sufentanil PCA reduces postoperative depression state in elderly colorectal cancer patients: a randomized controlled trial. Scientific Reports. 2026. doi:10.1038/s41598-026-49287-4
- Berman RM, Cappiello A, Anand A, et al. Antidepressant effects of ketamine in depressed patients. Biological Psychiatry. 2000. doi:10.1016/s0006-3223(99)00230-9
- Popova V, Daly EJ, Trivedi M, et al. Efficacy and safety of flexibly dosed esketamine nasal spray combined with a newly initiated oral antidepressant in treatment-resistant depression. JAMA. 2019. doi:10.1176/appi.ajp.2019.19020172
- Gan SL, Long YQ, Wang QY, et al. Effect of esketamine on postoperative depressive symptoms in patients undergoing thoracoscopic lung cancer surgery: a randomized controlled trial. Frontiers in Psychiatry. 2023. doi:10.3389/fpsyt.2023.1128406