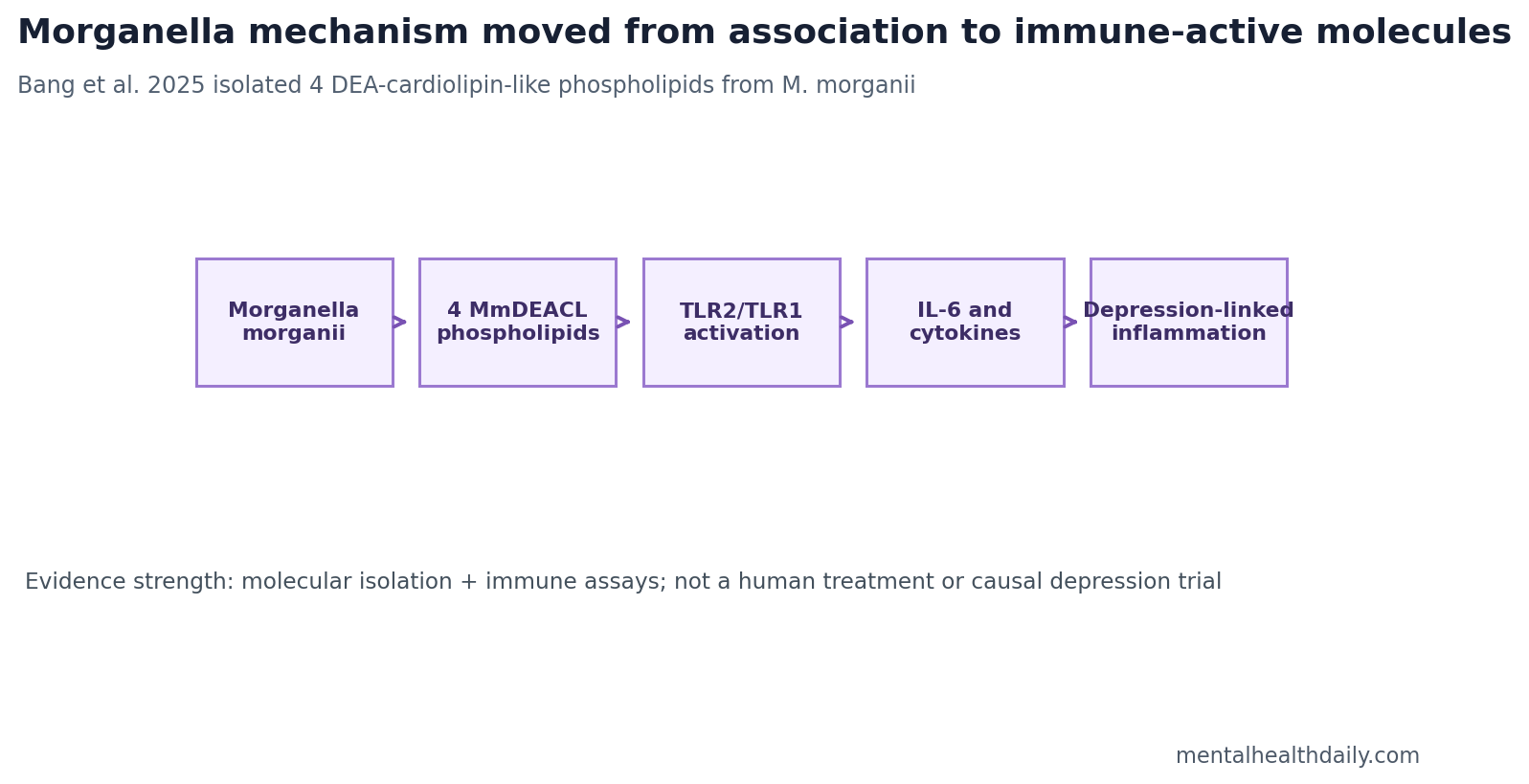
A 2025 Journal of the American Chemical Society study identified 4 unusual Morganella morganii phospholipids that activated TLR2/TLR1 immune receptors and induced inflammatory cytokines, especially IL-6.1 The finding does not prove that one gut bacterium causes depression, but it gives the microbiome-depression field something it often lacks: a named molecule and a receptor pathway.
Research Highlights
- 4 molecules were isolated: Bang et al. identified 4 closely related Morganella-derived MmDEACL phospholipids after bioassay-guided fractionation.1
- Innate immune receptors responded: The molecules activated TLR2/TLR1, a receptor pair that detects microbial lipid patterns.1
- IL-6 was a key output: The phospholipids induced pro-inflammatory cytokines, especially IL-6, a cytokine repeatedly linked to depression biology.1,3
- The chemistry was unusual: Diethanolamine replaced the central glycerol in a cardiolipin-like framework, creating DEA-cardiolipin molecular chimeras.1
- Clinical inference stays limited: The study tested bacterial molecules and immune assays, not 1 depression treatment trial or patient-screening protocol.1
Morganella morganii is a Gram-negative facultative anaerobe found in the environment and intestinal tract. It is usually treated as an opportunistic pathogen, but microbiome studies have also connected its abundance with inflammatory diseases and major depressive disorder.
MmDEACLs are the molecule family Bang et al. named: Morganella-derived diethanolamine cardiolipin-like phospholipids. In plain English, these are unusual bacterial membrane-like lipids that blend a cardiolipin framework with diethanolamine, a small industrially produced chemical that can enter lipid metabolism.
Bioassay-Guided Fractionation Found 4 Immune-Active Lipids
Bang et al. did not begin with a depression symptom scale. They began with a mechanistic problem: prior human data had linked Morganella with major depressive disorder, but association did not identify the molecule that might talk to the immune system.1
The researchers extracted Morganella morganii M11 material and tested fractions in murine bone-marrow-derived dendritic cells. After 2 rounds of chromatographic separation and functional assay, a single multicomponent fraction carried the activity. Further purification identified 4 related MmDEACL molecules.1
TLR2/TLR1 Turns a Gut Molecule Into an Immune Signal
Toll-like receptors are innate immune sensors that recognize microbial patterns. TLR2 often works with partner receptors, including TLR1, to detect bacterial lipids and trigger inflammatory signaling.4
Bang et al. found that the Morganella phospholipids activated TLR2/TLR1 and induced cytokines including TNF, IL-10, and especially IL-6.1 That receptor-level detail matters because it turns a loose gut-brain claim into a testable immune pathway.
IL-6 is an inflammatory cytokine involved in immune signaling, fever biology, metabolism, and stress-system communication. Dowlati et al. found elevated inflammatory cytokines including IL-6 in major depression across studies, although cytokine elevation is neither universal nor specific to depression.3
The Depression Link Is Mechanistic Plausibility, Not Clinical Proof
Valles-Colomer et al. showed that gut microbiome features and microbial neuroactive potential can associate with quality of life and depression in population data.2 Those studies are useful but often leave the field with the same problem: which organism, which molecule, which receptor, and which host pathway?
Bang et al. answer part of that chain. Morganella can produce immune-active phospholipids; those phospholipids can activate TLR2/TLR1; that activation can induce cytokines linked to depressive biology.1
The missing link is clinical causality. The paper does not show that high Morganella abundance causes a depressive episode, that MmDEACLs circulate at sufficient human concentrations, or that blocking TLR2/TLR1 improves mood.
It also does not collapse depression into inflammation. Cytokine signals are one plausible route into fatigue, anhedonia, sleep disruption, psychomotor slowing, and stress-system activation, but major depression remains heterogeneous. The molecule-level result is useful precisely because it can be tested inside an inflammatory subgroup instead of being stretched across every depressive presentation.
Why the Chemistry Is More Important Than the Microbiome Headline
Microbiome-depression coverage often gets stuck at the organism level: more of bacterium X, less of bacterium Y. That is rarely enough. Bacteria can be passengers, compensation signals, diet markers, medication markers, or true drivers depending on context.
Bang et al. move the question down a level. The 4 MmDEACLs differed in fatty-acid side chains, including C16:1, cyclopropane C17:0, C18:1, and cyclopropane C19:0 variants.1 That chemical specificity creates measurable targets for stool, plasma, cell, and animal studies.
Best next tests: measure these molecules in human stool and blood, compare depressed and non-depressed cohorts while controlling diet and medication, test whether levels predict IL-6 or other inflammatory markers, and run animal studies that separate Morganella colonization from purified molecule exposure.
What This Study Can and Cannot Support
Supported: one Morganella strain can make unusual phospholipids that activate innate immune receptors and induce inflammatory cytokines in experimental assays. The molecule-level mechanism fits broader cytokine-depression literature.
Not supported: microbiome testing for depression, antibiotics for mood, probiotic treatment claims, or certainty that Morganella is harmful in every host. Immune activation can depend on strain, molecule abundance, gut barrier state, host genetics, diet, and existing inflammation.
Clinical interpretation: the result is not ready for consumer action. It is a stronger research target: a named bacterial molecule family that can now be measured, blocked, or reproduced in better causal designs.
Strain, Barrier, and Host Context Could Decide the Effect
Microbiome findings often become too broad because the organism name is treated as the whole exposure. Morganella morganii is not one fixed clinical signal. Strains can differ in genes, metabolite production, growth conditions, and interaction with the surrounding microbial community.
Barrier context: immune-active bacterial lipids matter more if they reach host immune cells. Gut permeability, inflammatory bowel disease, infection, diet, medication, alcohol exposure, and metabolic disease could all influence whether a molecule produced in the gut becomes an immune signal with systemic consequences.
Host context: the same immune stimulus may produce different cytokine responses depending on TLR genetics, baseline inflammation, sex, age, obesity, stress physiology, and antidepressant or anti-inflammatory medication. That variability is one reason a molecule-level mechanism is more useful than a one-size-fits-all microbiome label.
What Would Make the Morganella Pathway Testable in Patients?
A useful clinical study would measure more than average Morganella abundance in depressed and non-depressed groups. It would measure the actual MmDEACL molecules, inflammatory markers including IL-6, gut-barrier markers, diet, medication, body mass index, infection history, and symptom dimensions such as fatigue, anhedonia, sleep disruption, and psychomotor slowing.
Best case for the pathway: higher MmDEACL exposure would predict a specific inflammatory depression phenotype, remain associated after confounder adjustment, and change with interventions that lower the molecule or block the receptor pathway. Without that chain, the finding remains a strong mechanistic lead rather than a clinical tool.
Depression heterogeneity: major depressive disorder groups together people with insomnia, hypersomnia, weight loss, weight gain, melancholic features, inflammatory illness, trauma exposure, medication effects, and metabolic disease. A gut-derived inflammatory molecule would probably apply to a narrower subgroup within that broad diagnostic category.
Most plausible target group: patients with depressive symptoms plus inflammatory markers, gut disease, metabolic dysfunction, or microbiome disruption may be more informative than an all-comers depression sample. Testing that subgroup logic would prevent a real signal from being diluted by patients whose depression is driven by other pathways.
That is also where microbiome work can become clinically serious. The goal is not to replace psychiatric diagnosis with stool taxonomy. The goal is to identify biological subtypes where a microbial molecule, immune pathway, and symptom pattern line up strongly enough to guide a targeted intervention.
For now, the safe conclusion is narrow: Morganella-derived lipids are worth measuring in inflammatory depression research, especially alongside cytokines and gut-barrier markers.
That is enough to move the question from loose association toward testable immune mechanism in real patients, with measurable molecules and outcomes.
Negative-control logic: if future depression cohorts show Morganella abundance without detectable MmDEACLs, or MmDEACL exposure without IL-6 or related inflammatory shifts, the simple organism-to-mood story weakens.
Positive-control logic: if purified MmDEACLs reproduce immune activation across human immune-cell systems and track an inflammatory symptom profile, the mechanism becomes harder to dismiss as generic microbiome noise.
That is the value of chemistry in a field full of broad association. A named molecule family gives researchers something to quantify, block, dose, and falsify. Depression biology needs that level of specificity before a gut-bacteria finding should influence clinical decisions.
Until then, reader-facing restraint should sit beside the real mechanism. The study gives depression researchers a sharper immune target, but it does not give patients a microbiome diagnosis, a supplement plan, or a reason to treat Morganella as a universal enemy.
Questions About Morganella and Depression
Does Morganella morganii cause depression?
Not proven. The study shows a plausible molecule-to-immune pathway that could help explain prior associations. It does not establish individual clinical causality.
Why is IL-6 important here?
IL-6 is one inflammatory signal repeatedly associated with depression in meta-analytic work. It is not a depression-specific marker, but it is a biologically plausible bridge between immune activation and mood symptoms.
Could diet or pollution exposure matter?
Possibly. Diethanolamine appears in the molecule structure, but the paper does not prove a real-world exposure route or dose-response relationship in humans.
What would make the evidence clinically meaningful?
Human studies would need to show that MmDEACL levels track depression risk, inflammatory state, or treatment response beyond confounders such as diet, medication, illness, and gut disease.
References
- Bang S, Shin YH, Park SM, et al. Unusual phospholipids from Morganella morganii linked to depression. Journal of the American Chemical Society. 2025. doi:10.1021/jacs.4c15158
- Valles-Colomer M, Falony G, Darzi Y, et al. The neuroactive potential of the human gut microbiota in quality of life and depression. Nature Microbiology. 2019. doi:10.1038/s41564-018-0337-x
- Dowlati Y, Herrmann N, Swardfager W, et al. A meta-analysis of cytokines in major depression. Biological Psychiatry. 2010. doi:10.1016/j.biopsych.2009.09.033
- Takeuchi O, Akira S. Pattern recognition receptors and inflammation. Cell. 2010. doi:10.1016/j.cell.2010.01.022