
A 2026 medRxiv meta-analysis of 27 trials found that transcranial direct current stimulation added to cognitive training improved global cognition immediately after treatment by SMD 0.36 compared with cognitive training alone.1 The signal was small, short-term, and rated very low certainty, so it is not evidence that tDCS is a durable cognitive-rehabilitation shortcut.
Research Highlights
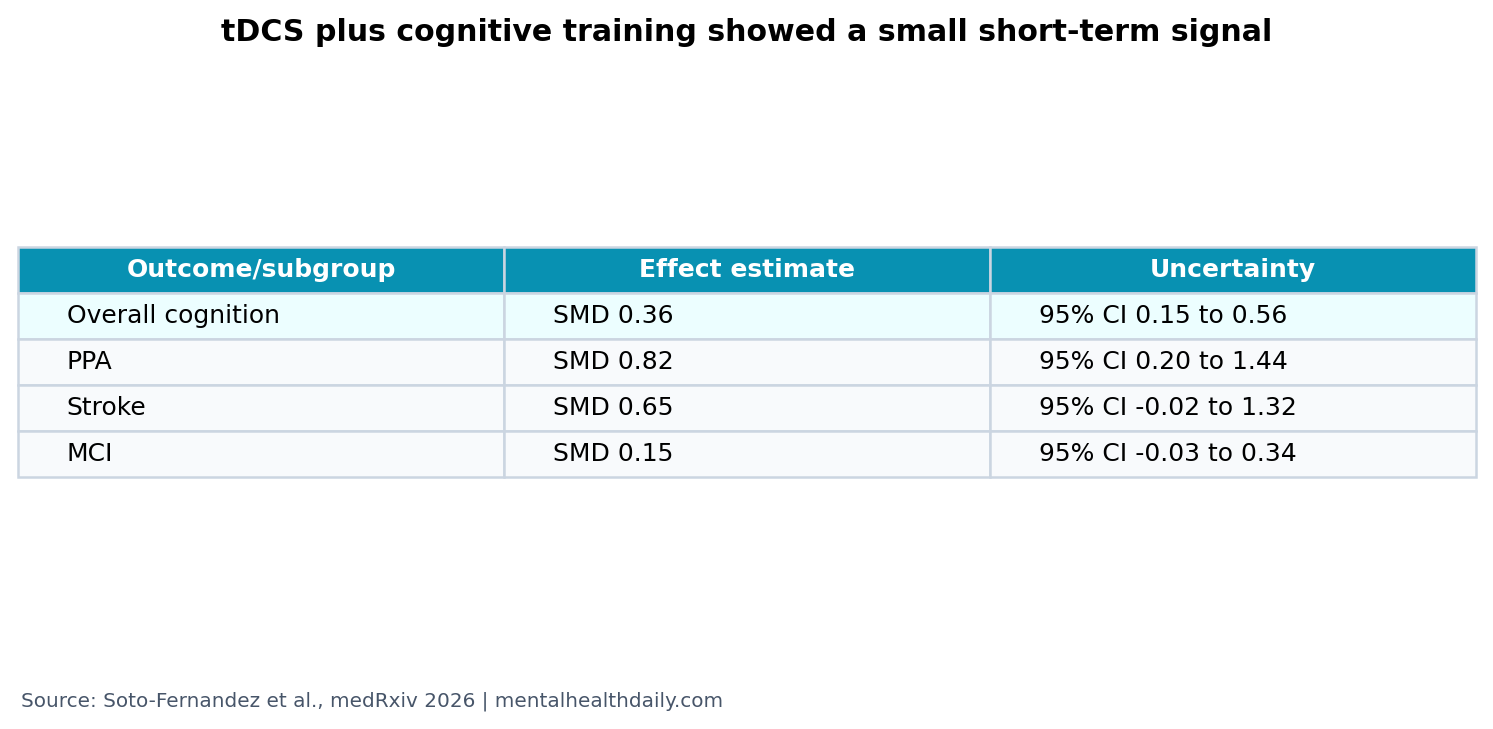
- Short-term cognition improved: pooled global cognitive performance favored tDCS plus cognitive training (SMD 0.36, 95% CI 0.15 to 0.56; p = 0.0006).1
- The evidence base was broad: the review included 27 studies and 1,012 participants across stroke, MCI, Alzheimer’s disease, HIV, multiple sclerosis, and PPA contexts.1
- Durability was the weak point: effects declined across follow-up periods, including samples of 365, 433, and 135 participants at later time windows.1
- Subgroups varied: PPA showed SMD 0.82, while MCI showed SMD 0.15 and crossed close to no effect.1
- Certainty stayed low: heterogeneity was moderate (I2 = 55%) and GRADE certainty for global cognition was very low.1
Transcranial direct current stimulation (tDCS) applies weak electrical current through scalp electrodes to shift cortical excitability. It does not “turn on” a brain region like a switch; it nudges the likelihood that neurons fire while a network is already active.
Cognitive training means structured practice on memory, attention, language, executive function, or other cognitive tasks. Pairing tDCS with training is meant to stimulate the network while that network is being used, potentially strengthening learning-related plasticity.
Global Cognition Improved by SMD 0.36 Immediately After Treatment
Soto-Fernandez et al. pooled controlled trials comparing tDCS plus cognitive training with cognitive training alone. The primary global cognitive estimate favored the add-on approach: SMD 0.36 (95% CI 0.15 to 0.56; Z = 3.44; p = 0.0006).1
Standardized mean difference puts different cognitive scales on a common metric. An SMD of 0.36 is a small-to-modest average effect. It is not trivial, but it is also not the kind of effect that should be sold as obvious clinical transformation.
The comparison is important. The add-on group was not being compared with doing nothing; it was compared with cognitive training or stimulation alone as defined by the included trials. The result therefore asks whether tDCS adds something above an active rehabilitation context.
Follow-Up Effects Faded Instead of Strengthening
The immediate post-treatment window carried the main effect. The paper described progressive attenuation across follow-up periods, with unstable estimates at 3 to 6 weeks, 3 to 4 months, and 6 to 7 months.1
That pattern matters because cognitive rehabilitation is judged by persistence as well as post-session test movement. A short-term boost may reflect practice effects, arousal, task engagement, or genuine plasticity that does not consolidate without maintenance sessions.
Clinical implication: the current evidence supports studying timing, dose, maintenance, and patient selection. It does not support treating one short stimulation course as a durable intervention for cognitive decline.
PPA and Stroke Looked More Promising Than MCI
Subgroup estimates differed by condition. Primary progressive aphasia showed the largest estimate (SMD 0.82, 95% CI 0.20 to 1.44). Stroke-related cognitive impairment showed SMD 0.65 (95% CI −0.02 to 1.32), a directionally favorable estimate that crossed the no-effect line.1
Mild cognitive impairment showed SMD 0.15 (95% CI −0.03 to 0.34), while multiple sclerosis was close to zero (SMD 0.07, 95% CI −0.55 to 0.69).1
Reader translation: the pooled average hides different clinical situations. A language-network rehabilitation task in primary progressive aphasia is not the same intervention problem as broad memory support in MCI or diffuse cognitive symptoms in multiple sclerosis.
Very Low Certainty Keeps the Result in the Testing Zone
The review rated global cognition evidence as very low certainty. The main problems were imprecision, heterogeneity, and variation in protocols, populations, scales, and follow-up.1
Heterogeneity means trial results disagreed more than expected from sampling error alone. The global cognitive analysis had I2 = 55%, a moderate level of disagreement. That does not erase the pooled effect, but it reduces confidence that one average estimate predicts the result for a new clinic, device montage, disease group, or training program.
tDCS physiology also supports caution. Stagg and Nitsche described tDCS as a cortical-excitability modulator rather than a direct treatment for cognition.2 Polania et al. emphasized that non-invasive stimulation effects depend on network state, task context, and stimulation parameters.3
Pairing Stimulation With Training Is the Mechanistic Point
The best case for tDCS is not passive stimulation. The mechanistic argument is state dependence: if a cognitive network is active during training, stimulation may bias plasticity in the same network. That is why this review focused on tDCS combined with cognitive therapy or cognitive stimulation.
Wu et al. reached a similar broad conclusion in an umbrella review of non-invasive stimulation for cognitive impairment: effects vary by technique, condition, outcome, and study quality.4 Soto-Fernandez et al. add a more specific question about the add-on value of tDCS during cognitive training.1
Supported: tDCS paired with cognitive training may produce a small immediate cognitive benefit in mixed cognitive-impairment trials.
Not supported: stand-alone consumer stimulation claims, durable disease modification, or using the same montage and dose across unrelated cognitive disorders.
Better Trials Need Fewer Mixed Targets
The pooled review is useful because it summarizes the field, but the next step is less pooling and more precision. A trial in post-stroke cognitive impairment asks a different biological question than a trial in Alzheimer’s disease, primary progressive aphasia, or HIV-associated cognitive impairment.
Target selection: stimulation should match the cognitive function being trained. A language task, working-memory task, and global cognitive screen do not recruit the same network. Montage choice should follow the task network, not habit.
Dose and timing: the review included variable session numbers, intensities, durations, and follow-up periods. If the effect fades, maintenance schedules and booster sessions need direct testing rather than being assumed.
Outcome choice: global cognitive scales can miss domain-specific gains. Trials should prespecify whether they are trying to improve naming, attention, memory, executive function, daily functioning, or caregiver-rated independence.
Responder biology: baseline cognitive severity, lesion location, neurodegenerative stage, medications, sleep, depression, and cortical-excitability markers may all change response. If those factors are not measured, a trial can report a small average effect while hiding a meaningful responder subgroup.
That is why the small pooled benefit should not be dismissed as meaningless or inflated into a treatment breakthrough. It is a development signal. The therapy concept deserves better-designed trials, not broader claims.
A practical trial would measure function alongside cognitive-test scores. If tDCS improves a memory task but leaves medication management, communication, work participation, or caregiver burden unchanged, the clinical value is limited. If a small test-score change predicts better daily functioning in a subgroup, the same SMD becomes more meaningful.
Adverse events and tolerability also belong in the efficacy equation. tDCS is usually described as low risk, but stimulation discomfort, skin irritation, headache, fatigue, dropout, and feasibility in older or neurologically impaired adults can decide whether a protocol is usable outside a trial.
The review also makes a quiet point about cognitive training itself. If the control condition is active training, then a positive add-on effect is harder to obtain than a placebo comparison. That makes SMD 0.36 more interesting, but it also means the clinical question is not “tDCS or no treatment.” It is whether stimulation adds enough benefit to justify equipment, supervision, and protocol complexity.
That threshold will probably differ by condition. A small add-on gain may be worthwhile in a rehabilitation clinic with trained staff and a targeted language protocol, but far less persuasive for broad memory complaints in community settings today, especially without follow-up durability.
Trial-quality requirement: sham stimulation has to remain believable, and training adherence has to be measured. If participants can guess their group or if the active arm completes more training, the apparent stimulation benefit may partly reflect expectancy, discomfort cues, therapist contact, or practice dose rather than cortical modulation.
Reporting should also separate near-transfer task gains from broad cognitive improvement. Better performance on trained material is useful, but it is weaker than improvement on untrained daily-life functions.
Clinical relevance begins with transfer.
Without transfer, the device claim stays narrow.
That distinction protects interpretation.
Questions About tDCS and Cognitive Training
Is tDCS proven to improve cognition?
Not in a broad clinical sense. This review found a small immediate add-on effect, but certainty was very low and follow-up durability was weak.
Why combine tDCS with cognitive training?
tDCS may work best when the target network is active. Cognitive training supplies the task engagement that stimulation alone lacks.
Which condition looked most promising?
Primary progressive aphasia had the largest subgroup estimate, but the confidence interval was wide. It should be treated as a signal for better trials, not a settled ranking.
Should people use home tDCS devices for memory?
This evidence does not support unsupervised use. The trials involved structured protocols, clinical populations, and cognitive training comparators.
References
- Soto-Fernandez P, Toledo-Rodriguez L, Figueroa-Vargas A, Figueroa-Taiba P, Billeke P. Effects of transcranial direct current stimulation (tDCS) combined with cognitive therapy in individuals with cognitive impairment: a systematic review and meta-analysis. medRxiv. 2026. doi:10.64898/2026.04.26.26351755
- Stagg CJ, Nitsche MA. Physiological basis of transcranial direct current stimulation. The Neuroscientist. 2011;17:37-53. doi:10.1177/1073858410386614
- Polania R, Nitsche MA, Ruff CC. Studying and modifying brain function with non-invasive brain stimulation. Nature Neuroscience. 2018;21:174-187. doi:10.1038/s41593-017-0054-4
- Wu M, Song W, Wang X, et al. Efficacy of non-invasive brain stimulation interventions on cognitive impairment: an umbrella review of meta-analyses of randomized controlled trials. Journal of NeuroEngineering and Rehabilitation. 2025;22:22. doi:10.1186/s12984-025-01566-3