Cannabis users often say the drug helps them blunt stressful memories. A 2026 randomized trial of 36 healthy adults tested low-dose oral THC against placebo during retrieval of a standardized lab stressor, and on every subjective and physiological measure that mattered, THC did nothing.1
Research Highlights
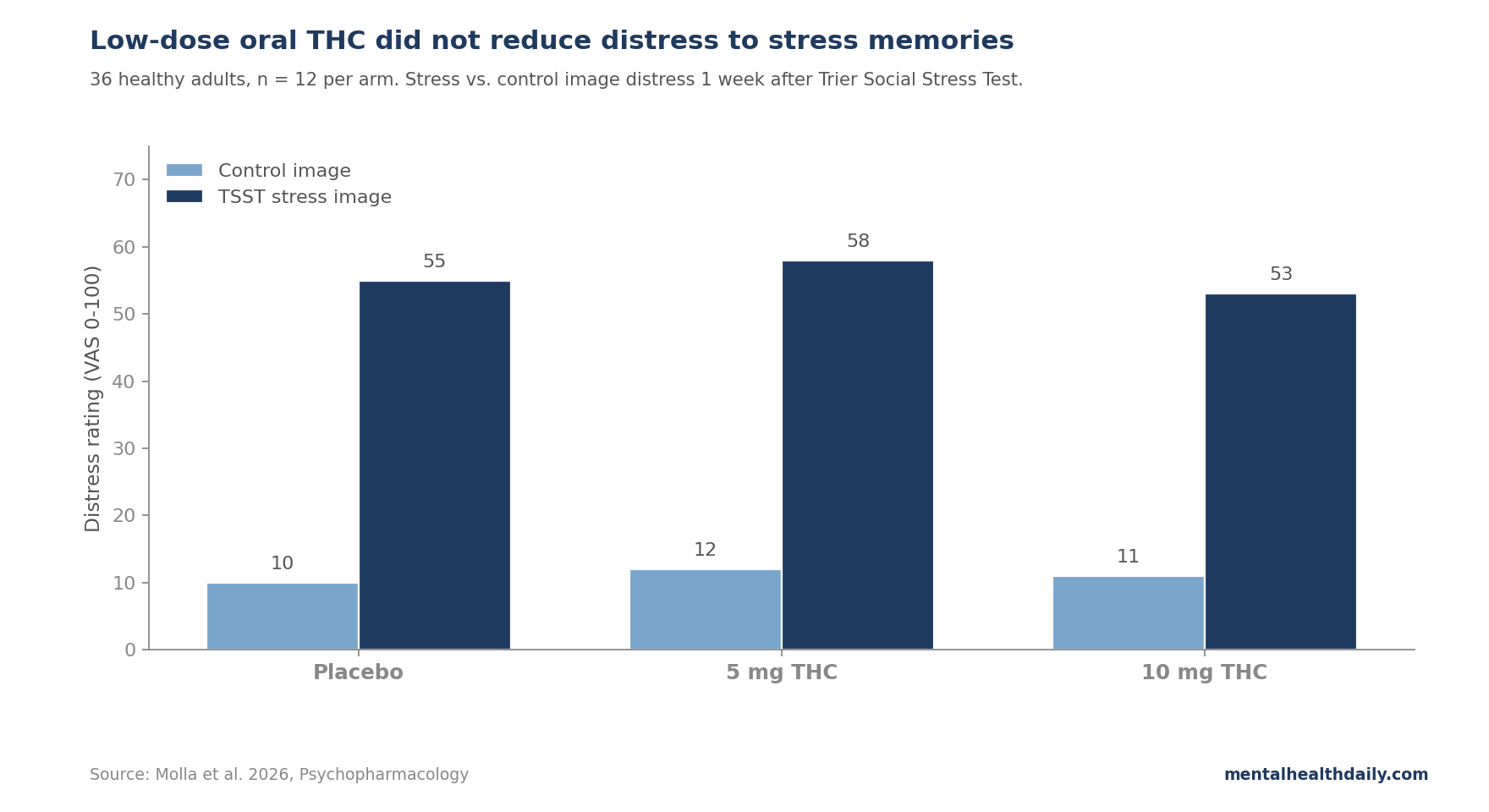
- 36-adult, 3-arm RCT: participants got placebo, 5 mg oral THC, or 10 mg oral THC (n = 12 per arm) before retrieving memories of a Trier Social Stress Test (TSST) administered 1 week earlier.1
- 5-minute TSST stress memory: a mock job-interview speech plus a mental-arithmetic task in front of stern-faced evaluators raised distress, arousal, heart rate, and salivary cortisol relative to a Bob Ross painting video control (p < 0.0001 for each). Stress images presented 1 week later still elicited substantial distress and arousal in placebo participants.1
- Active THC, no distress reduction: both 5 and 10 mg significantly increased “feel drug” and “high” ratings (p = 0.02 and p = 0.001), confirming the doses were active. Neither dose reduced distress, arousal, valence, or feelings of control during stress-image retrieval.1
- BF₁₀ below 0.10: all values were below 0.10 for the primary subjective outcomes — meaning the data were >10x more consistent with no THC effect than with the hypothesized THC effect, even with the small sample.1
- 1 expressive dissociation: stress images normally elicited self-conscious smiling; THC blunted that response (p = 0.02). Self-reported distress did not change in parallel, suggesting THC may decouple inner emotional state from outward expression.1
The lab-and-market expectation around cannabis as a stress reliever is large — around 40% of US young adults have used cannabis, and stress relief is one of the top self-reported reasons.1 The endocannabinoid system is also a real target: cannabinoid type 1 (CB1) receptors are dense in stress and emotion regulation regions, including amygdala and prefrontal cortex, and pharmacologically boosting endocannabinoid signaling has shown stress-dampening effects in animals and some human work.2
What is murkier is whether exogenous THC at the doses people actually take recreationally meaningfully reduces subjective stress and stress-memory recall in humans. The Molla trial is small but methodologically clean and arrives at a clear null on the central question.
The Trier Social Stress Test as a Stress-Memory Engine
The trial’s clever piece is using the Trier Social Stress Test (TSST) — a standardized public-speaking-and-arithmetic task performed in front of a stern panel — to manufacture a personally relevant stress memory in the lab. Researchers video-recorded each participant during the TSST and during a calm control task (watching Bob Ross paint), then 1 week later played back 20-second clips while participants rated their distress.
This is more controlled than studying real-world traumatic memories, where exposure type, intensity, and time-since-event vary across participants. Every participant’s stress memory was the same age, the same kind of stressor, and elicited a baseline response that could be benchmarked against a within-subject neutral control.
The TSST induction worked as expected:
- Distress (visual analog scale 0–100): increased post-TSST vs. post-control (F(1,34) = 114.6, p < 0.0001).
- Arousal (VAS): increased (F = 116.2, p < 0.0001).
- Heart rate: elevated (F = 67.8, p < 0.0001).
- Salivary cortisol: 10-minute post-TSST levels rose (F = 12.8, p = 0.001), with a stronger response in males (sex interaction p = 0.02).
1 week later, presenting the participant’s own TSST clips reliably re-elicited distress, arousal, and lower valence compared with their own control clips — replicating earlier work showing that stress-image cues retain their affective power across days.3
Low-Dose Oral THC Did Not Dampen Subjective or Physiological Stress-Memory Responses
2 hours after capsule ingestion (peak plasma THC), participants viewed their own TSST and control clips while researchers measured subjective distress and cardiovascular sympathetic activation (pre-ejection period, or PEP — a beat-to-beat measure of sympathetic drive on the heart, where shorter intervals reflect more sympathetic activation).
The pattern was uniform across measures. Stress images raised distress, raised arousal, lowered valence, and lowered ratings of being “in control” relative to control images (all p < 0.0001 for image-type main effect). And in every case, the THC arms showed the same response as placebo — no significant drug-by-image-type interaction on any of the 4 primary subjective measures.1
PEP showed no image-type difference (p = 0.8) but a marginal drug effect across all images (p = 0.07), suggesting some non-specific cardiovascular activation rather than a stress-memory dampening signal. Heart rate followed the same pattern.
The drug arms’ subjective effects confirmed dosing was real. Both 5 and 10 mg raised “feel drug” ratings vs. placebo (p = 0.02), and 10 mg also raised “dislike drug” ratings (p = 0.02) — consistent with a sample of light cannabis users (around 1–2 uses in the past 30 days). Both doses raised confusion (POMS Confusion subscale, p = 0.002) but neither raised anxiety scores.
Bayes Factors Argue This Is Not a Power Problem
The first reflexive critique of any null trial with n = 12 per group is “underpowered.” Molla et al. addressed this directly with Bayes factor analysis, which compares how much better the data fit the no-effect model vs. an alternative-effect model.
For all 4 primary subjective outcomes during stress retrieval (distress, arousal, valence, in-control), Bayes factors were below 0.10. Plain English: the data were more than 10 times as consistent with no THC effect as with the hypothesized stress-dampening effect. Conventional thresholds treat BF₁₀ < 0.33 as “moderate” evidence for the null and BF₁₀ < 0.10 as “strong” evidence for the null.1
At these doses, in this sample, with this paradigm, the absence of effect is unlikely to be a Type II error. A post-hoc power calculation suggested 15 per group would be needed to detect an effect of the size that Childs et al. 2017 reported for low-dose THC during acute stress (Cohen’s f = 0.44).4
THC could still affect stress memories under different dosing, timing, or memory-reactivation conditions, but this trial did not show that pattern.
Acute Stress Is Not the Same as Stress-Memory Retrieval
The Childs et al. 2017 study is the clearest counterweight. In that trial, 7.5 mg oral THC reduced VAS distress ratings during the live TSST, while a higher 12.5 mg dose backfired and increased negative mood and impaired performance.4
The Molla finding that THC failed to dampen memory retrieval, despite the same stressor, supports a clinically important distinction: dosing the drug while a person is actively in the stressor may engage HPA-axis dampening pathways differently than dosing while they are remembering it.
Acute social-evaluative stress reliably activates the hypothalamic-pituitary-adrenal (HPA) axis — cortisol rises, heart rate climbs, sympathetic drive increases.5 Stress-memory retrieval, in contrast, primarily engages cognitive and affective brain networks (medial prefrontal cortex, hippocampus, amygdala) without necessarily reactivating the full HPA cascade.
Endocannabinoid effects on the HPA axis are well-documented in animals; effects on cognitive-emotional memory retrieval circuits in humans are less so. The Molla null is consistent with the idea that THC’s stress-dampening effects sit upstream in the acute stress response, not downstream in memory retrieval.
THC Reduced Self-Conscious Smiling Without Reducing Distress
The 1 measure where THC moved the needle was self-conscious smiling. When placebo participants saw their own TSST clips, they smiled more than when watching their own Bob Ross clips — a kind of social embarrassment response. Both 5 and 10 mg THC blunted that increase (drug-by-cue interaction p = 0.02).1
Smiling here is not a positive emotion signal. It is a documented stress-induced facial response that may serve as nonverbal emotion regulation in social-evaluative contexts, and the Trier paradigm itself is known to elicit it.6 Reducing it could reflect:
- Dampened motivation to self-monitor. THC may reduce the social-monitoring drive that produces self-conscious smiling, even while subjective distress is unchanged.
- Affect blunting more broadly. Earlier work has shown THC can reduce reactivity to social and affective cues, possibly via amygdala-prefrontal modulation.7
- Decoupling of inner experience and outer expression. If subjective distress stayed flat but expressive behavior changed, the drug may have broken the normal link between the 2 — a finding consistent with anecdotal reports of cannabis-related “flat” affect.
This is interesting, but it should not be confused with stress reduction. A drug that leaves people feeling equally stressed but smiling less is not obviously therapeutic.
How This Lands Inside the Cannabis-for-PTSD Literature
The result calibrates rather than refutes the broader cannabis-for-stress hypothesis, but it does push back on the simplest version of it. The clinical-trial track record for cannabis in PTSD is weaker than the cultural narrative implies.
Bonn-Miller et al. 2021 ran a phase 2 RCT comparing 3 smoked cannabis preparations (high-THC, high-CBD, mixed THC+CBD) against placebo over 3 weeks in 80 US veterans with PTSD. None of the active arms outperformed placebo on the primary CAPS-5 PTSD severity outcome. All groups improved similarly, suggesting placebo response and time effects, not cannabis-specific benefit.8
On the encouraging side, Rabinak et al. 2013–2014 work in healthy adults showed that low-dose oral THC (7.5 mg) during fear-extinction learning enhanced extinction recall the next day, with parallel changes in ventromedial prefrontal cortex activation.9 That suggests CB1 agonism may help new safety learning, even if it doesn’t blunt retrieval of an already-formed stressful memory — the Molla finding.
The take-home: cannabinoid effects on stress and trauma memory appear to depend heavily on when in the stress-memory cycle the drug is administered (during acute stress, during extinction learning, during retrieval), and on the user’s baseline experience. The Molla trial cleanly tests retrieval and finds THC does not help.
Limitations and What This Trial Cannot Tell You
Sample size and population. 36 light cannabis users aged 18–35 with no major psychiatric disorders. Results may not generalize to clinical PTSD populations, frequent cannabis users, older adults, or people with anxiety disorders. The Bayes factor protects against Type II error within this sample but cannot extend the inference outside it.
Dose range. 5 and 10 mg oral THC are the low-recreational range. Childs et al. 2017 found that 7.5 mg reduced acute stress while 12.5 mg backfired — suggesting a narrow therapeutic window. Whether intermediate or different dosing routes (sublingual, inhaled) would behave differently is untested.
Stress memory salience. The TSST is a standardized stressor but not a personally meaningful trauma. THC effects on emotionally intense, naturally formed stress memories may differ.
Acute vs. chronic dosing. The trial tests a single oral dose. Chronic-use scenarios — and the tolerance, sensitization, or expectancy that come with them — are outside the design.
No CBD arm. THC and CBD have opposing effects on anxiety in some paradigms; CBD has its own emerging stress-related literature. This trial isolates THC, which is a strength for mechanism but a limitation for cannabis-product translation.
Practical Read for Cannabis-as-Stress-Relief Users
- Acute stress and stress-memory retrieval are separate problems. Low-dose THC may modestly reduce distress during a live stressor (Childs 2017), but does not appear to reduce distress when retrieving a stress memory (Molla 2026). The 2 are not interchangeable.
- The dose window is narrow. Low doses (around 7.5 mg oral) sit in the “possibly modestly anxiolytic for acute stress” zone. Higher doses tip into anxiogenic in many people. Chasing more is a bad strategy if stress relief is the goal.
- Cannabis-for-PTSD evidence is weaker than the marketing suggests. The largest controlled trial in US veterans (Bonn-Miller 2021) found no benefit over placebo at 3 weeks. Trauma-focused psychotherapies (CPT, prolonged exposure) and SSRIs remain the first-line evidence-based options.
- The smiling result is interesting but not therapeutic. Reduced self-conscious smiling without reduced distress is at best a behavioral marker, at worst a sign of expressive blunting. Neither reads as “cannabis treats stress.”
Questions About THC, Stress, and Memory
Does this mean cannabis doesn’t reduce anxiety?
Not exactly. Cannabis can reduce subjective distress during acute stress at low doses, and frequent users often report relief, but controlled-trial evidence for sustained anxiety or PTSD benefit is thin and mixed.8
The Molla trial specifically tests stress-memory retrieval, where THC did not help. Other paradigms (acute stress, fear extinction learning) show more variable results.
Why is this different from earlier studies showing THC reduces stress?
Timing. Childs et al. 2017 dosed THC immediately before the TSST and saw stress-dampening; Molla dosed before memory retrieval, 1 week after the original stressor. Acute stress engages the HPA axis and sympathetic system, which endocannabinoids regulate directly. Memory retrieval engages cognitive-affective networks where THC’s effects appear weaker.4
Should cannabis be considered for PTSD?
The largest controlled trial to date (Bonn-Miller et al. 2021) found no benefit over placebo for 3 weeks of smoked cannabis at clinically relevant doses in US veterans.8
Evidence-based PTSD treatments (cognitive processing therapy, prolonged exposure, EMDR, SSRIs) remain first-line. Cannabis may help individual symptoms (sleep, acute distress) for some users but is not a substitute for trauma-focused care.
What about CBD?
CBD has a distinct pharmacology (no CB1 agonism, multiple non-cannabinoid receptor effects) and a separate — if also limited — anxiety-modulation literature. The Molla trial does not address CBD.
Higher-quality CBD trials in social anxiety and generalized anxiety remain modest in size and effect; the case for CBD as a stress reliever is suggestive but unproven at scale.
Why did THC reduce smiling but not distress?
The most parsimonious interpretation is that THC affected expressive behavior more than inner experience — possibly by reducing the motivation to self-monitor, blunting affective responsiveness to social cues, or modulating amygdala-prefrontal circuits that link emotion to facial expression.7
It does not appear to reflect actual stress reduction, since participants’ self-reported distress was unchanged.
References
- Acute and delayed effects of THC on memories of stress in healthy adults. Molla H, Hahn E, Ramos C & de Wit H. Psychopharmacology. 2026. doi:10.1007/s00213-026-07064-1
- The endocannabinoid system as a target for novel anxiolytic drugs. Hill MN & Patel S. Neuroscience & Biobehavioral Reviews. 2017;76(Pt A):56-66. doi:10.1016/j.neubiorev.2016.10.027
- Generation and validation of a multisensory laboratory stress paradigm for studying memory of stressful events. Freund VA et al. Psychoneuroendocrinology. 2023;152:106086. doi:10.1016/j.psyneuen.2023.106086
- Dose-related effects of delta-9-THC on emotional responses to acute psychosocial stress. Childs E, Lutz JA & de Wit H. Drug and Alcohol Dependence. 2017;177:136-144. doi:10.1016/j.drugalcdep.2017.03.030
- Acute stressors and cortisol responses: a theoretical integration and synthesis of laboratory research. Dickerson SS & Kemeny ME. Psychological Bulletin. 2004;130(3):355-391. doi:10.1037/0033-2909.130.3.355
- You look stressed: a pilot study on facial action unit activity in the context of psychosocial stress. Blasberg JU et al. Comprehensive Psychoneuroendocrinology. 2023;15:100187. doi:10.1016/j.cpnec.2023.100187
- Cannabinoid modulation of amygdala reactivity to social signals of threat in humans. Phan KL et al. Journal of Neuroscience. 2008;28(10):2313-2319. doi:10.1523/JNEUROSCI.5603-07.2008
- The short-term impact of 3 smoked cannabis preparations versus placebo on PTSD symptoms: a randomized cross-over clinical trial. Bonn-Miller MO et al. PLOS ONE. 2021;16(3):e0246990. doi:10.1371/journal.pone.0246990
- Cannabinoid facilitation of fear extinction memory recall in humans. Rabinak CA et al. Neuropharmacology. 2013;64:396-402. doi:10.1016/j.neuropharm.2012.06.063