
A 2026 multi-cohort Alzheimer’s disease study found that MRI radiomics from the hippocampus and amygdala linked plasma pTau217 and smell identification to cognitive impairment — with more added cognitive signal than simple regional volume. The result is useful because it points to a possible bridge between blood biomarkers and brain-circuit damage, but it is still an associative machine-learning signal rather than a proven clinical diagnostic pathway.
Research Highlights
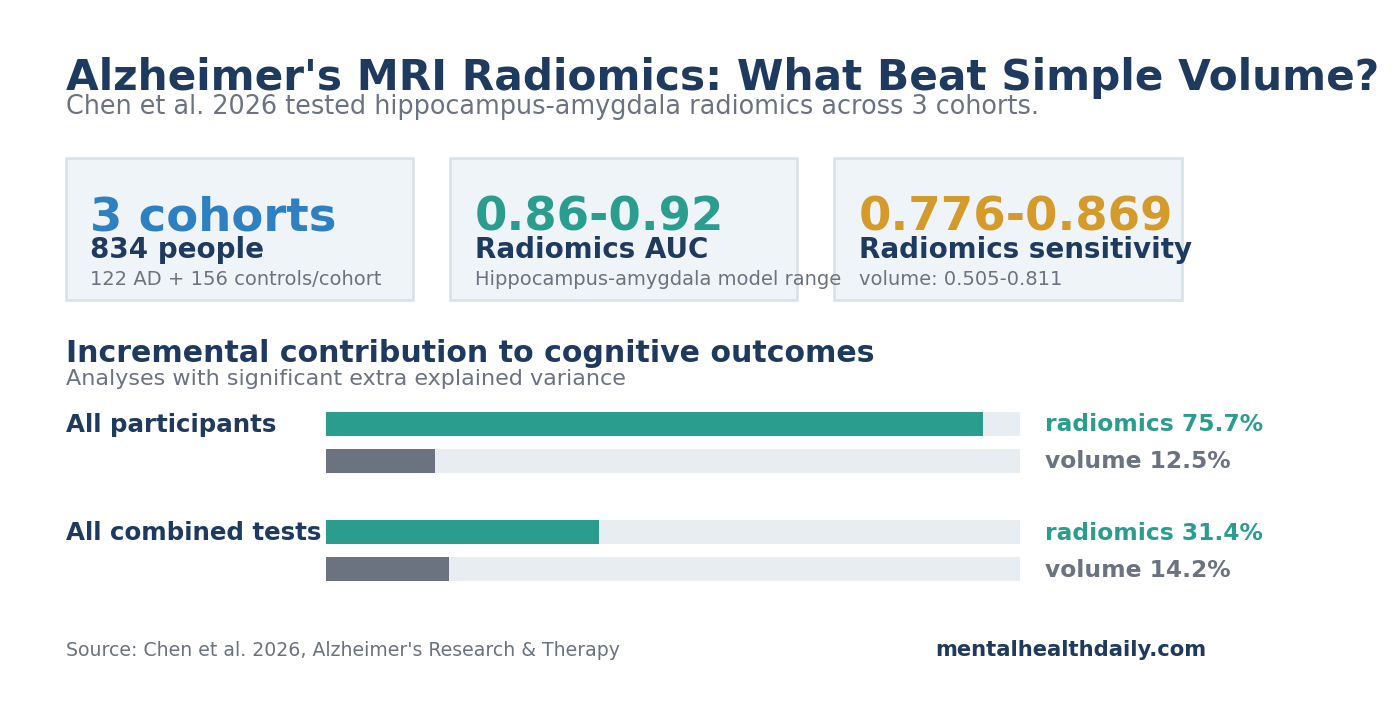
- Hippocampus-amygdala MRI texture performed best: Chen et al. tested 834 people across 3 cohorts and found that hippocampus-amygdala radiomics classified probable Alzheimer’s disease with AUC 0.86-0.92 and accuracy 0.81-0.88.1
- Radiomics improved sensitivity more than AUC: average AUC was only slightly higher for radiomics than volume, 0.872 vs. 0.868, but sensitivity ranged from 0.776-0.869 for radiomics vs. 0.505-0.811 for volume models.
- pTau217 and smell impairment converged on the same MRI signal: in the 1 in-house cohort, the hippocampus-amygdala radiomics score correlated with plasma pTau217, odor identification, and Mini-Mental State Examination (MMSE) cognition scores.
- Mediation results are mechanistic clues, not proof: selected radiomics features statistically mediated 26.9%-37.1% of the pTau217-to-cognition association and 26.6%-44.2% of the smell-to-cognition association.
- Clinical translation still needs biomarker-confirmed validation: Alzheimer’s diagnosis was clinical across 3 cohorts, plasma and smell testing were only available in the in-house cohort, and the design cannot show whether baseline MRI radiomics predicts future decline.
The interesting part is not that a machine-learning model separated Alzheimer’s disease from controls. Many MRI classifiers can do that under research conditions. The useful question is whether radiomics adds information that ordinary volume misses, especially in olfactory-limbic brain regions where tau pathology, smell impairment, and memory decline overlap.
Researchers Tested Olfactory MRI Radiomics in 834 People
Chen et al. developed and validated MRI radiomics models in 834 participants: an in-house Chinese cohort, an Alzheimer’s Disease Neuroimaging Initiative (ADNI) validation cohort, and an Open Access Series of Imaging Studies (OASIS) validation cohort. Each cohort included 122 people with probable Alzheimer’s disease and 156 cognitively unimpaired controls.1
Study snapshot:
- Design: cross-sectional MRI machine-learning study with 1 development cohort and 2 external validation cohorts.
- Participants: 366 people with probable Alzheimer’s disease and 468 cognitively unimpaired controls across all cohorts.
- Extra measurements: plasma pTau217, odor identification, and detailed cognitive testing were available in the in-house cohort.
Radiomics means converting medical images into many quantitative features that the eye does not directly read. In this study, the researchers extracted 1,502 features from each olfactory-related region of interest. Those features included shape, signal-intensity distribution, and texture patterns such as gray-level co-occurrence and run-length measures, which try to capture how MRI signal varies across neighboring voxels.
The olfactory framing is biologically plausible because smell impairment often appears before obvious dementia and because Alzheimer’s pathology affects connected olfactory-limbic structures. The hippocampus supports memory formation. The amygdala helps attach emotional and salience value to sensory information. The entorhinal and piriform cortices participate in smell processing. These regions are anatomically close to early Alzheimer’s disease pathways.
The in-house cohort had the richest phenotyping. People with Alzheimer’s disease had lower odor identification scores than controls, 6.45 ± 2.62 vs. 10.50 ± 2.55 correct on a 16-item smell test, and higher plasma pTau217, 0.80 ± 0.63 vs. 0.15 ± 0.12 pg/mL.
pTau217 means tau protein phosphorylated at threonine 217, a blood marker tied to Alzheimer’s-type tau biology. The same Alzheimer’s group had lower MMSE cognition scores across all cohorts.
Hippocampus-Amygdala Radiomics Beat Other Smell-Related Regions
The researchers compared radiomics from the piriform cortex, entorhinal cortex, orbitofrontal cortex, hippocampus, and amygdala. The combined hippocampus-amygdala model was the most stable performer after scanner harmonization, meaning the researchers adjusted MRI features so that scanner/site differences were less likely to masquerade as disease differences.
The best hippocampus-amygdala models reached AUC 0.86-0.92. AUC, or area under the receiver operating characteristic curve, measures how well a classifier ranks cases above controls across thresholds; 0.50 is chance, and 1.00 is perfect separation. Logistic regression and support vector machine models performed similarly, while random forest models were better calibrated for probability estimates.
Key model details were:
- Training and validation: the in-house cohort served as the development set, while ADNI and OASIS tested external generalization.
- Algorithms: support vector machine, logistic regression, random forest, LightGBM, Gaussian naive Bayes, and XGBoost were compared.
- Diagnostic range: the logistic regression model reached AUC 0.863 in the test set, 0.883 in ADNI, and 0.922 in OASIS.
- Sensitivity profile: logistic regression sensitivity was 0.811 in the test set, 0.869 in ADNI, and 0.926 in OASIS.
Why hippocampus-amygdala texture may work: the hippocampus and amygdala are downstream convergence hubs for smell, memory, emotional salience, and limbic disease spread.
Primary olfactory regions may be closer to the smell pathway, but hippocampus-amygdala texture may carry a more integrated burden of Alzheimer’s disease biology.
Radiomics Added More Than Simple Hippocampus and Amygdala Volume
Conventional volumetry asks whether a brain structure is smaller. Radiomics asks whether the MRI signal inside the structure has a disease-linked texture pattern. That distinction is the main clinical claim in this paper.
Across 6 algorithms and 3 cohorts, radiomics had only a small average AUC advantage over volume, 0.872 vs. 0.868. The larger difference was sensitivity: radiomics sensitivity ranged from 0.776-0.869, while volume-model sensitivity ranged from 0.505-0.811. In early-detection settings, sensitivity is not a trivial metric because false negatives can delay confirmatory biomarker testing and treatment evaluation.
The cognitive-prediction comparison was also stronger for radiomics. Hierarchical regression means the researchers first modeled cognition with clinical covariates and then tested whether adding a radiomics or volume feature explained extra variance. Radiomics features showed significant incremental contributions in 75.7% of all-participant analyses, compared with 12.5% for volume features. Across all combined analyses, radiomics remained ahead, 31.4% vs. 14.2%.
- AUC difference: small enough that radiomics should not be sold as a clean diagnostic replacement for volume.
- Sensitivity difference: large enough to matter if the goal is catching more true Alzheimer’s disease cases before confirmatory testing.
- Cognition difference: radiomics features more often explained extra variance beyond the base clinical model.
There is still a calibration issue. The volume models were competitive in external AUC, and volume performed better for some domains such as memory and executive function. A careful reading is that radiomics added information, not that volume became obsolete.
pTau217, Smell Identification, and Cognition Shared a Radiomics Signal
The in-house cohort allowed the most interesting analysis because it included plasma pTau217, a structured smell-identification test, and detailed cognitive testing. Across Alzheimer’s disease and control participants combined, the hippocampus-amygdala radiomics score correlated with MMSE cognition (r = −0.65), odor identification (r = −0.48), verbal fluency language performance (r = −0.45), processing speed (r = −0.49), and plasma pTau217 (r = 0.49), all after false-discovery-rate correction.
The negative correlations mean that higher radiomics abnormality tracked with worse cognition and worse odor identification. The positive pTau217 correlation means higher radiomics abnormality tracked with higher blood tau pathology. In the Alzheimer’s disease group alone, the radiomics score still correlated with MMSE (r = −0.28), while correlations in cognitively unimpaired controls were minimal.
The mediation analysis then tested whether radiomics statistically sat between tau or smell impairment and cognition. Mediation analysis is a statistical pathway model: it asks whether part of the association between 2 variables appears to pass through a third measured variable. It does not prove biology by itself, especially in cross-sectional data.
- pTau217 to cognition: 2 hippocampal radiomics features mediated 37.1% and 26.9% of the association between pTau217 and MMSE.
- Smell identification to cognition: the hippocampus-amygdala radiomics score mediated 26.6% of the smell-to-language association and 44.2% of the smell-to-memory association.
- Plain-English interpretation: tau biology, smell impairment, and cognitive impairment appeared to converge on hippocampus-amygdala MRI texture.
This is the strongest conceptual contribution of the study. It connects 3 measurement layers: a blood marker, a sensory test, and a structural MRI signature. Each layer is imperfect alone. Together, they sketch a testable Alzheimer’s disease pathway.
Blood Biomarkers Are Ahead of MRI Radiomics Clinically
Blood-test evidence is further along. Plasma pTau217 already has stronger clinical momentum than radiomics. Palmqvist et al. evaluated plasma phospho-tau217 in 1,767 symptomatic participants across primary and secondary care cohorts and reported strong diagnostic performance using an automated platform.2 A separate 2026 meta-analysis of 27 studies placed plasma pTau217 in a clinically useful blood-biomarker range for Alzheimer’s disease pathology.3
Radiomics fits downstream of molecular triage. Radiomics may complement that blood-test pathway rather than compete with it. A blood biomarker can say whether Alzheimer’s-type molecular pathology is likely. MRI radiomics may eventually help estimate where pathology has translated into brain-circuit injury and cognitive phenotype. That division of labor is more credible than treating an MRI texture model as a standalone diagnostic shortcut.
Biomarker confirmation remains the missing piece. The Alzheimer’s disease research framework already separates biological pathology from clinical syndrome. The 2018 National Institute on Aging-Alzheimer’s Association framework defined Alzheimer’s disease in research settings by amyloid, tau, and neurodegeneration biomarkers rather than symptoms alone.4
Chen et al. fit that biomarker logic, but the study did not biomarker-confirm every Alzheimer’s diagnosis with amyloid PET, tau PET, or cerebrospinal fluid.
Smell Testing Belongs in the Alzheimer’s Biomarker Conversation
Smell testing is cheap, fast, and biologically relevant, but it is not specific enough to diagnose Alzheimer’s disease. Many factors can impair smell, including viral injury, smoking, sinonasal disease, Parkinson’s disease, traumatic brain injury, medication effects, and normal aging. The value is triage and risk enrichment, not diagnosis.
Existing smell literature is supportive but non-specific. A systematic review and meta-analysis found large olfactory-identification deficits in Alzheimer’s disease.5
A 2021 review by Wheeler and Murphy summarized evidence that odor threshold, odor identification, and odor familiarity can help predict conversion to mild cognitive impairment or Alzheimer’s disease in older adults.6 A separate meta-analysis found that olfactory impairment predicted higher later risk of cognitive decline in older adults.7
Chen et al. added the imaging link. Lower odor identification was statistically tied to hippocampus-amygdala texture and cognition, which makes smell testing more interesting as part of a multimodal workup.
Limitations of This Radiomics Study
Evidence-strength note: this was a cross-sectional machine-learning and mediation study. It can show classification performance and statistical associations. It cannot show that MRI texture changes caused cognitive decline, that the model predicts future conversion, or that using the model improves clinical outcomes.
Clinical Alzheimer’s labels were not enough. Probable Alzheimer’s disease was diagnosed using clinical criteria. Without amyloid PET, tau PET, or cerebrospinal fluid confirmation across all cohorts, some cases may have mixed or non-Alzheimer’s disease pathology.
Multimodal data were limited. Plasma pTau217 and structured olfactory testing were available only in the in-house cohort. ADNI and OASIS helped validate MRI classification, but they did not externally validate the pTau217-smell-radiomics mediation pathway.
Radiomics features are hard to interpret biologically. Texture features may reflect gliosis, synaptic loss, myelin changes, tissue water shifts, or scanner/reconstruction artifacts. Post-mortem validation would be needed before a specific radiomics feature can be assigned a specific cellular meaning.
Prodromal Alzheimer’s disease remains the real test. The clinical prize is not separating established Alzheimer’s disease from healthy controls. It is predicting which people with subjective cognitive decline or mild cognitive impairment will progress, and whether the prediction changes management.
Clinical Use of Olfactory MRI Radiomics for Alzheimer’s Disease
For now, hippocampus-amygdala radiomics is a research-grade bridge between blood biomarkers and brain injury. It is not ready to replace plasma pTau217, amyloid PET, tau PET, cerebrospinal fluid testing, or clinical assessment.
A realistic future pathway would look narrower:
- Initial clinical assessment: symptoms, functional change, medication review, sleep, mood, neurological examination, and baseline cognitive testing.
- Low-friction biomarkers: plasma pTau217 and structured smell identification could enrich probability before expensive imaging.
- Brain-stage refinement: MRI radiomics could help estimate whether molecular risk has translated into hippocampus-amygdala injury.
- High-stakes confirmation: amyloid or tau confirmation would still be needed before disease-modifying treatment decisions.
The strongest takeaway is calibrated: the Chen study makes olfactory-limbic MRI radiomics worth following, especially when paired with pTau217 and smell testing. The data do not yet support routine clinical use, but they do support a sharper research question: whether a blood-test-plus-smell-test-plus-MRI-texture panel can predict Alzheimer’s disease progression earlier than blood or volume alone.
Questions About Olfactory MRI Radiomics and Alzheimer’s Disease
Why would MRI radiomics add information beyond hippocampal volume?
MRI radiomics is a computational method that extracts hundreds or thousands of numerical features from MRI scans. These features describe shape, intensity, and texture patterns that may capture disease-related tissue changes too subtle for ordinary visual reading.
Does this mean a smell test can diagnose Alzheimer’s disease?
No. Smell impairment is common in Alzheimer’s disease, but it is not specific. Viral injury, smoking, sinonasal disease, Parkinson’s disease, traumatic brain injury, medication effects, and aging can all reduce smell.
Smell testing is more plausible as a low-cost risk-enrichment tool when combined with cognition, blood biomarkers, and imaging.
Why did the hippocampus and amygdala perform better than primary smell regions?
The hippocampus and amygdala integrate smell with memory, emotion, and broader limbic circuitry. Alzheimer’s disease pathology may create a stronger cumulative MRI texture signal in these convergence hubs than in a single primary olfactory-processing region.
Is radiomics better than plasma pTau217?
No. Plasma pTau217 is closer to clinical deployment and directly tracks Alzheimer’s-type tau biology. Radiomics may eventually add brain-circuit context, but it has a heavier validation burden before clinical use.
What would prove this approach is clinically useful?
Longitudinal studies would need to show that baseline hippocampus-amygdala radiomics predicts future cognitive decline or conversion from mild cognitive impairment to Alzheimer’s disease. The model would also need biomarker-confirmed diagnoses, external validation, standardized MRI processing, and evidence that clinicians make better decisions when the radiomics result is added.
References
- Chen B, Gao P, Liu H, et al. Olfactory radiomics signatures link pTau217 to cognitive impairment in probable Alzheimer’s disease: a multi-cohort machine learning study. Alzheimer’s Research & Therapy. 2026. https://doi.org/10.1186/s13195-026-02053-0
- Palmqvist S, Warmenhoven N, Anastasi F, et al. Plasma phospho-tau217 for Alzheimer’s disease diagnosis in primary and secondary care using a fully automated platform. Nature Medicine. 2025;31:2036-2043. https://doi.org/10.1038/s41591-025-03622-w
- Gebril NM, Elettreby AM, Younis AH, et al. From cerebrospinal fluid to blood draw: plasma p-Tau217 as a non-invasive biomarker for Alzheimer’s disease: a Fagan nomogram-based meta-analytic study. Molecular Neurobiology. 2026;63:606. https://doi.org/10.1007/s12035-026-05864-2
- Jack CR Jr, Bennett DA, Blennow K, et al. NIA-AA Research Framework: Toward a biological definition of Alzheimer’s disease. Alzheimer’s & Dementia. 2018;14(4):535-562. https://doi.org/10.1016/j.jalz.2018.02.018
- de Moraes e Silva M, Mercer PBS, Witt MCZ, Pessoa RR. Olfactory dysfunction in Alzheimer’s disease: systematic review and meta-analysis. Dementia & Neuropsychologia. 2018;12(2):123-132. https://pubmed.ncbi.nlm.nih.gov/29988355/
- Wheeler PL, Murphy C. Olfactory measures as predictors of conversion to mild cognitive impairment and Alzheimer’s disease. Brain Sciences. 2021;11(11):1391. https://doi.org/10.3390/brainsci11111391
- Chen Z, Xie H, Yao L, et al. Olfactory impairment and the risk of cognitive decline and dementia in older adults: a meta-analysis. Brazilian Journal of Otorhinolaryngology. 2020;87(1):94-102. https://doi.org/10.1016/j.bjorl.2020.07.009