
A 2026 FAERS pharmacovigilance study of 28,938 dystonia reports found the strongest reporting signal for metoclopramide, while antipsychotics dominated the high-volume psychiatric medication signal and most timed cases began within 30 days of drug exposure.1
Research Highlights
- 28,938 dystonia reports: Chen et al. analyzed 27,618 patients represented in FAERS reports from Q1 2004 through Q3 2024.1
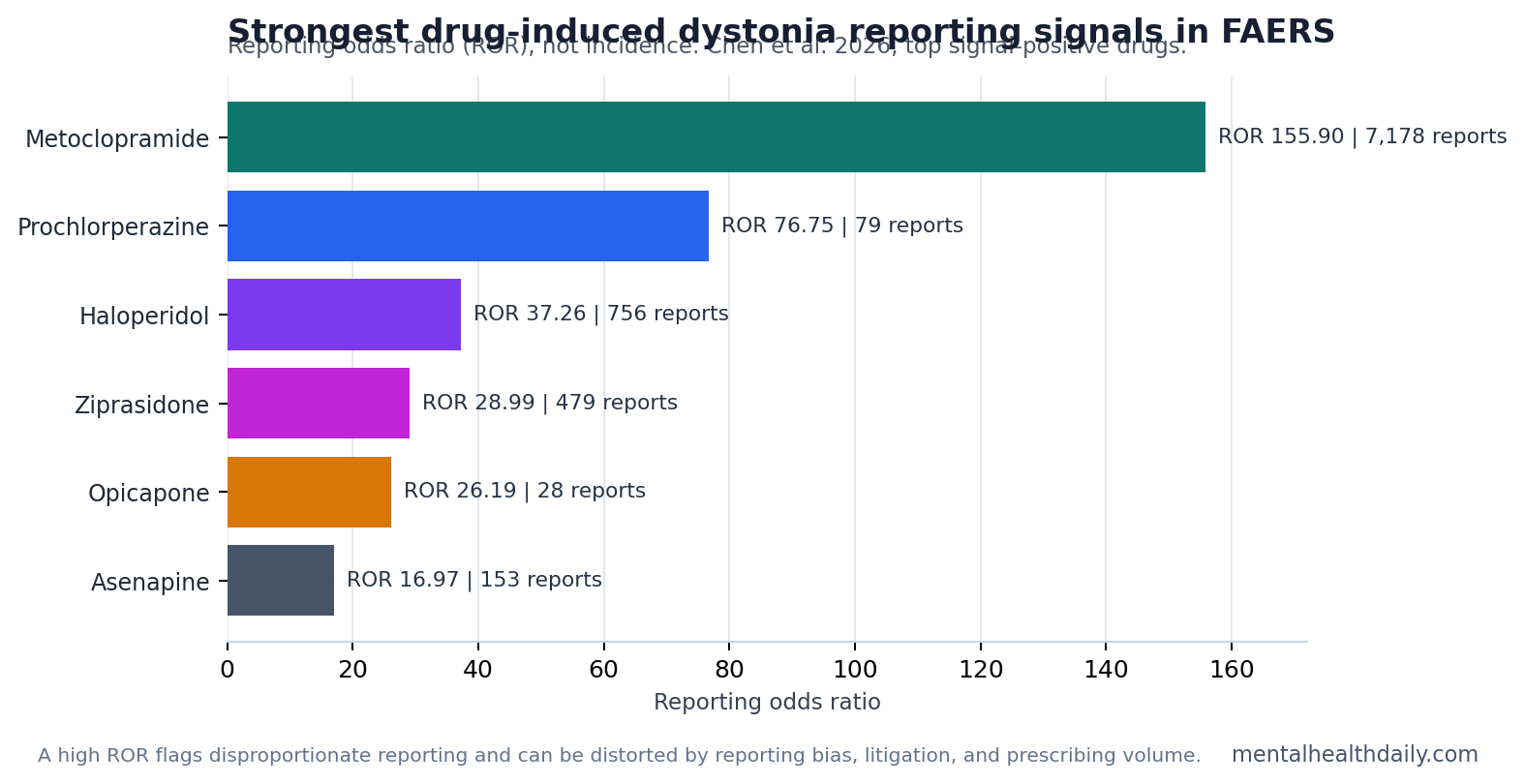
- Metoclopramide led the signal: the anti-nausea drug had 7,178 reports and a reporting odds ratio (ROR) of 155.90, with a 95% confidence interval (CI) of 151.70–160.21.1
- Antipsychotics filled the psychiatric-risk tier: aripiprazole had 1,595 reports, risperidone 1,366, quetiapine 940, olanzapine 837, and haloperidol 756.1
- Early monitoring is the practical window: among reports with usable timing, 66.34% occurred within 0–30 days and the overall median onset was 5 days.1
- Label gaps were signal-level, not proof: 8 implicated drugs lacked dystonia labeling, but several had low report counts, so the result supports targeted study rather than automatic causal certainty.1
Drug-induced dystonia means sustained or intermittent involuntary muscle contraction after medication exposure, often producing abnormal eye, jaw, neck, trunk, or limb postures. The reaction sits inside the broader family of extrapyramidal symptoms — movement problems caused by disruption of dopamine-sensitive motor circuits, especially in the basal ganglia.2,3
The Chen et al. analysis ranks reporting signals rather than per-prescription dystonia incidence. FAERS is a spontaneous adverse-event reporting system, so it detects disproportionate reporting, not incidence. The practical signal is narrower: when new sustained spasms or abnormal postures appear after a medication change, the drug review should start with dopamine-blocking antiemetics and antipsychotics, then widen to less obvious medication classes if the timing fits.
Metoclopramide Had the Strongest Dystonia Reporting Signal
Metoclopramide is a dopamine D2 receptor antagonist used for nausea, vomiting, reflux-related symptoms, and gastroparesis. The same dopamine blockade that helps gastrointestinal motility can disturb motor circuits, which is why metoclopramide has long been linked to acute dystonia, tardive dyskinesia, and other movement disorders.1,2
In the 2026 FAERS study, metoclopramide was the most frequently reported drug among the top 50 dystonia-signal agents, with 7,178 reports. It also had the strongest disproportionality signal: ROR 155.90 (95% CI 151.70–160.21), proportional reporting ratio 146.77, information component 6.79, and empirical Bayesian geometric mean 110.61.1
Interpretive limit: a high ROR means dystonia appeared disproportionately often among reports involving that drug. Clinical risk cannot be multiplied directly from this number because FAERS lacks a clean denominator for how many people used the drug without reporting dystonia.
Chen et al. also cautioned that metoclopramide report volume was affected by litigation-related reporting. Lawyer-submitted reports made up a substantial part of the database, and metoclopramide counts fell sharply after those reports were excluded. That makes metoclopramide a real safety signal, but not a clean population-risk estimate.
Antipsychotics Dominated the Psychiatric Medication Signal
Antipsychotics are drugs used for schizophrenia, bipolar disorder, agitation, tic disorders, psychosis-spectrum symptoms, and some off-label behavioral indications. Many reduce dopamine signaling, and dopamine blockade in striatal motor pathways is a classic mechanism for acute dystonia.3,5
Aripiprazole, risperidone, quetiapine, olanzapine, haloperidol, paliperidone, ziprasidone, clozapine, lurasidone, brexpiprazole, asenapine, and cariprazine all appeared among the top 50 signal-positive drugs. The volume leaders were aripiprazole at 1,595 reports, risperidone at 1,366, quetiapine at 940, olanzapine at 837, and haloperidol at 756.1
Signal strength and report volume did not rank drugs the same way:
- Haloperidol: 756 reports, but a much stronger ROR of 37.26, consistent with the older first-generation antipsychotic profile.
- Aripiprazole: 1,595 reports and ROR 14.73, showing that partial dopamine agonism does not remove dystonia risk.
- Quetiapine: 940 reports but lower ROR 6.12, a reminder that high use or reporting volume can look different from disproportionality strength.
- Ziprasidone and asenapine: fewer reports than aripiprazole or risperidone, but stronger RORs of 28.99 and 16.97.
Loonen and Ivanova described antipsychotic-induced dystonia as a basal-ganglia problem in which dopaminergic, cholinergic, and individual susceptibility factors interact.3
Mechanism read: the FAERS list is not limited to one antipsychotic generation or one receptor profile. Dose changes, rapid initiation, patient age, previous dystonic reactions, and drug combinations can matter more than a simple “old vs. new antipsychotic” split.
66.34% of Timed Reports Began Within 30 Days
Timing is where the FAERS analysis becomes most useful for recognition. Among 5,657 reports with complete and plausible timing, the median time to dystonia onset was 5 days, and 66.34% occurred within 0–30 days after exposure.1
The top-5 drug timing analysis sharpened that window. Metoclopramide and risperidone had median onset times of 2 days. Aripiprazole had a median of 5 days. Olanzapine and quetiapine were slower, at 16 and 19 days, respectively. The between-drug timing curves differed significantly, with log-rank chi-square 93.36, df = 4, and p < 0.001.1
Clinical implication: the first month after starting or increasing a higher-signal drug is the highest-yield monitoring period. Sudden neck pulling, jaw spasm, tongue protrusion, eye deviation, throat tightness, or painful sustained posturing in that window should trigger a medication-safety review rather than a vague anxiety, panic, or “behavioral” explanation.
Time-to-onset evidence is still incomplete. The timing analysis used only 5,657 reports, representing about 20.49% of the dystonia reports with adequate temporal information. Late-onset estimates also became less stable as the number at risk dropped. The early-onset pattern is clinically coherent, but the exact percentages should not be treated as a complete natural history.
Aripiprazole Plus Risperidone Was the Top Reported Combination
Chen et al. also examined 2-drug co-reporting signals. The aripiprazole-risperidone combination had 49 co-reported dystonia cases and the highest count among the top drug-pair signals. Other notable pairs included methylphenidate plus risperidone (48 reports), aripiprazole plus fluoxetine (36), quetiapine plus risperidone (31), and erythromycin plus haloperidol (29).1
Drug-drug interaction means one medication changes the exposure, metabolism, receptor effect, or adverse-event risk of another. For antipsychotics, the concern extends beyond additive dopamine effects. CYP2D6 and other liver-enzyme pathways can affect drug levels, and some selective serotonin reuptake inhibitors (SSRIs) can change antipsychotic metabolism or serotonergic-dopaminergic balance.1,6
The 2024 antipsychotic-polypharmacy meta-analysis by Hojlund et al. put that concern in a broader clinical context: antipsychotic polypharmacy is common, but tolerability and efficacy tradeoffs vary by combination and indication.6 FAERS cannot prove that aripiprazole plus risperidone caused dystonia in the co-reported cases, but it gives medication reviewers a concrete pair to check when dystonia appears in a patient taking multiple psychotropics.
8 Label-Gap Drugs Need Follow-Up, Not Overclaiming
The study found 8 signal-positive drugs for which dystonia was not listed in package labeling: lamotrigine, valproic acid, escitalopram, clonazepam, deutetrabenazine, trofinetide, amantadine, and sevoflurane.1
That list matters because dystonia is not always considered when a patient is taking an antiepileptic drug, antidepressant, antiparkinsonian agent, Rett syndrome drug, or anesthetic exposure rather than a classic dopamine blocker. Catthoor et al. similarly emphasized that non-antipsychotic-induced dystonia evidence exists but is heterogeneous and often built from case-level or narrative evidence.7
Regulatory interpretation should stay conservative. Four of the 8 label-gap drugs had only 30–39 reports each. A small FAERS signal can identify a question worth studying, but it cannot establish enough causal certainty for an immediate labeling change by itself.
Evidence-strength note: this is a retrospective pharmacovigilance study. It can rank reporting signals, expose timing patterns, and flag medication combinations. It cannot calculate incidence, prove that the drug caused the dystonia in an individual report, fully remove reporting bias, or separate drug effect from the underlying illness in every case.
Clinical use: the signal is strongest as a medication-review checklist after new spasms, abnormal postures, jaw tightness, eye deviation, or neck twisting.
Questions About Drug-Induced Dystonia Signals
Does this mean metoclopramide is the most dangerous dystonia drug?
No. Metoclopramide had the strongest FAERS reporting signal and the highest report count in this analysis, but FAERS cannot estimate true clinical incidence. The result means metoclopramide should stay near the top of the medication review when dystonia appears after nausea or gastric-motility treatment.
Why do antipsychotics cause dystonia?
Many antipsychotics reduce dopamine signaling in motor circuits. When dopamine-acetylcholine balance shifts in the basal ganglia, vulnerable patients can develop sustained muscle contractions, abnormal postures, jaw or neck spasms, eye deviation, or other extrapyramidal symptoms.3,5
When should dystonia be suspected after a medication change?
The Chen et al. timing data point to the first month as the highest-yield window, especially the first days to weeks for metoclopramide, risperidone, and aripiprazole. New sustained posturing, painful spasms, or abnormal eye, jaw, tongue, throat, or neck contractions after initiation or dose escalation should be treated as medication-linked until reviewed.
What should a patient do if dystonia symptoms appear?
Sudden dystonia-like symptoms can be urgent, especially if the throat, tongue, breathing, or swallowing is involved. Medication changes, dose reduction, discontinuation, anticholinergic rescue treatment, or switching decisions should be handled by a clinician who can review the full drug list and the severity of the reaction.
References
- Chen C, Lin X, Yang Y, Yan J, Chen J, Zheng Y, Li J. Identifying high-risk medications for drug-induced dystonia: a 20-year retrospective real-world pharmacovigilance study based on FAERS. Health Science Reports. 2026;9:e72194. https://doi.org/10.1002/hsr2.72194
- Duma SR, Fung VS. Drug-induced movement disorders. Australian Prescriber. 2019;42:56–61. https://doi.org/10.18773/austprescr.2019.014
- Loonen AJM, Ivanova SA. Neurobiological mechanisms associated with antipsychotic drug-induced dystonia. Journal of Psychopharmacology. 2021;35:3–14. https://doi.org/10.1177/0269881120944156
- Rissardo JP, Vora N, Mathew B, Kashyap V, Muhammad S, Fornari Caprara AL. Overview of movement disorders secondary to drugs. Clinics and Practice. 2023;13:959–976. https://doi.org/10.3390/clinpract13040087
- Vanegas-Arroyave N, Caroff SN, Citrome L, et al. An evidence-based update on anticholinergic use for drug-induced movement disorders. CNS Drugs. 2024;38:239–254. https://doi.org/10.1007/s40263-024-01078-z
- Hojlund M, Kohler-Forsberg O, Gregersen AT, et al. Prevalence, correlates, tolerability-related outcomes, and efficacy-related outcomes of antipsychotic polypharmacy: a systematic review and meta-analysis. Lancet Psychiatry. 2024;11:975–989. https://doi.org/10.1016/s2215-0366(24)00314-6
- Catthoor K, Detraux J, De Hert M. The epidemiology and phenomenology of non-antipsychotic-induced dystonia: a hybrid systematic-narrative review. European Psychiatry. 2025;68:e36. https://doi.org/10.1192/j.eurpsy.2025.18