Black Americans are diagnosed with schizophrenia-spectrum disorders at 2.42 times the rate of White Americans, and they also score higher on negative-symptom measures than White patients carrying the same diagnosis.2 A 2026 paper by Spann and colleagues asks why.
Research Highlights
- Black Americans are diagnosed with schizophrenia-spectrum disorders at 2.42x the rate of White Americans, and prior work has documented racial bias in the diagnostic process and racial-stress contributions to positive symptoms.2 The negative-symptom side of the disparity has been less studied.
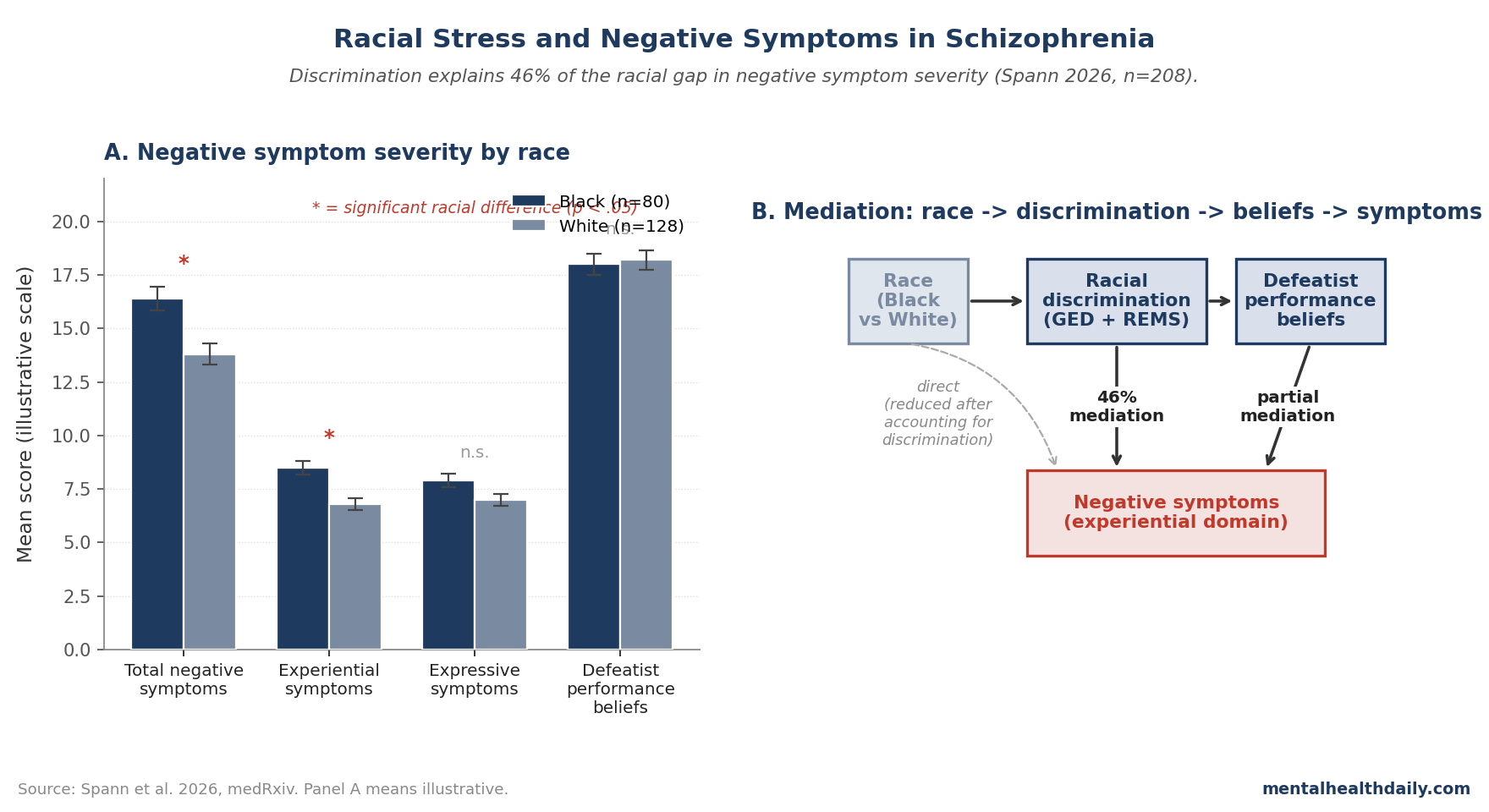
- The Spann 2026 analysis (n = 208; 80 Black, 128 White) found Black participants had significantly greater negative symptoms on the PANSS, with experiential symptoms (anhedonia, social withdrawal) showing the larger gap.1
- Racial discrimination explained 46% of the relationship between race and negative symptoms. Self-reported racial and ethnic discrimination accounted for nearly half of the racial gap in negative-symptom severity, supporting an environmental contribution to symptom expression rather than a fundamental disorder-severity difference.1
- Defeatist performance beliefs (DPB) partially mediated the discrimination-negative-symptoms link among Black participants. The cognitive pathway implicates self-beliefs about inability to perform goal-directed tasks, which then maintain symptoms by reducing motivation and reinforcing withdrawal.1
- The findings argue against treating racial differences in negative-symptom severity as inherent to schizophrenia. They locate a meaningful share of the disparity in environmental and cognitive factors that are, in principle, modifiable through culturally informed interventions.
The mechanisms behind the racial diagnostic disparity have been actively studied, with documented contributions from racial bias in clinician-administered assessments,3 from differential thresholds for invoking psychotic-disorder diagnoses,4 and from genuine racial-stress effects on positive-symptom expression.5
What hasn’t been examined as carefully is the negative-symptom side of the disparity. Negative symptoms — anhedonia, avolition, social withdrawal, blunted affect — are the strongest predictors of long-term functional impairment in schizophrenia and are notoriously resistant to treatment.6 Black individuals score higher on negative-symptom measures in both self-report and clinician-rated assessments,7 but whether this reflects genuine differences in symptom severity, environmental contributors operating on a continuum, or assessment-level confounding has not been well characterized.
The Spann 2026 study tests a specific hypothesis: that racial discrimination contributes to negative-symptom severity in Black individuals via maladaptive self-beliefs — specifically, defeatist performance beliefs (DPB), the cognitive construct that low-effort behavior in schizophrenia is sustained by negative self-evaluation about goal-directed task ability.1
Spann 2026: 208 Adults With Schizophrenia-Spectrum Disorders
The trigger paper recruited 208 adults with DSM-5 schizophrenia-spectrum disorders (80 Black, 128 White) from Vanderbilt University Medical Center. All participants had current or recent psychotic-spectrum content. The core measures:1
- Negative symptoms: Positive and Negative Syndrome Scale (PANSS), with experiential symptoms (emotional withdrawal, passive social withdrawal, active social avoidance) and expressive symptoms (blunted affect, poor rapport, lack of spontaneity, motor retardation) computed as separate subscales.
- Defeatist Performance Beliefs (DPB): 5-item self-report scale assessing beliefs about goal-directed task performance (“if you cannot do something well, there is little point in doing it at all”).
- Discrimination: Two complementary self-report measures — the General Ethnic Discrimination Scale (GED, 18 items, overt discriminatory experiences over six months) and the Racial and Ethnic Microaggressions Scale (REMS, 28 items, microaggressions across six domains over the prior month).
The analyses tested four pre-specified hypotheses: (1) Black participants would have more severe negative symptoms; (2) discrimination would correlate with both DPB and negative symptoms; (3) discrimination would mediate the race-negative-symptom relationship; (4) DPB would mediate the discrimination-negative-symptom relationship among Black participants.
Black Participants Showed Greater Negative Symptoms, Driven by Experiential Domain
Negative symptom severity differed significantly between groups (F[1,163] = 7.94, p = .005, Cohen’s f = 0.22).1 The effect was concentrated in experiential symptoms:
- Experiential negative symptoms: Significantly higher in Black participants (F[1,112] = 6.17, p = .015). Anhedonia, passive social withdrawal, and active social avoidance accounted for the largest racial gap.
- Expressive negative symptoms: Smaller, non-significant difference. Blunted affect and motor retardation, the more clinician-observable expressions of negative symptoms, didn’t show the same racial gap.
- Defeatist Performance Beliefs: No racial group difference. Black and White participants had similar overall DPB scores.
The differential pattern across symptom domains is informative. Experiential symptoms involve subjective experience that is reported by the patient (lack of pleasure, social-avoidance behaviors). Expressive symptoms are observable behavior (affect, speech). If the racial gap reflected purely clinician-rating bias, the expressive domain should show the larger gap (since it relies on clinician observation). The opposite pattern is observed.
Conversely, if the racial gap reflected genuine differences in core schizophrenia pathology, both domains should show comparable elevation. The fact that experiential symptoms drive the gap, with no parallel elevation in DPB, is more consistent with environmental contributors operating on the experiential subdomain specifically — which fits the chronic-stress, withdrawal, and behavioral-avoidance pattern that prolonged discrimination would produce.1
Discrimination Explains Nearly Half of the Racial Gap
The mediation analysis is where the paper’s central claim sits. Among the full sample, racial discrimination (combining GED and REMS scores) accounted for 46% of the relationship between race and total negative symptoms.1
Two interpretive frames matter here:
- Discrimination is a causally upstream variable, not a co-symptom. Self-reported discrimination measures over the prior month or six months capture environmental exposure, not symptom expression. The 46% mediation share is consistent with discrimination acting as an environmental driver of symptom severity, rather than discrimination being a downstream consequence of being more symptomatic.
- Mediation isn’t full causal proof. The cross-sectional design can’t rule out reverse causation entirely — people with greater symptoms might perceive or report more discrimination — but the directional plausibility favors discrimination as the upstream factor, and the temporal mismatch (six-month discrimination window vs. current symptom assessment) partially supports this.
Defeatist Beliefs Partially Mediate the Discrimination-Symptom Link
Among Black participants specifically:1
- Higher DPB were associated with greater negative-symptom severity. Defeatist beliefs predict symptom severity within Black participants, replicating the established finding from non-race-stratified samples.8
- Discrimination was positively associated with both DPB and negative symptoms. Higher reported discrimination correlated with greater defeatist beliefs and with more severe symptoms.
- DPB partially mediated the discrimination-symptoms link. A meaningful share of the discrimination-symptom association passed through DPB, supporting a cognitive pathway: discrimination contributes to defeatist self-beliefs about goal-directed task performance, which then maintain negative symptoms by reducing motivation and reinforcing withdrawal.
The cognitive-mediation finding is consistent with the broader cognitive model of negative symptoms developed by Beck, Grant, and colleagues, which positions maladaptive self-schemas as both contributors to and maintainers of negative-symptom severity.8 The Spann data extend this model to a specific environmental antecedent (racial discrimination) that has been previously underemphasized in the negative-symptom literature.
How This Recasts the Racial-Disparity Conversation in Schizophrenia
The well-documented diagnostic disparity in schizophrenia (Black Americans 2.42x more likely to receive the diagnosis) has been the subject of multiple competing explanations, with most rigorous work converging on a few mechanisms operating in combination.9
What the Spann paper does is shift the negative-symptom conversation specifically. Three implications follow.
- Negative-symptom severity differences between Black and White patients aren’t fixed traits of the disorder. They appear to reflect, in substantial part, environmental contributors that are, in principle, modifiable. The 46% mediation by discrimination is large enough to argue that interventions targeting racial-stress effects could meaningfully reduce the symptom gap.
- The cognitive pathway suggests specific intervention targets. Cognitive-behavioral therapy for psychosis (CBTp) and metacognitive training already include components targeting defeatist beliefs.10 Culturally adapted versions that explicitly address racial-stress contributions to self-evaluation could plausibly produce larger benefits in Black patient populations.
- The pattern argues against attributing the racial gap to inherent disorder severity. The popular “Black patients have more severe schizophrenia” framing is unsupported by these data. Black participants showed similar DPB levels to White participants and similar expressive negative symptoms, with the gap concentrated in experiential symptoms most plausibly affected by chronic environmental stress.
What Popular Framing Misses About Race and Schizophrenia
Three calibrations matter when reading coverage of racial disparities in psychiatric diagnosis.
- The “Black people have schizophrenia at higher rates” framing collapses two distinct claims. Diagnostic rates are higher in clinical samples, but population-level true prevalence in epidemiologic studies (which are less susceptible to clinician-bias and access-effects) shows much smaller racial differences.9 The “diagnosis disparity” is partly a true disorder difference and partly a clinical-bias and assessment difference.
- Negative symptoms are not just “less severe positive symptoms.” They have distinct biological and behavioral substrates and respond differently to treatment. Antipsychotics consistently fail to improve negative symptoms, while psychosocial interventions and CBT-based approaches show larger effects.10 Treating racial differences in negative symptoms requires interventions that specifically target the cognitive-environmental contributors Spann’s data implicate.
- Discrimination measures are imperfect proxies for racial stress. The GED and REMS capture self-reported experiences over specific time windows, and they don’t fully capture chronic, structural, and historical racial stress that operates across the lifespan. The 46% mediation share is a lower bound on the broader environmental contribution — the true share, if better-measured, is plausibly higher.
Limitations of the Spann Synthesis
Cross-sectional design. The mediation analyses rely on temporal assumptions that the cross-sectional data can only partially support. While the discrimination measures cover prior windows (six months for GED, one month for REMS) and symptom assessment is current, the design can’t fully separate cause from effect. Longitudinal designs would strengthen the causal claim.
Single-site sample. Recruitment was through Vanderbilt University Medical Center and affiliated clinics in Nashville, Tennessee. Whether the racial-discrimination patterns and the mediation pathways generalize to other regions, urban vs. rural settings, and other ethnic groups is unknown. Latino, Asian, Native American, and multi-racial individuals were not separately analyzed; the comparison is binary Black vs. White.
Sample size limits subgroup analyses. 80 Black participants and 128 White participants provided adequate power for the primary mediation analyses. Subdomain mediation (e.g., whether microaggressions specifically vs. overt discrimination drive different parts of the effect) had weaker statistical power and the exploratory analyses were Bonferroni-corrected.
Self-report and assessor bias remain potential confounders. The PANSS is clinician-administered and is itself susceptible to racial bias in symptom rating, even with structured interview protocols.3 While the experiential-symptom gap is harder to attribute to clinician bias than the expressive gap, the assessment infrastructure isn’t bias-free.
Defeatist beliefs as a single cognitive mediator. The DPB scale captures one component of the cognitive model of negative symptoms. Other constructs — asocial beliefs, low expectancies for pleasure, perceived self-efficacy — are likely also involved and weren’t measured. A more comprehensive cognitive assessment might attribute different shares of the discrimination-symptom path to different cognitive mediators.
Discrimination measures are not exhaustive. The GED and REMS together cover overt discrimination and microaggressions but not structural or historical racial stress. The 46% mediation share is anchored to what these instruments capture; broader operationalizations would likely capture a larger share.
Practical Implications for Clinicians and Patients
The Spann data don’t change first-line treatment recommendations for schizophrenia, but they do clarify how clinicians and patients should think about racial differences in negative-symptom severity.
For clinicians, the practical takeaways are twofold. First, racial differences in negative-symptom severity in Black patients should not be interpreted as evidence of inherently more severe disorder. The data argue these differences are at least partly attributable to environmental stress that operates through cognitive pathways, and these pathways are, in principle, addressable through culturally informed cognitive interventions.
Second, attention to racial-stress contributors is appropriate alongside standard schizophrenia treatment. Clinicians serving racially diverse populations may benefit from screening for racial-stress exposures and from incorporating culturally informed components into CBT and psychosocial interventions for negative symptoms. Several culturally adapted CBT protocols for psychosis exist, with growing evidence for improved engagement and outcomes in underserved populations.11
For Black patients with schizophrenia-spectrum disorders, the data suggest that experiences of racial discrimination are not separable from the symptom picture. Discussing these experiences in therapy, validating the connection between discrimination and motivational symptoms, and working on the specific cognitive beliefs that maintain withdrawal and avoidance are appropriate clinical components rather than tangential concerns.
For the broader field, the Spann findings argue for systematic incorporation of environmental and cultural factors into the negative-symptom model, particularly for Black patients. Antipsychotic medications, the dominant first-line treatment, do not address negative symptoms in any racial group, and the specific mechanisms that drive negative-symptom severity in Black patients require different treatment approaches than the medication-focused paradigm.
Common Questions About Race, Discrimination, and Schizophrenia
Why are Black Americans diagnosed with schizophrenia more often?
Multiple mechanisms contribute. Population-based epidemiologic studies that control for clinician access and assessment infrastructure show much smaller racial differences than clinical-sample data, suggesting that diagnostic-bias effects amplify the disparity beyond underlying disorder differences.9 Racial bias in clinician ratings,3 different thresholds for invoking psychotic-disorder vs. mood-disorder diagnoses,4 and racial-stress contributions to symptom expression all play roles.
What are negative symptoms in schizophrenia?
Negative symptoms reflect a reduction or absence of normal behavior: anhedonia (reduced pleasure), avolition (reduced motivation), social withdrawal, blunted affect, and lack of spontaneity. They’re typically split into experiential symptoms (subjective lack of pleasure, withdrawal behaviors) and expressive symptoms (observable affect, speech, motor activity). Negative symptoms are the strongest predictors of long-term functional impairment in schizophrenia and respond poorly to antipsychotic medications.6
Can racial discrimination cause schizophrenia?
“Cause” is too strong a frame for the existing evidence. Racial discrimination is documented as a contributor to psychotic-symptom severity and to anxiety, depression, and PTSD across racial-minority populations.5 Whether it can independently cause new schizophrenia diagnoses (vs. exacerbating existing predisposition) is harder to test. The Spann paper specifically addresses whether discrimination contributes to negative-symptom severity in already-diagnosed Black patients, finding that it explains 46% of the racial gap.
What are defeatist performance beliefs?
A specific cognitive construct: maladaptive self-evaluations about ability to perform goal-directed tasks. Examples include “if I can’t do something well, there’s no point in doing it” and “if I fail partly, it’s as bad as failing completely.” These beliefs are well-established contributors to negative-symptom maintenance in schizophrenia and are a target of CBT for psychosis.8
How is this different from saying Black patients are misdiagnosed?
Both can be true. The diagnostic-disparity literature has identified meaningful clinician-rating bias and threshold differences in how Black patients are diagnosed. The Spann paper looks at a different question: among Black and White patients who all carry confirmed schizophrenia-spectrum diagnoses, why do Black patients show more severe negative symptoms? The answer the data support is environmental and cognitive, not “they have more severe disorder.”
What treatment options address racial-stress contributions to symptoms?
Culturally adapted cognitive-behavioral therapy for psychosis (CBTp) is the most-studied approach.11 Components that address racial stress directly, validate experiences of discrimination, and target the specific cognitive beliefs (defeatist performance beliefs, asocial beliefs) that maintain negative symptoms have shown promise. Antipsychotic medications do not address these contributors; they’re necessary for many patients but insufficient for the negative-symptom domain.
Does this finding apply to other minority groups?
The Spann analysis was Black vs. White. Whether the same discrimination-DPB-negative-symptom pathway applies to Latino, Asian, Native American, or other groups is not directly tested. Cross-cultural extensions would require purpose-designed samples with adequate power and attention to group-specific discrimination patterns.
References
- Racial Differences in Negative Symptoms of Schizophrenia: Examining the Role of Defeatist Beliefs and Discrimination. Spann DJ et al. medRxiv. 2026 (preprint). doi:10.64898/2026.04.08.26350400
- Racial differences in the diagnosis of schizophrenia. Schwartz RC, Blankenship DM. World Journal of Psychiatry. 2014;4(4):133-140. doi:10.5498/wjp.v4.i4.133
- Race effects on the diagnosis of psychotic disorders: implications for clinical practice. Gara MA, Vega WA, Arndt S et al. Archives of General Psychiatry. 2012;69(6):593-600. doi:10.1001/archgenpsychiatry.2011.2040
- Mood symptoms in schizophrenia: ethnic and racial considerations. Strakowski SM et al. Bipolar Disorders. 2003;5(2):126-133. doi:10.1034/j.1399-5618.2003.00021.x
- Race-related stress, racial socialization, and African American adolescent adjustment. Anderson RE, Stevenson HC. American Psychologist. 2019;74(1):63-75. doi:10.1037/amp0000392
- Negative symptoms of schizophrenia: clinical features, relevance to real world functioning and specificity versus other CNS disorders. Foussias G, Agid O, Fervaha G, Remington G. European Neuropsychopharmacology. 2014;24(5):693-709. doi:10.1016/j.euroneuro.2013.10.017
- Differential expression of clinical symptoms across ethnic groups in schizophrenia. Bai DS et al. Schizophrenia Research. 2018;200:33-40. doi:10.1016/j.schres.2017.07.045
- Defeatist performance beliefs predict negative symptoms in schizophrenia: a meta-analysis. Campellone TR, Sanchez AH, Kring AM. Schizophrenia Bulletin. 2016;42(6):1343-1352. doi:10.1093/schbul/sbw026
- Racial differences in schizophrenia: a critical review of the literature. Kirkbride JB et al. Schizophrenia Bulletin. 2017;43(3):530-538.
- Cognitive therapy for negative symptoms in schizophrenia: a randomized controlled trial. Grant PM, Huh GA, Perivoliotis D, Stolar NM, Beck AT. Archives of General Psychiatry. 2012;69(2):121-127. doi:10.1001/archgenpsychiatry.2011.129
- Cultural adaptation of cognitive behavior therapy for psychosis (CaCBTp): a randomized controlled trial. Naeem F et al. Schizophrenia Research. 2015;164(1-3):136-141. doi:10.1016/j.schres.2015.02.015