Psychiatric brain biomarkers have produced a large research literature but little routine clinical use. A 2026 evidence map found 441 primary studies and 27 systematic reviews of neuroimaging or neurophysiologic biomarkers for mental-health disorders, yet the field still looks too small, cross-sectional, and depression-heavy for ordinary diagnostic or treatment decisions.1
Research Highlights
- Large map, weak translation: Sowerby et al. identified 441 primary studies and 27 systematic reviews, but concluded that clinical implementation of psychiatric MRI and EEG tests remains premature.1
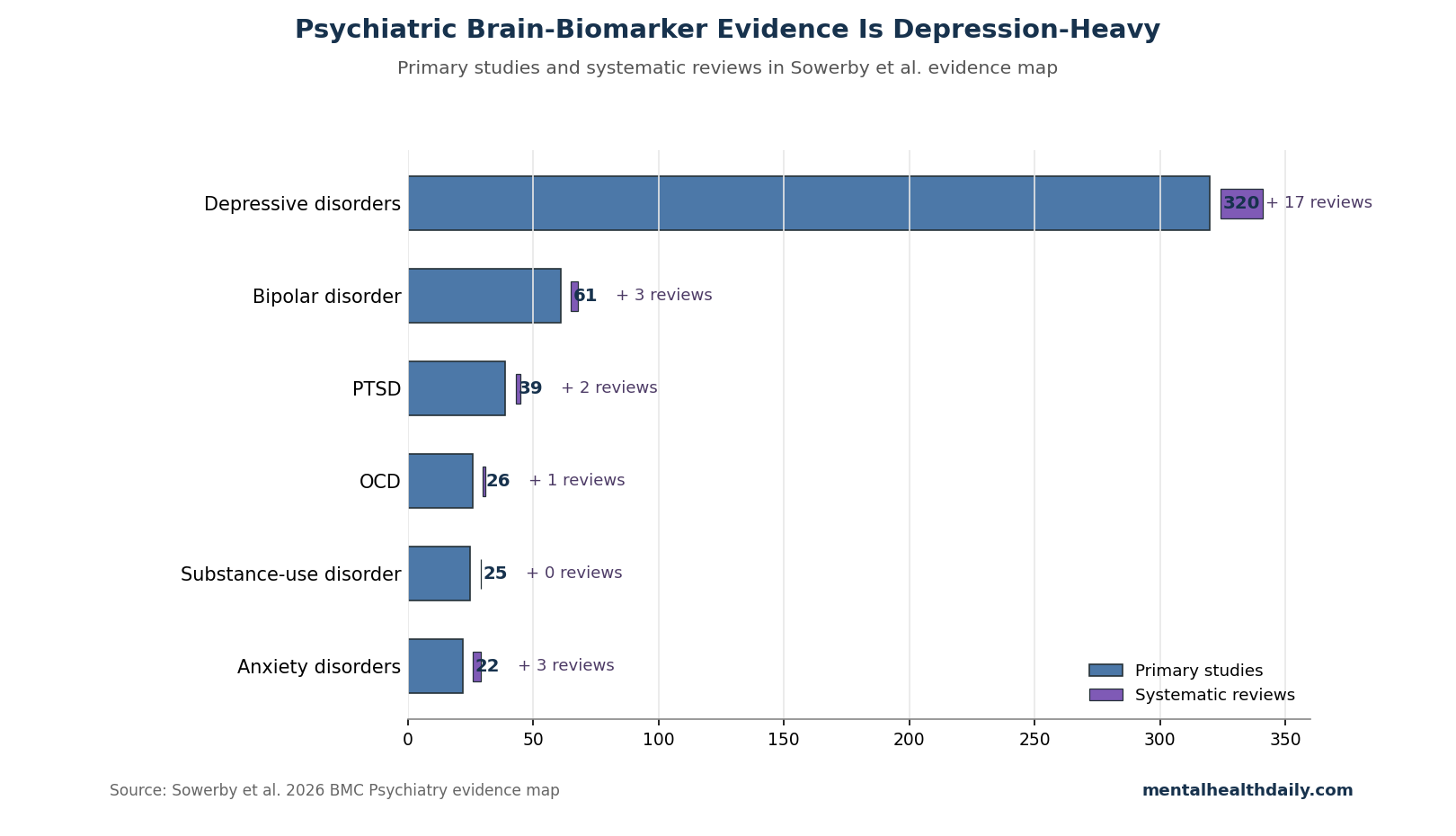
- Depression dominated the evidence: Depressive disorders accounted for 320 primary studies and 17 systematic reviews, compared with 61 bipolar, 39 PTSD, 26 OCD, 25 substance-use, and 22 anxiety-disorder primary studies.1
- Small samples stayed common: Across disorders, 263 primary studies had fewer than 100 participants, a major problem when brain-wide association work suggests stable brain-phenotype links often need thousands of people.1,3
- MRI and EEG were the main tools: About 3/4 of primary studies used MRI-based methods and 20% used EEG, with far less evidence for PET, SPECT, MEG, ASL, DTI, or paired-pulse TMS.1
- Older adults were barely represented: Only 5 studies focused on samples with a mean age of 65 or older, despite age-related brain change being central to biomarker interpretation.1
The calibrated read is not that brain biomarkers are useless. It is that psychiatric MRI, functional MRI, and electroencephalogram signals are still mostly research tools until studies become larger, longitudinal, externally validated, and tied to decisions that change patient outcomes.
441 Studies Did Not Add Up to Clinical Utility
Biomarkers are measurable biological signals used to detect disease, estimate prognosis, or guide treatment. In psychiatry, proposed brain biomarkers often come from magnetic resonance imaging (MRI; scans of brain structure or function), functional MRI (fMRI; MRI signals used to infer regional brain activity), or electroencephalogram (EEG; scalp-recorded electrical activity from the brain).
Sowerby et al. searched MEDLINE and Embase from January 2010 through September 2023 and screened 58,824 unique records. The final evidence map included 441 primary studies and 27 systematic reviews across depressive disorders, bipolar disorder, anxiety disorders, obsessive-compulsive disorder (OCD), posttraumatic stress disorder (PTSD), and substance-use disorder.1
Evidence map: this design catalogs what evidence exists, where it clusters, and where gaps remain. It does not pool accuracy estimates, grade every study’s bias, or tell a clinician which scan should be ordered on Monday morning.
That distinction drives the whole result. A large count of studies can still fail the clinical-utility test if most studies ask whether patient groups differ on a scan, rather than whether a test improves diagnosis, prognosis, treatment choice, safety monitoring, or functional outcomes.
Depression Had 320 Studies; Anxiety Had 22
Depressive disorders dominated the map: 320 primary studies and 17 systematic reviews. Other conditions were much thinner: 61 primary studies for bipolar disorder, 39 for PTSD, 26 for OCD, 25 for substance-use disorder, and 22 for anxiety disorders.1
That imbalance matters because psychiatric biomarker claims often travel faster than the disorder-specific evidence. A brain signature that helps separate depressed adults from healthy controls does not automatically diagnose PTSD, predict relapse in alcohol-use disorder, or distinguish bipolar depression from unipolar depression.
- Depression: 201 studies evaluated diagnosis, and 119 evaluated treatment response.
- Bipolar disorder: 53 studies evaluated diagnosis, often against unipolar depression or healthy controls.
- PTSD: 31 studies evaluated diagnosis, but only 7 evaluated treatment response.
- Substance-use disorder: 14 studies evaluated diagnosis, 9 evaluated prognosis, and 2 evaluated treatment response.
- Anxiety disorders: 16 studies evaluated diagnosis and 7 evaluated treatment response.
Precision psychiatry sounds like one field, but the evidence map shows several uneven literatures. Depression MRI is not the same evidence base as OCD fMRI, PTSD EEG, or relapse prediction in opioid-use disorder.
Most Psychiatric Biomarker Studies Were Small and Cross-Sectional
Sample size is the hardest practical barrier. Across disorders, 263 primary studies had fewer than 100 participants. In depression alone, 187 of 320 primary studies had total sample sizes below 100, and only 9 exceeded 1,000 participants.1
Small samples create a clinical reliability problem. Brain measures are noisy, psychiatric diagnoses are heterogeneous, medication history varies, and scanner protocols differ. A 40-person fMRI classifier can look impressive inside one lab and then collapse when tested in another population.
Marek et al. made the scale problem sharper in a 2022 Nature analysis of brain-wide association studies: reproducible links between brain measures and complex phenotypes often require thousands of individuals, not dozens.3 That does not invalidate every small psychiatric imaging study, but it changes what small studies can reasonably claim.
Evidence-strength note: Sowerby et al. mapped evidence volume and study characteristics. Because the review did not formally rate every primary study’s bias or pool performance metrics, its strongest conclusion is about readiness and distribution, not the exact diagnostic accuracy of any one MRI or EEG marker.
Cross-Sectional Diagnosis Is Not the Same as Prognosis
Cross-sectional studies measure people at one point in time. They can ask whether a brain feature differs between diagnosed patients and controls. They cannot prove that the feature appears before illness, predicts relapse, identifies treatment response, or changes a clinical decision.
Diagnosis dominated the evidence map. In depression, 201 studies evaluated diagnosis, and most diagnostic MRI or EEG studies were cross-sectional. In PTSD, nearly all diagnostic studies were cross-sectional, with only 2 cohort studies. Substance-use disorder had a similar pattern: all 9 diagnostic-accuracy studies were cross-sectional.1
Clinical biomarker use usually needs stronger designs:
- Diagnostic use: a test should improve classification beyond structured interviews, symptom scales, history, and ordinary clinical assessment.
- Prognostic use: a test should predict future relapse, remission, suicide risk, functional decline, or treatment need before that outcome is obvious.
- Treatment-selection use: a test should identify which patient is more likely to benefit from medication, psychotherapy, ECT, rTMS, or another intervention.
- Safety use: a test should improve detection of adverse-event risk, but Sowerby et al. found no existing study evaluating prediction of adverse events.1
Without that step from group difference to patient-level decision, biomarker language can overstate what the study actually gives a clinician.
EEG Depression Markers Show the Same Translation Problem
EEG is cheaper and more scalable than MRI, so it is a natural candidate for psychiatric biomarker work. But depression EEG reviews have repeatedly shown how hard it is to move from promising signal to clinical test.
Van der Vinne et al. reviewed frontal alpha asymmetry as a depression diagnostic marker and questioned whether the signal was fact or fiction as a practical diagnostic tool.4 Widge et al. found EEG treatment-response prediction in major depressive illness promising enough to study, but not ready to guide routine antidepressant decisions.5
Sowerby et al. found 100 depression EEG primary studies and 55 depression EEG diagnostic studies. Nearly all diagnostic EEG studies were cross-sectional, and only 9 had at least 100 participants.1
Practical implication: EEG may be the more deployable technology, but deployability does not solve validation. A cheap test that has not been externally validated still risks false reassurance, false labeling, and wasted treatment detours.
Large Cohorts Are the Exit Route From One-Lab Biomarkers
The map points toward a practical exit route: large, shared, longitudinal datasets with standardized clinical measures. Sowerby et al. named the Adolescent Brain Cognitive Development study, UK Biobank, and Human Connectome Project as examples of large-scale data infrastructure that can support more reproducible mental-health biomarker work.1
Williams argued earlier that depression and anxiety might be reorganized around neural-circuit dysfunction instead of only symptom labels.2 That is a plausible research direction. It becomes clinically useful only if circuit measures identify real patient subgroups, predict outcomes, and outperform simpler information such as symptom course, comorbidity, trauma exposure, medication history, sleep, cognition, and functioning.
For psychiatric MRI and EEG, the bar should be concrete:
- External validation: does the model work in hospitals, scanners, languages, and populations outside the training dataset?
- Incremental value: does the biomarker add useful information beyond a careful interview and validated symptom scales?
- Decision impact: does the test change treatment, monitoring, or referral in a way that improves outcomes?
- Equity check: does performance hold across age, sex, race, ethnicity, disability, trauma burden, and medication exposure?
Until those conditions are met, psychiatric brain biomarkers are better described as research signals than clinical tests.
Questions About Psychiatric Brain Biomarkers
Can MRI diagnose depression, PTSD, OCD, or bipolar disorder right now?
Not as a routine clinical test. MRI can reveal research-level group differences and may help exclude neurological disease when clinically indicated, but Sowerby et al. concluded that psychiatric MRI and EEG tests are not ready for ordinary diagnosis or treatment management.1
Does this mean psychiatric disorders are not biological?
No. It means the currently mapped biomarkers are not yet stable enough for individual clinical decisions. Psychiatric disorders can involve real brain, immune, endocrine, developmental, and environmental mechanisms without any single scan being ready as a diagnostic shortcut.
Why are small studies such a problem in brain biomarker research?
Brain measurements are high-dimensional: a study can examine thousands of voxels, regions, connections, frequencies, or model features. With small samples, a model may learn quirks of the training group instead of a repeatable illness signal.
Which psychiatric biomarker use is most plausible first?
Treatment-response prediction is more plausible than broad diagnosis because the decision is narrower: among people who already have a diagnosis, can a test predict response to a specific intervention? Even there, EEG, MRI, and fMRI markers still need larger external validation before routine use.
What should patients do if a clinic sells brain scans for psychiatric diagnosis?
Ask what diagnosis, treatment choice, or outcome the scan has been validated to improve, and in what population. A useful answer should include published external validation, not colorful images, case examples, or claims that the scan shows a chemical imbalance.
Bottom line: psychiatric neuroimaging and EEG biomarkers are scientifically active but clinically immature. The 2026 evidence map found hundreds of studies, yet the dominant pattern was small, cross-sectional, depression-focused work rather than validated tests that improve real diagnostic or treatment decisions.
References
- Sowerby C, Landsteiner A, Ullman K, Anthony M, Kalinowski C, Spoont MR, et al. Neuroimaging and neurophysiologic biomarkers for diagnosis and prognosis of depressive disorders, bipolar disorder, anxiety disorders, obsessive compulsive disorder, posttraumatic stress disorder, and substance use disorder: an evidence map. BMC Psychiatry. 2026;26:375. https://doi.org/10.1186/s12888-025-07429-4
- Williams LM. Precision psychiatry: a neural circuit taxonomy for depression and anxiety. Lancet Psychiatry. 2016;3(5):472-480. doi:10.1016/s2215-0366(15)00579-9
- Marek S, Tervo-Clemmens B, Calabro FJ, Montez DF, Kay BP, Hatoum AS, et al. Reproducible brain-wide association studies require thousands of individuals. Nature. 2022;603(7902):654-660. https://doi.org/10.1038/s41586-022-04492-9
- van der Vinne N, Vollebregt MA, van Putten MJAM, Arns M. Frontal alpha asymmetry as a diagnostic marker in depression: fact or fiction? A meta-analysis. NeuroImage: Clinical. 2017;16:79-87. https://doi.org/10.1016/j.nicl.2017.07.006
- Widge AS, Bilge MT, Montana R, Chang W, Rodriguez CI, Deckersbach T, et al. Electroencephalographic biomarkers for treatment response prediction in major depressive illness: a meta-analysis. American Journal of Psychiatry. 2019;176(1):44-56. https://doi.org/10.1176/appi.ajp.2018.17121358
- Santos VA, Carvalho DD, Van Ameringen M, Nardi AE, Freire RC. Neuroimaging findings as predictors of treatment outcome of psychotherapy in anxiety disorders. Progress in Neuro-Psychopharmacology & Biological Psychiatry. 2019;91:60-71. https://doi.org/10.1016/j.pnpbp.2018.09.001
- Colvonen PJ, Glassman LH, Crocker LD, Buttner MM, Orff H, Schiehser DM, et al. Pretreatment biomarkers predicting PTSD psychotherapy outcomes: a systematic review. Neuroscience & Biobehavioral Reviews. 2017;75:140-156. https://doi.org/10.1016/j.neubiorev.2017.02.003