
A 68-person randomized trial in Indian healthcare workers found a narrow but useful pattern: combined yoga plus Bhagavad Gita teaching beat usual care immediately on GAD-7 anxiety scores (p = 0.009), while Gita teaching alone beat usual care at 45 days (p = 0.047).1 Yoga alone improved within its own arm, but it did not separate clearly from control in the corrected between-group comparisons.
Research Highlights
- Immediate signal favored the combined arm: Yoga+Gita beat control immediately after the 1-week intervention (p = 0.009), with baseline GAD-7 scores balanced across all 4 groups (p = 0.908).1
- Durability favored Gita alone: at 45 days, Gita beat control in the corrected pairwise test (p = 0.047), while Yoga+Gita missed that threshold (p = 0.057).1
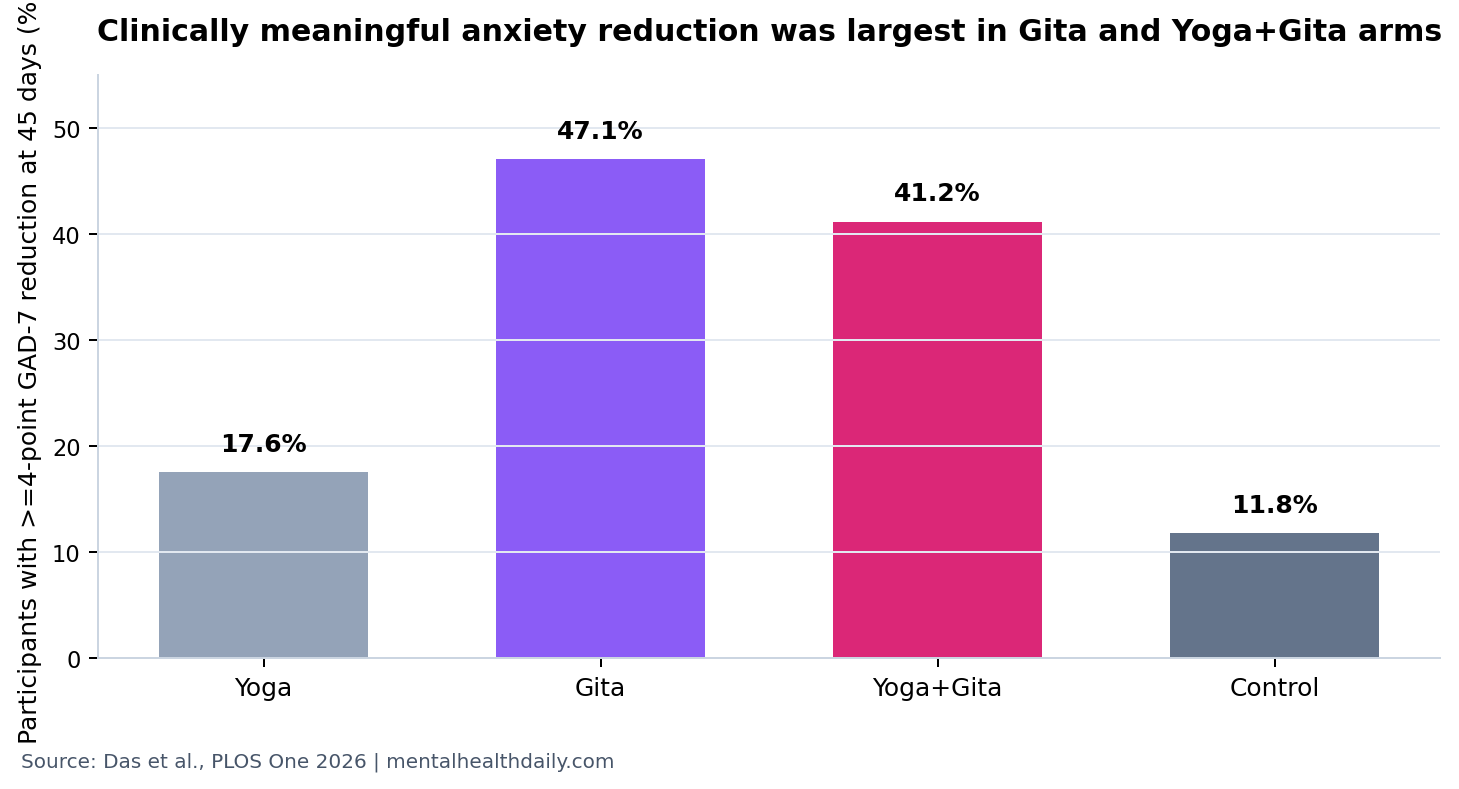
- Responder rates were uneven: a clinically meaningful ≥4-point GAD-7 drop occurred in 47.1% with Gita, 41.2% with Yoga+Gita, 17.6% with yoga, and 11.8% with control.1
- Yoga alone was weaker than the Gita-containing arms: yoga improved from baseline within arm (p = 0.007 at 45 days), but the yoga-vs-control pairwise comparison was not significant at 45 days (p = 0.944).1
- Evidence remains small and culturally bounded: the trial had 17 people per arm, an unblinded intervention, a usual-care control, and exploratory subgroup findings that were not adjusted for multiple testing.1
GAD-7 is a 7-item anxiety questionnaire that asks about symptoms such as nervousness, uncontrollable worry, restlessness, irritability, and fear that something awful might happen. A ≥4-point reduction is often treated as a minimum clinically important difference, meaning a change large enough to be noticed as more than measurement noise.2
The trial compared 3 low-stigma, culturally familiar interventions against usual care, then separated immediate from delayed anxiety effects.
Yoga+Gita Beat Control Immediately; Gita Led at 45 Days
Das et al. randomized 68 healthcare workers at a secondary hospital in India to 4 arms: 60 minutes of yoga daily for 1 week, 60 minutes of Bhagavad Gita teaching daily for 1 week, 30 minutes of yoga plus 30 minutes of Gita teaching daily for 1 week, or usual care.1
Each arm had 17 participants, and no one was lost to follow-up. GAD-7 scores were measured at baseline, immediately after the intervention, and 45 days later. Baseline anxiety did not differ across groups (p = 0.908), which makes the post-intervention comparisons easier to read.
The immediate post-intervention Kruskal-Wallis test differed across groups (p = 0.011), and the corrected pairwise test identified Yoga+Gita vs. control as the significant split (p = 0.009). At 45 days, the group test also differed (p = 0.025), but the corrected pairwise signal belonged to Gita vs. control (p = 0.047).1
That pattern argues against the lazy headline that “yoga worked.” The more precise read is that the combined intervention gave the clearest immediate anxiety separation, and scripture-based teaching gave the clearest delayed separation in this specific setting.
47.1% of the Gita Arm Had a Clinically Meaningful 45-Day Drop
The responder analysis makes the practical signal easier to see. At 45 days, a ≥4-point GAD-7 reduction occurred in 8 of 17 people in the Gita arm (47.1%), 7 of 17 in the Yoga+Gita arm (41.2%), 3 of 17 in the yoga arm (17.6%), and 2 of 17 in control (11.8%).1
Exact odds ratios reflected the same gradient, but with wide confidence intervals because the cells were small:
- Gita vs. control: OR 6.67, 95% CI 1.15-38.60.
- Yoga+Gita vs. control: OR 5.25, 95% CI 0.90-30.62.
- Yoga vs. control: OR 1.61, 95% CI 0.23-11.09.
Point estimates favor Gita and Yoga+Gita, not yoga alone. The confidence intervals also say the study was too small to estimate the true effect precisely. Both facts matter: the directional pattern is not random-looking, but it is not a definitive clinical guideline.
Healthcare Workers Need Low-Friction Supports, Not Wellness Theater
Healthcare-worker mental health during COVID-19 was not a vague morale problem. A systematic review by Vizheh et al. described substantial anxiety, depression, insomnia, and distress among healthcare workers during the pandemic.3 Weibelzahl et al. similarly reported depression and anxiety concerns among healthcare professionals in pandemic conditions.4
Help-seeking is a separate barrier. Galbraith et al. found that student nurses’ attitudes toward seeking stress support were mixed, with stigma and perceived professional consequences shaping behavior.5 For working clinicians, the same friction can make formal mental-health referral feel heavier than a familiar group practice.
Culturally embedded intervention means the support fits the language, values, and routines of the population receiving it. In this trial, Bhagavad Gita teaching was not a generic spiritual add-on. It was a familiar text in a mostly Hindu Indian healthcare-worker sample, used as a structured cognitive-emotional practice.
That framing is important because uptake is part of the treatment. A technically stronger intervention that people avoid can lose to a modest intervention that people will actually attend.
Spiritual Content Is Plausible, but Context-Dependent
Religious and spiritual interventions have randomized-trial evidence, but the literature is heterogeneous. Goncalves et al. reviewed randomized clinical trials of religious and spiritual interventions in mental-health care and found signals of benefit across varied designs, populations, and outcomes.6
For the Das trial, the plausible active ingredients are not mystical. Gita teaching may have offered cognitive reframing, acceptance, duty-based meaning, social connection, instructor attention, and a language for fear under pressure. Those mechanisms overlap with secular stress-management concepts even when the cultural packaging differs.
Generalizability limit: a Gita-based intervention in an Indian healthcare-worker sample cannot be assumed to work the same way in non-Hindu, non-Indian, or religiously mixed workplaces. A secular acceptance-based program, another spiritual text, or a mindfulness protocol may be the closer equivalent elsewhere.
Yoga Evidence Supports Stress Relief, but This Trial Did Not Make Yoga the Star
Yoga has adjacent evidence for anxiety, depression, and stress. Sharma et al. tested yoga in COVID-19-positive patients and reported improvements in stress, anxiety, and depression in a quasi-randomized design.7 Chiappetta et al. reviewed mindfulness-based stress-management interventions among healthcare workers and found supportive but methodologically mixed evidence.8
Those adjacent findings make the yoga arm credible. Still, this specific 2026 trial does not support yoga as the strongest standalone option. Yoga participants improved from baseline, but the corrected between-group comparisons did not show that yoga clearly beat usual care at either post-intervention timepoint.1
Calibrated read: yoga may help some healthcare workers, especially if they practice consistently, but this trial’s strongest comparative signals came from Gita-containing arms.
The Control Arm Leaves an Attention Problem
The control condition was usual care, not an attention-matched program. That matters because the intervention arms received daily 60-minute sessions for 1 week. Instructor attention, group structure, scheduling, expectancy, and social support could all reduce anxiety independent of yoga postures or Gita content.
Evidence-strength note: this was a randomized trial, but participants were not blinded to their assigned intervention. Data analysts were blinded, which reduces analysis bias, but participant expectancy remains a live alternative explanation.
The small sample also limits subgroup interpretation. Researchers reported larger exploratory benefits among women and among participants who continued practice, but those analyses were not adjusted for multiple comparisons.1 Treat them as clues for a larger trial, not as proof that one subgroup should be targeted clinically.
Workplace Stress Programs Should Match the Workforce
The practical result is not “prescribe scripture” or “replace therapy with yoga.” It is that low-stigma workplace supports may work better when they are familiar, structured, and acceptable to the people being asked to use them.
For Indian healthcare settings where Bhagavad Gita teaching is culturally congruent, the 45-day signal is worth testing in a larger, attention-controlled trial. For other settings, the transferable principle is not the exact text; it is the combination of meaning-making, cognitive reframing, practice continuity, and group support.
Future trials should compare culturally adapted spiritual teaching, secular cognitive stress-management, yoga, and attention-matched group contact. They should also measure adherence more precisely than a yes/no continued-practice question.
The study is strongest when read as a calibration exercise. Yoga and Gita are not interchangeable wellness labels. In this trial, Gita-containing arms carried the clearest comparative signal, while yoga alone looked weaker after correction.
Questions About Yoga, Gita, and Healthcare-Worker Anxiety
Did the combined Yoga+Gita arm work best?
It had the clearest immediate effect vs. control (p = 0.009), but Gita alone had the clearest 45-day effect (p = 0.047). The trial does not prove that combining them is always better.
Was yoga alone effective?
Yoga improved within its own group, but it did not clearly beat control in the corrected pairwise comparisons. That makes the standalone yoga claim weaker than the Gita-containing-arm claim.
Can this be generalized outside India?
Only carefully. The intervention used a culturally familiar text in a specific healthcare-worker sample. Other settings would need an equivalent culturally acceptable intervention, not automatic copy-paste.
Could this replace mental-health treatment for clinicians?
No. It is a short workplace support signal for anxiety symptoms, not a replacement for diagnosis, therapy, medication, crisis care, or occupational-system fixes.
References
- Das N, Konduru L, Dahia SS, et al. The stress reduction potential of Bhagavad Gita and Yoga for healthcare workers during the COVID-19 pandemic: A randomized controlled trial. PLOS One. 2026;21(4):e0347320. doi:10.1371/journal.pone.0347320
- Toussaint A, Husing P, Gumz A, et al. Sensitivity to change and minimal clinically important difference of the 7-item Generalized Anxiety Disorder Questionnaire (GAD-7). Journal of Affective Disorders. 2020;265:395-401. doi:10.1016/j.jad.2020.01.032
- Vizheh M, Qorbani M, Arzaghi SM, et al. The mental health of healthcare workers in the COVID-19 pandemic: A systematic review. Journal of Diabetes and Metabolic Disorders. 2020;19(2):1967-1978. doi:10.1007/s40200-020-00643-9
- Weibelzahl S, Reiter J, Duden G. Depression and anxiety in healthcare professionals during the COVID-19 pandemic. Epidemiology and Infection. 2021;149:e46. doi:10.1017/S0950268821000303
- Galbraith ND, Brown KE, Clifton E. A survey of student nurses’ attitudes toward help seeking for stress. Nursing Forum. 2014;49(3):171-181. doi:10.1111/nuf.12066
- Goncalves JPB, Lucchetti G, Menezes PR, Vallada H. Religious and spiritual interventions in mental health care: a systematic review and meta-analysis of randomized controlled clinical trials. Psychological Medicine. 2015;45(14):2937-2949. doi:10.1017/S0033291715001166
- Sharma N, Sahni PS, Sharma US, Kumar J, Garg R. Effect of Yoga on the Stress, Anxiety, and Depression of COVID-19-Positive Patients: A Quasi-Randomized Controlled Study. International Journal of Yoga Therapy. 2022;32:Article 8. doi:10.17761/2022-D-22-00013
- Chiappetta M, D’Egidio V, Sestili C, Cocchiara RA, La Torre G. Stress management interventions among healthcare workers using mindfulness: a systematic review. Senses and Sciences. 2018;5:517-549. Senses and Sciences