
A 2026 nationwide Korean analysis found that resistance exercise was associated with lower depression and anxiety scores after propensity score matching, while aerobic exercise alone was not significantly associated with either outcome. The result favors adding weights, bands, machines, or body-weight strength work to mental-health exercise advice without assuming that lifting caused the lower symptom scores.1
Research Highlights
- Large Korean survey sample: Yun et al. analyzed 21,298 adults for depression and 8,707 adults for anxiety using KNHANES survey years with PHQ-9 and GAD-7 data.1
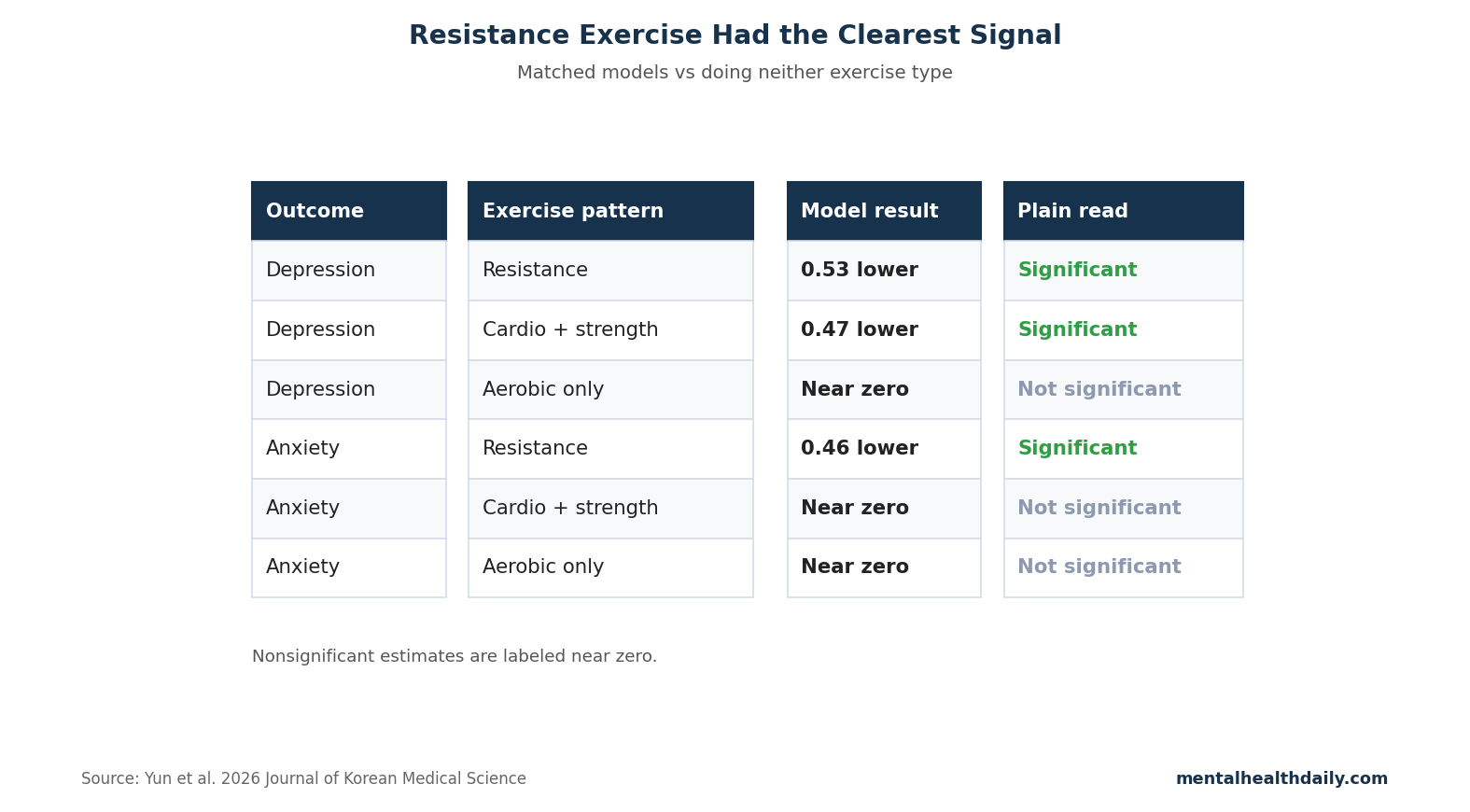
- Resistance exercise had the strongest association: Compared with adults doing neither aerobic nor resistance exercise, the resistance group had lower PHQ-9 scores (β = −0.534, 95% CI −0.765 to −0.303) and lower GAD-7 scores (β = −0.459, 95% CI −0.808 to −0.110).1
- Total exercise helped depression: Combined aerobic plus resistance exercise was associated with lower PHQ-9 scores (β = −0.473, 95% CI −0.706 to −0.241), but the coefficient was smaller than resistance exercise alone.1
- Aerobic-only exercise was not significant: Aerobic exercise alone did not show a significant association with depression or anxiety in the matched models.1
- Causality remains unsettled: The study was cross-sectional, so it cannot prove that resistance training caused lower symptom scores; people who begin with lower depression scores may also be more likely to lift regularly.1
Resistance exercise means muscle-loading exercise: weights, machines, bands, calisthenics, or other activity where muscles work against external resistance. For depression and anxiety, it may help through improved sleep, inflammatory signaling, self-efficacy, insulin sensitivity, muscle-derived signaling molecules, and the simple fact that strength gains are visible and trackable.
21,298 Adults for Depression and 8,707 for Anxiety
The study used the Korean National Health and Nutrition Examination Survey, a population survey of noninstitutionalized Korean residents. Depression was measured with the PHQ-9 across survey years 2014, 2016, 2018, 2020, and 2022. Anxiety was measured with the GAD-7 in 2021 and 2022.1
- PHQ-9: a 9-item depression questionnaire covering low mood, anhedonia, sleep, appetite, energy, guilt, concentration, psychomotor change, and suicidal thoughts.
- GAD-7: a 7-item anxiety questionnaire covering worry, nervousness, restlessness, irritability, and fear something awful might happen.
- Matching method: propensity-score-based exact matching created balanced groups by age and sex before regression adjustment.
The comparison groups were total exercise, aerobic exercise only, resistance exercise only, and neither aerobic nor resistance exercise.
Resistance Exercise Beat No Exercise on Both PHQ-9 and GAD-7
Matched result: after matching, resistance exercise had the lowest depression and anxiety scores compared with the non-aerobic/non-resistance reference group. The PHQ-9 coefficient was −0.534, and the GAD-7 coefficient was −0.459.1
These are not huge symptom shifts for an individual patient, but they matter at population scale. A half-point average movement across thousands of people can reflect a meaningful shift in the mild-symptom range, especially if the intervention also improves metabolic health, pain tolerance, and function.
Directional guidance: if someone already walks or cycles, the data argue for adding 2–3 days per week of strength training rather than only increasing cardio volume. If someone hates gyms, resistance work can still mean home squats, push-ups against a wall, resistance bands, carrying, step-ups, or machine circuits.
Aerobic-Only Exercise Was Null in This Analysis
Aerobic exercise alone was not significantly associated with PHQ-9 or GAD-7 scores after matching. That does not erase randomized-trial evidence that aerobic exercise can reduce depressive symptoms.2,3 It does narrow the claim for this Korean observational dataset.
- Measurement problem: survey categories may not capture intensity, progression, adherence, or whether aerobic exercise was prescribed for illness.
- Selection problem: people with pain, frailty, cardiometabolic illness, or anxiety may choose walking because it is accessible, which can dilute apparent benefit.
- Comparison problem: resistance exercise may identify a subgroup with better baseline function or more structured routines despite matching.
Exercise Trials Support Both Cardio and Strength Training for Depression
Trial context: meta-analyses generally support exercise for depression, with benefits across aerobic, resistance, and mixed programs.2,3 Resistance training has also shown anxiolytic effects in prior syntheses.4
The Korean analysis adds a public-health angle: in a representative adult sample, resistance exercise may be underused in mental-health messaging compared with walking, running, and cycling. The result should push recommendations toward a combined model rather than an aerobic-only script.
Evidence-strength note: because the study is cross-sectional, it can support association and hypothesis generation. It cannot determine dose-response, treatment effect, or whether starting resistance exercise would lower PHQ-9 or GAD-7 in a depressed person.
Women and Older Adults May Be High-Yield Strength-Training Groups
Subgroup analyses in Yun et al. indicated stronger resistance-exercise associations in women and older adults.1 That does not prove that sex or age caused a larger response. It may reflect baseline activity patterns, muscle-strengthening gaps, comorbidity, pain, retirement schedule, body composition, or who can realistically add structured lifting without replacing other activity.
Program implication: strength training may be especially worth offering when the default advice has been only walking. Older adults and women are often steered toward low-intensity cardio for safety, but supervised or appropriately scaled resistance work can target function, confidence, fall risk, metabolic health, and mood at the same time.
Why Strength Training Could Have a Different Mental-Health Signal
Aerobic exercise is often framed as the default mental-health exercise because it improves cardiorespiratory fitness and has a long trial literature. Resistance exercise may work through partly different routes. It creates progressive mastery, increases muscle strength, improves glucose handling, reduces frailty, and can change body confidence in a way that walking alone may not.
Muscle as endocrine tissue: contracting skeletal muscle releases signaling molecules that influence inflammation, metabolism, vascular function, and brain adaptation. That does not make lifting a direct antidepressant, but it gives resistance training a biological route beyond distraction or willpower.
- Behavioral route: visible strength gains can build self-efficacy.
- Sleep route: regular training can consolidate sleep pressure and circadian rhythm.
- Metabolic route: improved insulin sensitivity may indirectly affect fatigue and mood.
- Pain route: stronger muscles and joints may reduce avoidance and disability.
How to Apply the Finding Without Overselling It
The Yun study supports a practical starting point: build exercise advice around both cardio and strength, then adapt to what the person will actually do. For a sedentary anxious person, that might mean 10 minutes of walking plus 2 sets of wall push-ups and chair squats. For a depressed person who already walks, it may mean adding machines, bands, or dumbbells twice weekly.
Adherence comes first: a perfect program abandoned after 9 days loses to a plain routine repeated for 6 months. Strength work should start below the intimidation threshold, progress slowly, and avoid injury. The target is a repeatable habit, not a fitness identity.
Care context: medication, psychotherapy, sleep treatment, pain management, and social support still matter. Exercise is a useful lever because it affects many systems at once; it is not a substitute for care when depression is severe, suicidal, psychotic, bipolar, or medically complicated.
A Simple Program Beats a Perfect Exercise Theory
A practical resistance plan can start with 6 movements: squat or sit-to-stand, hip hinge, push, pull, carry, and calf or step work. For anxious or depressed beginners, the dose can be deliberately small: 1-2 sets, 2 days per week, with an easy walk on other days. The goal is to build a routine that survives low-motivation weeks.
Progression rule: increase repetitions, load, or sets only when the current dose feels repeatable. Pain spikes, dizziness, chest symptoms, severe eating-disorder risk, and unstable medical disease require medical guidance rather than generic exercise advice.
Resistance Training Should Be Scaled to Depression Severity
For mild symptoms, a self-directed plan may be enough. For moderate depression, scheduling, accountability, and low-friction home equipment can make the difference between intention and repetition. For severe depression, suicidality, mania risk, psychosis, or medically complicated anxiety, exercise belongs inside a broader care plan rather than as the main intervention.
Low-barrier start: 15 minutes, 2 days per week, with movements that do not require a gym, can build the first adherence layer.
Program fit: people with anxiety may prefer predictable machine circuits, while people with depression may benefit from short home routines that require no travel. Matching the routine to friction points is part of the intervention.
Questions About Resistance Exercise for Depression and Anxiety
Should resistance exercise replace aerobic exercise?
No. Optimal mental-health exercise usually combines both. The useful update is that strength training should not be treated as optional decoration after cardio.
How much strength training is enough?
Most public-health guidance starts with 2 days per week of major muscle-group resistance exercise. For mental health, consistency and progression matter more than a perfect split.
Does this prove lifting treats depression?
No. Randomized trials are needed for treatment effects. This study shows that in a large Korean survey, resistance exercise marked lower depression and anxiety scores after matching.
References
- Comparative Associations of Aerobic Exercise and Resistance Exercise With Depression and Anxiety in Korean Adults: A Nationwide Propensity Score Matching Analysis. Yun YJ, Lee Y, Kwon YJ, Lee JW. Journal of Korean Medical Science. 2026;41:e123. doi:10.3346/jkms.2026.41.e123
- Exercise as a treatment for depression: a meta-analysis adjusting for publication bias. Schuch FB, Vancampfort D, Richards J, et al. Journal of Psychiatric Research. 2016;77:42–51. doi:10.1016/j.jpsychires.2016.02.023
- Effect of exercise for depression: systematic review and network meta-analysis. Noetel M, Sanders T, Gallardo-Gomez D, et al. BMJ. 2024;384:e075847. doi:10.1136/bmj-2023-075847
- The anxiolytic effects of resistance exercise. Gordon BR, McDowell CP, Lyons M, Herring MP. Sports Medicine. 2017;47:2521–2532. doi:10.1007/s40279-017-0769-0