A 2026 ECG analysis involving 269 healthy young adults found that sex differences in resting heart-rate dynamics appeared in very short 2-5 second fluctuations, not in the usual 5-minute heart rate variability averages. The short-window similarity graph metric predicted male sex with an odds ratio of 2.78 (95% CI 1.32-5.86), while conventional lnRMSSD, lnHF-HRV, and lnLF-HRV did not independently separate males from females.1
Research Highlights
- Short-window dynamics carried the signal: in 269 healthy adults aged 18-30 years, the graph-theory metric edges 2+2 was associated with male sex (OR 2.78; 95% CI 1.32-5.86; p = 0.007).1
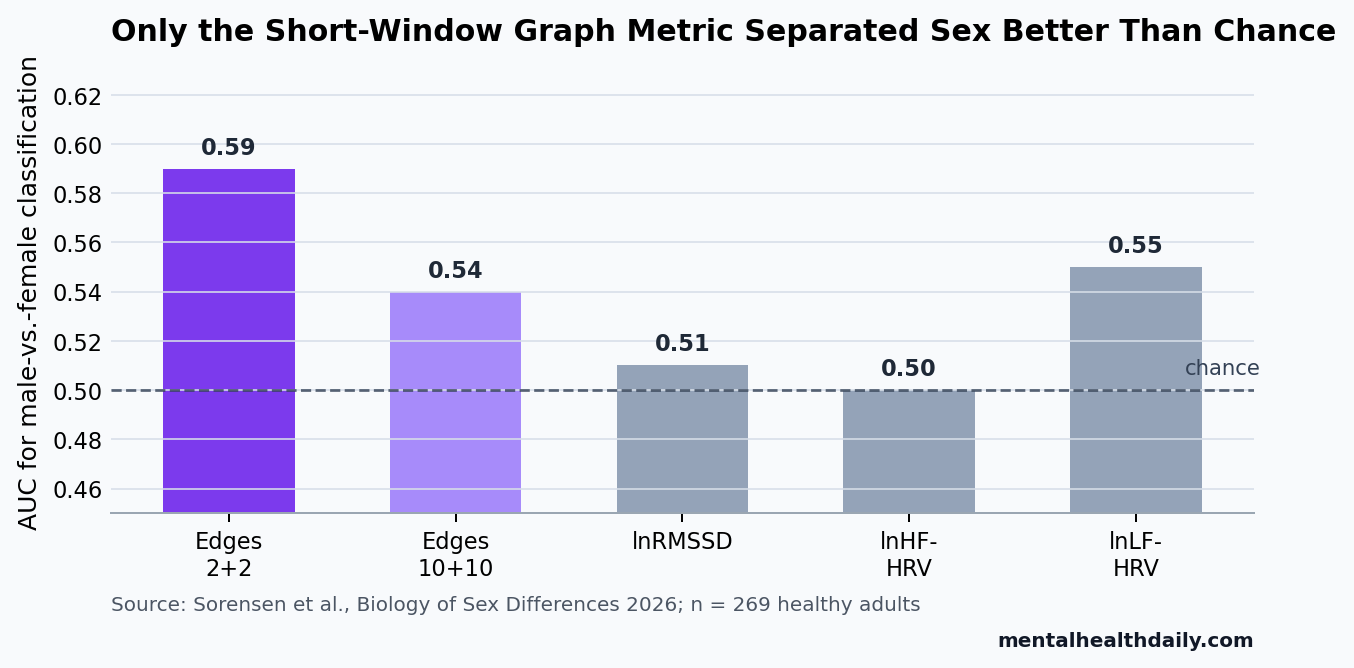
- Standard HRV averages missed the split: lnRMSSD, lnHF-HRV, and lnLF-HRV had nonsignificant odds ratios when tested as separate predictors, with AUC values only 0.50-0.55.1
- The best model was still modest: edges 2+2 had the highest AUC at 0.59, so the method detected a group-level pattern rather than a useful individual classifier.1
- The direction matched adult HRV meta-analyses: males showed greater interbeat-interval interrelatedness than females, meaning lower short-scale variability, while adult meta-analytic work generally finds higher resting HRV in females.2
- Clinical translation needs restraint: HRV is linked to emotion regulation and psychopathology across studies, but a 5-minute resting ECG marker cannot diagnose anxiety, depression, or stress resilience by itself.5,6
Heart rate variability (HRV) is the natural variation in time between heartbeats. Higher vagally mediated HRV usually means the parasympathetic branch of the autonomic nervous system can adjust heart rate flexibly, but HRV is a regulatory marker, not a direct readout of personality, emotion, or mental illness.
Sørensen et al. tested a narrower question: whether young adults show sex differences in rapid spontaneous interbeat-interval patterns that standard HRV summaries miss. That distinction matters because common HRV measures average several minutes of data, while vagal effects can shift heart timing within 1-2 beats.
Edges 2+2 Detected the Male-vs.-Female Difference
The 2026 study pooled resting electrocardiogram recordings from 3 university-based projects in Norway and the United States. After exclusions for missing age/sex data, age over 30 years, and extreme graph-metric outliers, the final analysis included 269 healthy adults aged 18-30 years; 141 participants were male.
Electrocardiogram (ECG) recording measures the heart’s electrical activity. The researchers used 5-minute resting ECG segments, corrected artifacts, and extracted both conventional HRV measures and a similarity graph metric from interbeat intervals.
Similarity graph theory means each heartbeat interval becomes a node, and intervals that are similar enough are connected by edges. In this study, the key metric was edges 2+2: a short sliding window centered on one heartbeat interval with 2 neighboring intervals on each side, covering roughly 2-5 seconds of heart timing.
Higher edges 2+2 values mean adjacent interbeat intervals are more similar to each other. In ordinary HRV language, that points to lower rapid variability. Males had higher edges 2+2 values than females, with a common language effect size of 0.60; a randomly selected male had a 60% probability of having a higher edges 2+2 value than a randomly selected female.
Primary regression result: each 1-unit increase in edges 2+2 was associated with higher odds of being male (OR 2.78; 95% CI 1.32-5.86; p = 0.007), adjusted for age and body mass index.
IQR-scaled result: a 1-interquartile-range increase in edges 2+2 corresponded to OR 1.491 (95% CI 1.122-2.015), which is a more intuitive shift from the lower to upper middle of the observed distribution.
Conventional 5-Minute HRV Metrics Did Not Independently Separate Sex
lnRMSSD is the natural-log version of the root mean square of successive differences between normal heartbeats. It is often used as a time-domain marker of short-term vagal regulation. lnHF-HRV is the log-transformed high-frequency power band, another common vagally mediated HRV measure, but one that depends more on respiratory rhythm.
In separate age- and BMI-adjusted models, lnRMSSD, lnHF-HRV, and lnLF-HRV did not significantly predict sex. Their AUC values were near chance: 0.51 for lnRMSSD, 0.50 for lnHF-HRV, and 0.55 for lnLF-HRV. Edges 10+10, a longer similarity-graph window, also failed to separate sex clearly (AUC 0.54).
The combined models sharpened the interpretation. When edges 2+2 and lnRMSSD were entered together, edges 2+2 strengthened to OR 4.53 (95% CI 1.83-11.20; p = 0.001), and lnRMSSD also reached significance (OR 1.73; 95% CI 1.06-2.81; p = 0.028). After further adjustment for mean heart rate and respiration rate, only edges 2+2 remained significant.
That pattern does not make conventional HRV useless. It says that, in healthy young adults, averaged HRV measures may be too coarse for a subtle sex-linked pattern that unfolds over a few beats. RMSSD may still share relevant variance, but the short-window graph metric retained the cleaner association after physiological adjustment.
AUC 0.59 Means Detection, Not Classification
The strongest performance number was modest. Edges 2+2 produced an AUC of 0.59, where 0.50 means chance-level discrimination and 1.00 means perfect separation. Across tested similarity thresholds from 0.5% to 4%, model performance stayed in the same range, with AUC values from 0.59 to 0.60 and Nagelkerke R2 values from 0.048 to 0.053.
What the method can support: a group-level claim that very short interbeat-interval organization differed by sex in this healthy young-adult sample.
What it cannot support: an individual prediction tool, a clinical stress test, or a claim that any 1 person’s autonomic flexibility can be inferred from sex or from this graph metric alone.
The power calculation fits the same calibrated reading. The observed OR of 2.78 gave an estimated 74% statistical power; 80% power would have required OR 3.05. The result is not a fragile p-value in isolation, but it is also not a high-accuracy classifier.
Adult HRV Meta-Analyses Point in the Same Direction
Koenig and Thayer’s 2016 meta-analysis found that healthy adult females generally show higher resting HRV than males, although the exact pattern depends on metric choice, transformation, and age.2 Koenig et al. later reported a different developmental picture in children and adolescents, where sex differences in resting vagal activity follow an age-dependent pattern.3
The Sørensen result sits inside that developmental transition. Young adulthood is a hard window because conventional adult sex differences may be present but small, while adolescent patterns are still close enough to complicate interpretation. A metric built around 2-5 second fluctuations may expose a female-favoring flexibility pattern before it becomes obvious in averaged HRV summaries.
Biologically, that claim is plausible but not proven by this design.
Mechanism caveat: estradiol, progesterone, testosterone, dopamine signaling, respiration, physical activity, and stress state can all influence autonomic regulation. The study did not measure menstrual cycle phase, hormonal contraceptive use, medication use, smoking, exercise, diet, or repeated-day stability, so mechanism language needs to stay conditional.
Graph Theory May Help HRV Research Avoid Averaging Away Fast Physiology
Kvadsheim et al. previously used a graph-theory approach to interbeat intervals in adolescents with attention-deficit/hyperactivity disorder (ADHD), a neurodevelopmental condition involving attention, impulse control, and self-regulation. That work suggested altered autonomic functioning in ADHD and gave the 2026 analysis a methodological precedent.4
The broader HRV literature explains why this approach is attractive. Beauchaine and Thayer described HRV as a transdiagnostic biomarker candidate across psychopathology, while Kemp et al. found lower HRV in depression and examined effects of antidepressant treatment.5,6 Those findings keep HRV relevant to mental health, but they also make overinterpretation tempting.
Short-window graph metrics could improve research when the question is about rapid autonomic adjustment alongside average resting tone. They may be especially useful in studies of stress recovery, emotion regulation, attention, panic physiology, or treatment response where second-by-second autonomic flexibility is part of the hypothesis.
The next validation step is reliability. A metric can be sensitive and still be unstable across days, devices, breathing conditions, or preprocessing pipelines. Before edges 2+2 becomes a routine psychophysiology endpoint, studies need repeated recordings, controlled respiration comparisons, menstrual-cycle reporting, and direct tests against behavioral or clinical outcomes.
Practical Takeaways for Reading HRV Studies
- Metric choice changes the answer: RMSSD, HF-HRV, entropy, detrended fluctuation analysis, and graph metrics do not measure the same thing. A null result in 1 HRV metric is not a null result for all autonomic dynamics.
- Time scale matters: 5-minute averages can be reliable trait markers, but they can miss fast changes that happen across a few beats.
- Sex differences are age-sensitive: child, adolescent, young-adult, and older-adult HRV patterns should not be collapsed into a single blanket rule.
- Clinical claims require outcome data: an autonomic marker becomes clinically useful only when it predicts symptoms, functioning, treatment response, or risk beyond ordinary clinical information.
Questions About Resting HRV and Sex Differences
Did the study show that females have healthier autonomic regulation?
No. Females showed lower interbeat-interval interrelatedness in the short-window graph metric, consistent with higher rapid variability. That is compatible with flexible autonomic regulation, but the study did not measure health outcomes, stress recovery, or clinical symptoms.
Why did standard HRV measures miss the difference?
Standard metrics summarize variability across the full 5-minute recording. The sex-linked signal in this study appeared strongest in 2-5 second organization, where vagal influences can change heart timing quickly.
Can edges 2+2 diagnose anxiety or stress vulnerability?
No. The AUC was only 0.59 for sex classification, and the sample involved healthy young adults. The metric is a research tool until it is validated against clinical outcomes and repeated recordings.
Should HRV researchers include sex as a covariate?
Usually yes, but sex should not be treated as a simple correction term. Age, respiration, hormones, menstrual cycle phase, medications, fitness, and study context can all change how sex-linked autonomic patterns appear.
References
- Sørensen L, Kvadsheim E, Koenig J, Thayer JF, Williams DP, MacDonald HJ, et al. Capturing sex differences in spontaneous autonomic fluctuations of resting heart rate using a similarity graph theory approach. Biology of Sex Differences. 2026. https://doi.org/10.1186/s13293-026-00904-x
- Koenig J, Thayer JF. Sex differences in healthy human heart rate variability: A meta-analysis. Neuroscience & Biobehavioral Reviews. 2016;64:288-310. https://doi.org/10.1016/j.neubiorev.2016.03.007
- Koenig J, Rash JA, Campbell TS, Thayer JF, Kaess M. A Meta-Analysis on Sex Differences in Resting-State Vagal Activity in Children and Adolescents. Frontiers in Physiology. 2017;8:582. https://doi.org/10.3389/fphys.2017.00582
- Kvadsheim E, Fasmer OB, Fasmer EE, Hauge ER, Thayer JF, Osnes B, et al. Innovative approaches in investigating inter-beat intervals: Graph theoretical method suggests altered autonomic functioning in adolescents with ADHD. Psychophysiology. 2022;59:e14005. https://doi.org/10.1111/psyp.14005
- Beauchaine TP, Thayer JF. Heart rate variability as a transdiagnostic biomarker of psychopathology. International Journal of Psychophysiology. 2015;98:338-350. https://doi.org/10.1016/j.ijpsycho.2015.08.004
- Kemp AH, Quintana DS, Gray MA, Felmingham KL, Brown K, Gatt JM. Impact of depression and antidepressant treatment on heart rate variability: a review and meta-analysis. Biological Psychiatry. 2010;67:1067-1074. https://doi.org/10.1016/j.biopsych.2009.12.012
- Laborde S, Mosley E, Thayer JF. Heart Rate Variability and Cardiac Vagal Tone in Psychophysiological Research: Recommendations for Experiment Planning, Data Analysis, and Data Reporting. Frontiers in Psychology. 2017;8:213. https://doi.org/10.3389/fpsyg.2017.00213
- Sacha J. Interaction between heart rate and heart rate variability. Annals of Noninvasive Electrocardiology. 2014;19:207-216. https://doi.org/10.1111/anec.12148