A 2026 serum multiomics study linked occupational noise exposure to tinnitus severity mostly through metabolism: 10 metabolites, including GABA, fumaric acid, and steroid hormone precursors, statistically mediated 92% of the exposure-tinnitus association.1 The result is not a clinical blood test yet, but it pushes tinnitus biology beyond the ear-only frame toward a metabolism-immunity model that can be tested prospectively.
Research Highlights
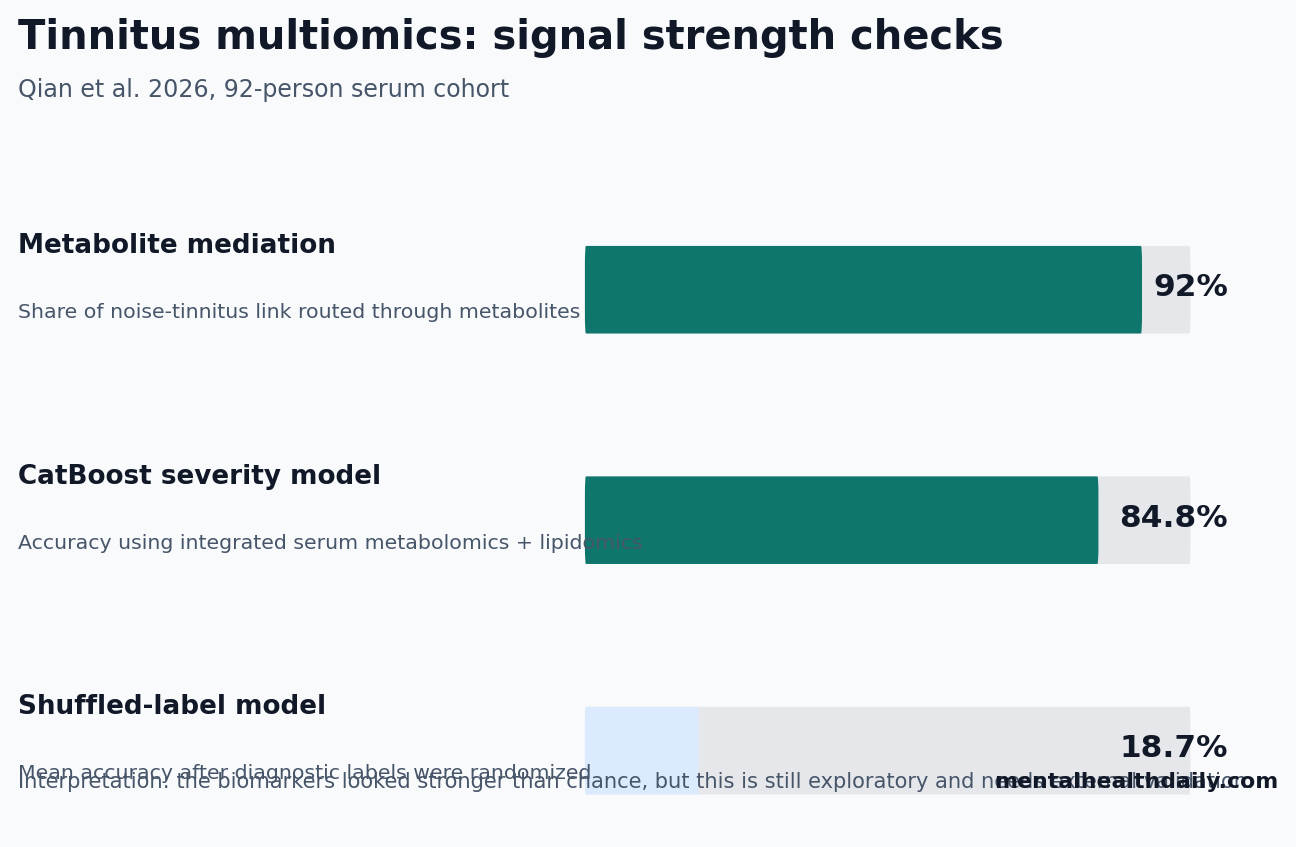
- Metabolites carried most of the signal: mediation analysis estimated a 92% indirect effect linking occupational noise exposure to tinnitus through serum metabolites, with p < 0.001.1
- Severity prediction beat chance: a CatBoost model using metabolomic and lipidomic features classified tinnitus severity with 84.8% accuracy, while shuffled-label models averaged about 18.7% accuracy.1
- GABA was the reader-facing clue: reduced GABA (gamma-aminobutyric acid, the main inhibitory neurotransmitter) tracked with a model in which weaker inhibition may leave auditory circuits more excitable than normal.1
- Lipids appeared early: sphingolipids and other lipid classes separated even grade I tinnitus from controls, suggesting membrane and inflammatory signaling may shift before broader metabolic disruption.1
- The evidence is still exploratory: the cohort included 92 participants, exposure was reconstructed from job categories, and the biomarker model needs external validation in cohorts larger than 92 participants before clinical use.1
Tinnitus means hearing sound without an external source. The symptom is usually discussed through hearing loss, cochlear injury, auditory-cortex overactivity, anxiety, sleep disruption, or maladaptive attention. Qian et al. tested a different layer: whether chronic occupational noise exposure leaves a measurable serum signature that connects environmental exposure to tinnitus severity.
The useful calibration is narrow. This study does not prove that GABA supplements, lipid-lowering interventions, or immune drugs treat tinnitus. It does suggest that tinnitus severity may be partly readable through blood chemistry, especially when noise exposure, lipids, inhibitory neurotransmission, and immune polarization are studied together.
92% of the Noise-Tinnitus Link Ran Through Metabolites
Qian et al. recruited 156 people in Shanghai between January 2020 and October 2022. After exclusions, 92 high-quality serum samples remained for the omics discovery phase: 74 tinnitus patients and 18 controls. Among the tinnitus patients, 73 had complete clinical, immunological, metabolomic, and lipidomic data for the mechanistic analyses.1
Exposure classification: occupational noise was reconstructed with a job-exposure matrix using 8-hour time-weighted average categories: low exposure below 80 dB(A), moderate exposure from 80 to 85 dB(A), and high exposure at or above 85 dB(A). This is better than a vague occupational-history checkbox, but it is still not personal dosimetry.
Main exposure model: compared with low occupational noise exposure, moderate exposure was associated with much higher tinnitus odds after adjustment (adjusted OR = 27.4, 95% CI 1.75-5050, p = 0.013). The confidence interval was enormous, which means the direction looked strong but the estimate was imprecise.
High exposure did not show the same confirmed association as low exposure (adjusted OR = 1.46, 95% CI 0.08-27.6, p = 0.819), likely reflecting small subgroup size and separation problems rather than a clean dose-response curve.1
The headline result came from mediation analysis. A panel of 10 metabolites statistically explained most of the occupational noise-tinnitus association, with a total indirect effect of 92% (p < 0.001). In plain English, the model said the noise signal was mostly routed through measurable metabolic changes rather than appearing as a direct exposure-to-symptom jump.
That does not prove causality. Mediation analysis is a statistical attempt to estimate whether one variable helps explain the link between another variable and an outcome. In a cross-sectional study, it can propose a pathway; it cannot prove that occupational noise first changed serum metabolites and then caused tinnitus.
GABA and Sphingolipids Made the Signal Biologically Plausible
Two biomarker families make the paper more interesting than a generic machine-learning exercise.
- GABA: gamma-aminobutyric acid is the main inhibitory neurotransmitter in the brain. In auditory circuits, weaker inhibitory tone can make spontaneous neural activity harder to suppress, which is one plausible route to phantom sound perception.
- Sphingolipids: these are membrane lipids that also act as signaling molecules. They can influence cell death, inflammation, oxidative stress, and membrane excitability, which gives them a plausible bridge between environmental injury and neural symptoms.
Qian et al. found that GABA ranked among the top predictive features in the CatBoost model. Lower serum GABA also fit their broader pattern: tinnitus severity, anxiety/depression scores, Th1 immune activity, and metabolic disruption moved together in ways consistent with weaker inhibitory control and more inflammation.1
Lipidomics added timing information. Metabolomic profiles for grade I tinnitus still looked close to controls, but lipidomic profiles already separated grade I patients from controls. The study identified 428 significantly altered lipid molecules, including glycerol esters, glycerophospholipids, cardiolipin, sphingomyelin, and sphingosine-based lipids.1
Mechanistically, the staged model is coherent: early lipid disruption may make auditory cells more vulnerable, mitochondrial energy stress may impair adenosine triphosphate (ATP, the cell’s main energy currency), and weaker GABAergic inhibition may leave auditory circuits more excitable. The problem is that coherence is not confirmation. The next test is whether these markers predict future tinnitus onset or worsening in people whose noise exposure is measured directly.
Machine Learning Found a Real Signal, Not a Ready Diagnostic Test
The predictive modeling used 4779 features: 11 demographic or clinical variables, 732 metabolomic features, and 4036 lipidomic features. The outcome was tinnitus severity from 0 for controls through grade IV for severe impairment.1
CatBoost performed best among the tested algorithms, with 84.8% accuracy, mean absolute error of 0.174, and macro F1 score of 0.8467. LightGBM was close at 83.7% accuracy. Logistic regression reached 79.3%, which suggests part of the signal was nonlinear but also shows that simpler models were not useless.
Overfitting check: after researchers shuffled diagnostic labels 100 times, the null models averaged about 18.7% accuracy (p < 0.01 vs the real model). That matters because a 92-person cohort with 4779 candidate features is exactly the kind of setting where a model can look impressive by memorizing noise. Nested cross-validation and permutation testing reduce that risk; they do not replace independent replication.
Inflammation Fits the Tinnitus Literature, but It Is Not the Whole Story
Inflammation is not new in tinnitus research. Wang et al. showed in rodent models that noise-induced tinnitus-like behavior can involve neuroinflammation and synaptic imbalance.2 Mennink et al. reviewed inflammation findings in tinnitus and found enough signal to take the pathway seriously, while also showing why heterogeneous immune markers are hard to turn into a clean clinical test.4
Qian et al. sharpened the immune piece by profiling Th1-type inflammation. Th1 cells are T helper immune cells that promote cellular inflammatory responses, often through cytokines such as interferon gamma and interleukin-2.
In the 2026 study, Th1 percentage was associated with tinnitus in the adjusted model (adjusted OR = 1.23 per percentage point, 95% CI 1.07-1.55, p < 0.001), while regulatory T cells moved in the opposite direction (adjusted OR = 0.57, 95% CI 0.35-0.93, p = 0.024).1
The paper’s own mediation results are useful here because they prevent overclaiming. Metabolic and lipid markers looked upstream; Th1/Treg balance looked more downstream. In other words, immune activation may help sustain tinnitus, but the strongest statistical bridge from occupational noise to tinnitus ran through metabolites and lipids.
Sedley et al. also matters for calibration. Their human auditory-cortex neurochemistry work connected tinnitus presence and severity to neural chemistry inside auditory cortex.3 Blood biomarkers are easier to sample, but tinnitus is still a brain-and-ear symptom. A serum panel will need to prove that it adds information beyond audiometry, symptom scales, neuroimaging, and clinical history.
What This Study Can and Cannot Support
Supported: serum multiomics found a coherent metabolic, lipidomic, and immune signature associated with occupational noise exposure and tinnitus severity in one Shanghai cohort. The signal was strong enough to classify severity better than shuffled labels and biologically plausible enough to justify follow-up.
Not supported yet: clinical diagnosis, screening, treatment selection, or supplement recommendations. The cross-sectional design cannot establish time order, and job-exposure matrices can misclassify real noise dose. Late-stage tinnitus subgroups were modest, which makes the largest estimates unstable.
Best next validation: follow noise-exposed workers over time with personal dosimetry, repeated tinnitus assessments, audiometry, and repeated serum samples. If sphingolipids and GABA shift before tinnitus worsens, the biomarker claim becomes much stronger. If they shift only after symptoms are established, they may still be useful for staging, but not for early warning.
Questions About Noise Exposure, Tinnitus, and Blood Biomarkers
Does this mean tinnitus can be diagnosed with a blood test?
No. The 2026 study found a promising research signal, not a validated diagnostic assay. The model needs external validation in larger cohorts before it can be used clinically.
Is occupational noise still the main practical target?
Yes. Even if the metabolism-immunity pathway is real, the upstream exposure remains noise. Hearing protection, exposure reduction, and workplace controls are still the intervention layer with the clearest evidence base.
Should people with tinnitus take GABA or lipid-targeting supplements?
This study does not support that. Serum GABA and sphingolipids may be biomarkers or pathway clues, but changing them without proof could be ineffective or misleading. Treatment decisions still need clinical evaluation, hearing assessment, and evidence-based tinnitus management.
References
- Qian T, Wang G, Li P, et al. Metabolic Reprogramming Bridges Environmental Exposure and Tinnitus Severity: Evidence from AI-Driven Serum Multiomics. Environment & Health. 2026;4:585-600. https://doi.org/10.1021/envhealth.5c00512
- Wang W, Zhang LS, Zinsmaier AK, et al. Neuroinflammation mediates noise-induced synaptic imbalance and tinnitus in rodent models. PLOS Biology. 2019;17:e3000307. https://doi.org/10.1371/journal.pbio.3000307
- Sedley W, Parikh J, Edden RAE, Tait V, Blamire A, Griffiths TD. Human Auditory Cortex Neurochemistry Reflects the Presence and Severity of Tinnitus. Journal of Neuroscience. 2015;35:14822-14828. https://doi.org/10.1523/JNEUROSCI.2695-15.2015
- Mennink LM, Aalbers MW, van Dijk P, van Dijk JMC. The Role of Inflammation in Tinnitus: A Systematic Review and Meta-Analysis. Journal of Clinical Medicine. 2022;11:1000. https://doi.org/10.3390/jcm11041000
- Kang DW, Kim SS, Park DC, Kim SH, Yeo SG. Objective and Measurable Biomarkers in Chronic Subjective Tinnitus. International Journal of Molecular Sciences. 2021;22:6619. https://doi.org/10.3390/ijms22126619