A 2026 multicenter Italian cohort followed 216 early Parkinson’s disease patients for 24 months after levodopa initiation and found sex/gender differences in non-motor symptom burden.1 Women had higher anxiety, pain, mobility, and emotional-well-being burden, while men had higher hypersexuality.
Research Highlights
- Longitudinal sample: The study followed 216 early levodopa-naive Parkinson patients, including 139 men and 77 women, from 17 Italian centers.1
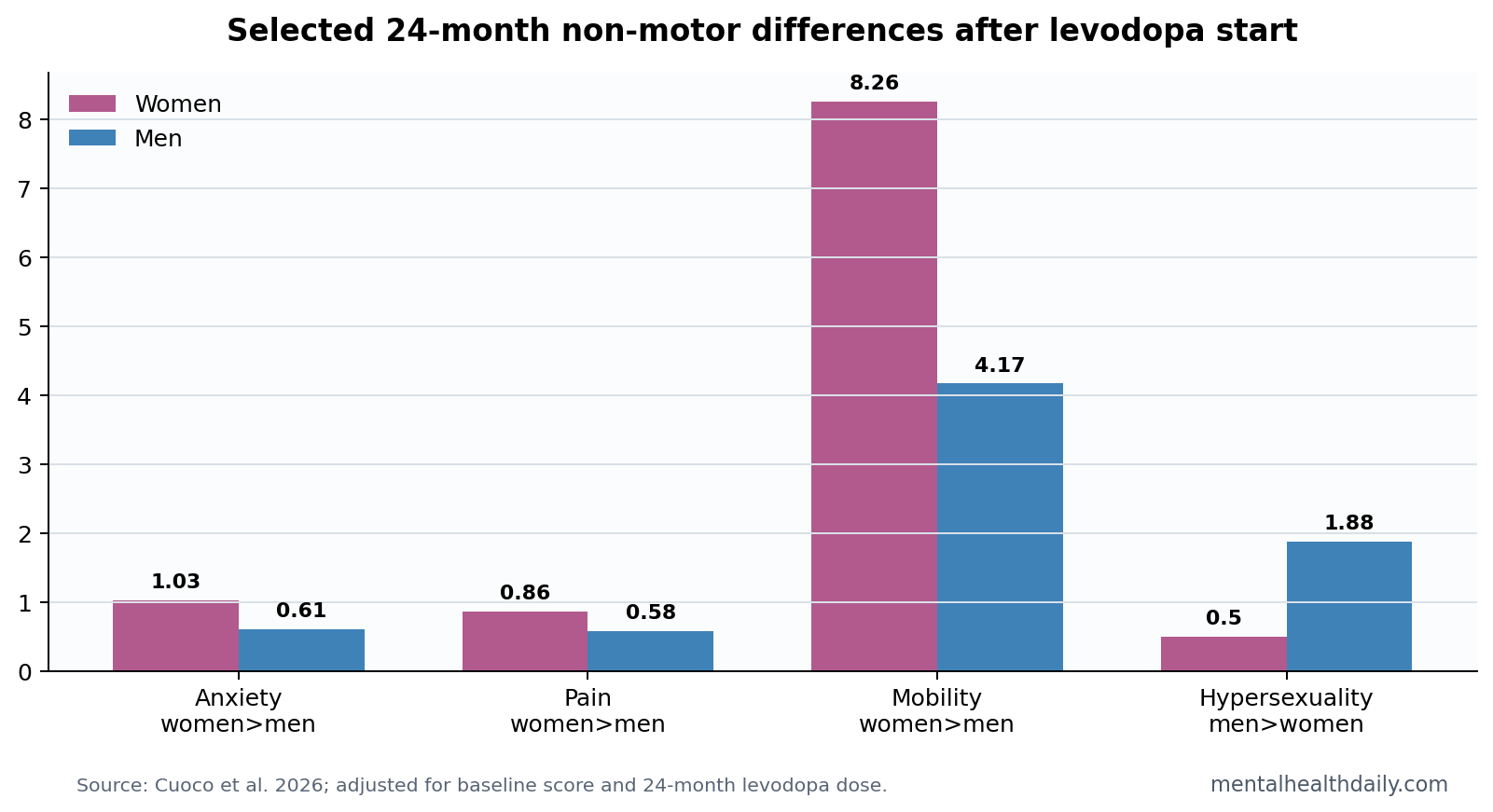
- Anxiety stayed higher in women: At 24 months, anxious mood was 1.03 in women vs. 0.61 in men after adjustment, p = 0.015.1
- Pain stayed higher in women: Pain was 0.86 in women vs. 0.58 in men, p = 0.012, after baseline and dose adjustment.1
- Hypersexuality was higher in men: Men scored 1.88 vs. 0.50 in women, p < 0.001.1
- Dose did not erase the pattern: Men had higher 24-month levodopa dose, 327.64 vs. 286.69 mg/day, making adjusted models important.1
Non-motor symptoms are Parkinson’s disease problems outside tremor, rigidity, slowness, and gait. They include anxiety, depression, pain, sleep disruption, autonomic symptoms, cognitive changes, fatigue, impulse-control symptoms, and quality-of-life burden.
Levodopa is the main dopamine-replacement treatment for Parkinson’s motor symptoms. It can improve movement, but dopamine replacement can also intersect with mood, impulse control, sleep, and autonomic symptoms.
Women Had Higher Anxiety, Pain, Mobility, and Emotional Burden
Cuoco et al. reported several baseline differences, then tested 24-month outcomes after adjusting for baseline scores and levodopa dose. At 24 months, women had higher cognitive impairment, anxious mood, pain, orthostatic/fainting symptoms, PDQ-39 mobility burden, and emotional-well-being burden.1
The anxiety and pain differences were clinically easy to read. Anxious mood was 1.03 in women vs. 0.61 in men, p = 0.015. Pain was 0.86 vs. 0.58, p = 0.012. PDQ-39 mobility burden was also higher in women, 8.26 vs. 4.17, p = 0.009.
PDQ-39 is a Parkinson’s quality-of-life questionnaire. A higher mobility score means more difficulty with movement-related daily functioning, while a higher emotional well-being score means more mood and emotional burden. Those are patient-centered outcomes, not narrow motor exam findings.
The most useful way to read the female-higher pattern is by symptom domain, not by a single global severity claim:
- Anxiety and pain: both remained higher in women after adjustment, which makes them screening targets at routine follow-up rather than optional side questions.
- Mobility and emotional well-being: PDQ-39 differences suggest that quality-of-life burden can stay visible even when the visit is organized around motor medication response.
- Cognition and orthostatic symptoms: the signal was broader than mood alone, so a narrow depression-only screen would miss part of the non-motor pattern.
The pattern matters because pain, anxiety, and orthostatic symptoms can be underrecognized when a visit focuses on tremor, bradykinesia, rigidity, and medication timing. A patient can have acceptable motor control and still have poor quality of life because the non-motor symptom load is high.
Men Had Higher Hypersexuality Despite Higher Levodopa Dose
Men showed the clearest male-higher signal for hypersexuality: 1.88 vs. 0.50, p < 0.001. That fits the broader clinical concern that dopamine replacement can contribute to impulse-control symptoms in susceptible patients.
The dose detail matters. Men received slightly higher daily levodopa at 24 months, 327.64 vs. 286.69 mg/day, p = 0.016. The researchers adjusted for dose, but observational adjustment cannot prove that dose, sex biology, reporting behavior, or clinical monitoring fully explain the difference.
Hypersexuality is an impulse-control symptom involving increased or difficult-to-control sexual thoughts or behavior. In Parkinson’s disease, impulse-control symptoms are clinically important because dopaminergic drugs can amplify reward-seeking behavior in vulnerable patients.
The male-higher hypersexuality result should prompt direct screening, not embarrassment or silence. Patients often do not volunteer impulse-control symptoms unless clinicians ask plainly. Family members may notice spending, gambling, pornography use, compulsive shopping, binge eating, or sexual-behavior changes before the patient frames them as medication-related.
Sex/Gender Differences Should Change Screening, Not Stereotyping
Parkinson’s disease is often introduced through motor symptoms, but non-motor symptoms can dominate quality of life.2 Sex-difference reviews have also warned that women and men can differ in symptom profiles, care pathways, and treatment complications.3
Clinical implication: women with early Parkinson’s should be actively asked about anxiety, pain, orthostatic symptoms, mobility burden, and emotional well-being. Men should be actively asked about impulse-control and sexual-behavior symptoms, especially after dopaminergic treatment starts.
Evidence-strength note: this was an observational cohort. The result can identify domains that deserve screening. It cannot reduce a patient’s symptoms to sex alone, and it cannot prove whether each difference came from biology, dose, reporting, clinical attention, or social context.
Binary sex/gender analysis is also a limitation. The reported groups may combine biological sex, gendered symptom reporting, treatment expectations, clinician behavior, body size, hormone exposure, comorbidity, and social support. The study can show that the groups differed; it cannot cleanly assign the cause of each difference.
Even with that limitation, symptom-specific screening is low-risk. Asking every early Parkinson patient about anxiety, pain, faintness, sexual behavior, sleep, constipation, urinary symptoms, cognition, and mood is better than assuming motor response to levodopa tells the whole story.
Levodopa Follow-Up Should Include Non-Motor Review
Levodopa follow-up often centers on dose timing, wearing off, dyskinesia, and motor response. Cuoco et al. point to a broader follow-up template. A 24-month visit should also ask which symptoms changed after treatment began and which quality-of-life domains stayed burdensome.
Useful follow-up domains:
- Mood: anxiety, depression, irritability, panic, and apathy.
- Pain and autonomic symptoms: pain, dizziness, faintness, constipation, urinary symptoms, sweating, and thermoregulation.
- Impulse control: hypersexuality, gambling, shopping, binge eating, and compulsive medication use.
- Function: mobility, falls, daily activities, emotional well-being, and caregiver burden.
That broader review can prevent 2 common misses. First, pain and anxiety may be treated as unrelated problems even when they are part of the Parkinson symptom burden. Second, impulse-control symptoms may be missed until they cause financial, relational, or safety harm. Both misses are avoidable when non-motor screening is routine.
Medication decisions should then be individualized. Higher levodopa dose can improve mobility and daily function, but dopaminergic exposure can also interact with hallucinations, sleepiness, orthostatic symptoms, and impulse control. A patient with excellent motor response and worsening non-motor symptoms still needs medication review.
The study also argues for measuring quality of life directly. Motor scores can look acceptable while PDQ-39 mobility or emotional well-being remains poor. Asking about the patient’s day-to-day life gives clinicians a better view than relying on tremor or rigidity alone.
It also helps separate treatable symptoms from vague disease burden. Pain may need medication review, physical therapy, sleep assessment, or neuropathy workup. Anxiety may need counseling, medication adjustment, or more predictable dose timing. Hypersexuality may need dopamine-agonist review, family-supported monitoring, and direct safety planning.
Future studies should test whether sex/gender differences persist across larger, more diverse cohorts and whether they predict treatment changes. It would also help to separate biological sex from gendered reporting, body size, hormone exposure, caregiver involvement, and clinician response. Those pieces may all contribute to the observed pattern.
The immediate reader-facing conclusion is straightforward: early Parkinson’s follow-up should include non-motor symptoms from the start. Levodopa response is important, but anxiety, pain, faintness, sexual-behavior changes, mobility burden, and emotional well-being can shape the patient’s actual disease experience just as strongly.
That conclusion is compatible with individualized care. A woman with low anxiety and no pain still needs impulse-control screening; a man with severe pain or orthostatic symptoms still needs those symptoms treated. The group pattern should widen the checklist, not narrow assumptions about any 1 patient.
Patient education should also name non-motor symptoms before they become crises. If patients and families know that mood, pain, faintness, and impulse-control changes can belong to the Parkinson treatment course, they are more likely to report them early and less likely to treat them as personal failures.
A practical visit template would pair motor review with a short non-motor checklist at every major dose change. That checklist does not need to be complicated: mood, pain, dizziness, sleep, constipation, urination, sexual behavior, spending or gambling, hallucinations, cognition, falls, and caregiver stress cover much of the risk surface.
The sex/gender signal should make that checklist more sensitive. Women in this cohort carried higher anxiety, pain, and quality-of-life burden; men carried higher hypersexuality. Both patterns are actionable only if the clinician asks before the symptom becomes the loudest problem in the room.
That is the clean clinical use of the study: widen early screening, then tailor care to the individual symptom pattern that actually appears during follow-up visits over time in practice.
Questions About Parkinson Non-Motor Sex Differences
Does levodopa cause these sex differences?
The study cannot prove that. It followed patients after levodopa initiation and adjusted for dose, but treatment exposure is only 1 part of the pattern.
Should clinicians screen men and women differently?
They should screen everyone broadly, then keep the sex-linked risk domains in mind so anxiety, pain, orthostatic symptoms, and impulse-control symptoms are not missed.
Do these findings apply to advanced Parkinson’s disease?
Not directly. The cohort involved early Parkinson’s disease over 24 months, so advanced disease and long-term treatment complications require separate evidence.
References
- Cuoco S, et al. Gender differences in non-motor symptoms and quality of life in early Parkinson’s disease after 24 months of levodopa treatment. Neurological Sciences. 2026. doi:10.1007/s10072-026-09031-2
- Chaudhuri KR, Healy DG, Schapira AHV. Non-motor symptoms of Parkinson’s disease: diagnosis and management. Lancet Neurology. 2006. doi:10.1016/s1474-4422(06)70373-8
- Miller IN, Cronin-Golomb A. Gender differences in Parkinson’s disease: clinical characteristics and cognition. Movement Disorders. 2013. doi:10.1002/mds.25312
- Picillo M, et al. The relevance of gender in Parkinson’s disease: a review. Journal of Neurology. 2017. doi:10.1007/s00415-016-8384-9