
Statins do not look like a dementia-prevention drug, but they do not look like a dementia hazard either. In 322,358 Kaiser Permanente Northern California patients followed for an average of 11.8 years, dementia diagnoses rose right after statins were started, then flattened: after the first year, the hazard ratio for Alzheimer’s disease and related dementias was 1.00.1
Research Highlights
- 322,358 patients over 11.8 years: Kaiser records gave the analysis enough follow-up to separate early diagnosis noise from long-term dementia risk.1
- Statin starters vs. matched nonstarters: 249,613 initiators were compared with people who had not started statins.1
- Year-1 diagnosis spike: dementia diagnoses were 46% higher after initiation, with the strongest spike in the first month.1
- Post-year-1 flatline: after the first year, the dementia hazard ratio was 1.00.1
- Heart/stroke risk, not dementia prevention: statins still make sense when cardiovascular risk warrants them.1,6
The cholesterol-dementia story is biologically plausible: high LDL cholesterol can feed atherosclerosis, atherosclerosis can raise stroke and small-vessel injury, and vascular injury can lower the brain’s reserve against Alzheimer’s pathology. APOE also sits at the intersection of lipid transport and Alzheimer’s disease risk.2 That makes the statin question tempting: if high LDL can damage the aging brain, maybe statins protect it.
The study by Zimmerman et al. is useful because it refuses the easiest answer. It does not say statins are secretly a dementia drug. It also does not validate the common patient worry that statins are quietly eroding memory. It says the best read of statin initiation, with long follow-up and an attempt to mimic randomization, is close to zero.
322,358 Patients, 249,613 Statin Initiators, 11.8 Years Follow-Up
The study used Kaiser Permanente Northern California electronic health records for members born before 1951 who had at least 4 years of continuous membership during the 1997–2010 eligibility window. Participants with prior dementia diagnoses or prior statin use during the run-in period were excluded.1
The sample is easier to understand as a study snapshot:
- Eligible pool: 705,061 Kaiser members born before 1951, with prior dementia diagnoses and prior statin use excluded.
- Matched analytic sample: 322,358 unique participants, including 249,613 statin initiators matched with comparable noninitiators.
- Baseline profile: mean age 67.4 years; 55.1% female.
- Follow-up: average 11.8 years, with first-year and after-year-1 estimates analyzed separately.1
The design matters. A plain comparison of statin users to nonusers is weak because people who receive statins differ from people who do not: they have different LDL levels, cardiovascular histories, health-care contact, diabetes rates, medication adherence, and preventive-care behavior. A target trial emulation tries to ask the cleaner question: what would happen if, at a defined baseline date, one otherwise eligible person initiated a statin and a similar person did not?
Zimmerman et al. matched statin initiators to up to 5 noninitiators on age and LDL cholesterol, then used inverse probability weighting to balance measured clinical variables. The primary contrast was intent-to-treat: starting statins versus not starting statins, not perfect long-term statin adherence versus never touching a statin.
First-Year Dementia Diagnoses Increased 46%
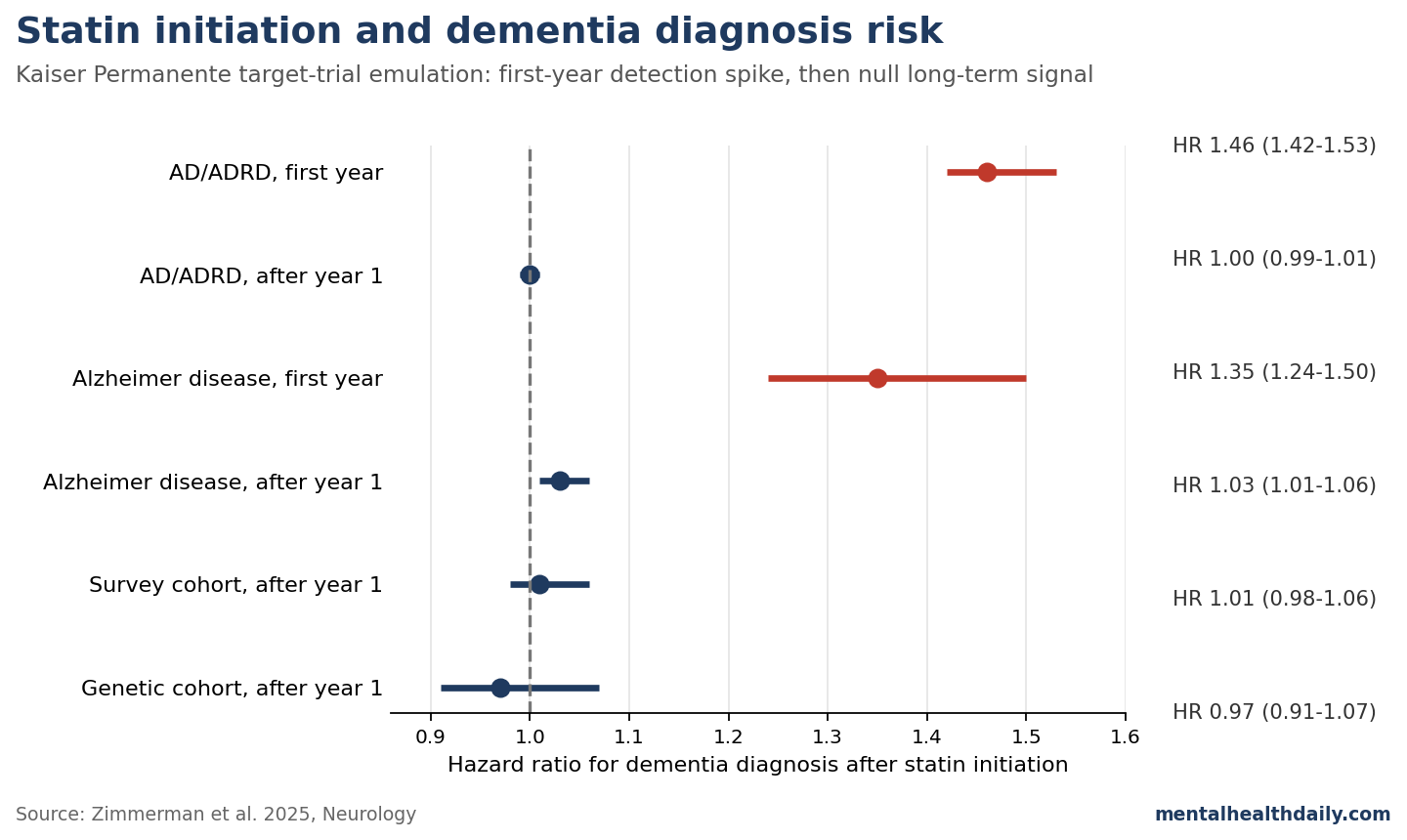
The result that will travel badly is the first-year number. During the first year after the initial statin prescription, AD/ADRD diagnoses were higher among initiators: HR 1.46 (95% CI 1.42–1.53). For Alzheimer’s disease alone, the first-year HR was 1.35 (95% CI 1.24–1.50).1
Read mechanically, that looks like statins rapidly increase dementia diagnoses. Read epidemiologically, it looks like detection bias. A statin prescription often appears after a cardiovascular risk review, abnormal lipid result, diabetes diagnosis, stroke or transient ischemic attack workup, or renewed contact with the health system. More contact means more chances for existing cognitive symptoms to be noticed, coded, and followed.
The paper tested this interpretation directly by varying the early window. The short-term elevation was strongest in the first month after initiation: HR 2.78 (95% CI 2.48–3.13), then attenuated rapidly. That time course is not biologically persuasive as a statin-causes-dementia mechanism. Dementia does not emerge within weeks because hepatic HMG-CoA reductase was inhibited. Medical observation does.
After Year 1: HR 1.00 for AD/ADRD, 1.03 for Alzheimer’s Disease
The long-term result is the opposite of a viral headline. After the first year, the fully adjusted AD/ADRD hazard ratio was 1.00 (95% CI 0.99–1.01). The Alzheimer’s disease-only estimate was slightly above the null at 1.03 (95% CI 1.01–1.06), but that is small enough to be clinically fragile and vulnerable to outcome misclassification.1
The nested cohorts do not rescue a hidden APOE story. In the survey cohort, which added education, income, general health, and survey language, the after-year-1 AD/ADRD HR was 1.01 (95% CI 0.98–1.06). In the genetic cohort, which added APOE-e4 allele count and ancestry principal components, the corresponding HR was 0.97 (95% CI 0.91–1.07).1
APOE-e4 is the obvious place to look for lipid-genetic interaction because APOE is a lipid-transport gene and the e4 allele is the largest common genetic risk factor for late-onset Alzheimer’s disease. If ordinary clinical statin initiation had a large dementia effect hidden by APOE distribution, the genetic subcohort would be one place for the estimate to move. It did not move enough to change the interpretation.
Why Older Observational Studies Looked Protective
The older literature often made statins look more exciting. Olmastroni et al. pooled 46 observational studies and found statin use associated with a 20% lower dementia risk and a 32% lower Alzheimer’s disease risk.3 That is the kind of number that makes an easy prevention narrative: take a widely used cardiovascular drug, lower LDL, reduce dementia.
The problem is not that the biology is silly. Midlife vascular risk, diabetes, stroke, hypertension, and lipid metabolism all belong in the dementia-risk map.2 The problem is that observational statin use is a badly confounded exposure. People who start and continue preventive medication tend to have different health-care access, clinician contact, adherence patterns, income, education, smoking rates, exercise habits, and baseline cardiovascular risk than people who do not.
Power et al. made this point in 2015: randomized trials did not support starting statins in late life for short-term cognitive protection, while observational studies were vulnerable to bias, reverse causation, and inconsistent exposure definitions.4
The study by Zimmerman et al. is essentially a large-scale answer to that methodological complaint. It preserves the real-world sample size and long follow-up of observational data, but shapes the analysis around a hypothetical trial.
Statin Initiation Looks Null; Sustained Use Is Harder to Prove
The Kaiser study is not the first statin-dementia target-trial emulation, but it is much larger. Caniglia et al. used Rotterdam Study data to emulate statin initiation and sustained statin use in 6,373 individuals.
Statin initiation alone produced a 10-year dementia risk difference of −0.1% (95% CI −2.3% to 1.8%). Sustained use produced a more protective-looking estimate, −2.2% (95% CI −5.2% to 1.6%), but with wide uncertainty and residual-confounding concerns.5
The new Kaiser analysis lands in the same conceptual zone: initiation itself is not a dementia-prevention signal. If long-term adherence to statins protects a subgroup through vascular pathways, this design is not the right way to prove it. But it is strong evidence against a large harmful effect of ordinary statin initiation on long-term dementia diagnosis.
That distinction is not wordplay. An initiation analysis asks whether the clinical act of starting a statin shifts future dementia incidence. A per-protocol long-term exposure analysis asks whether actually staying on statins for years changes risk. The first question is less vulnerable to adherence bias; the second is closer to the biological exposure but easier to confound.
Cognitive Trials Do Not Show Statin Memory Harm
The dementia-prevention case remains unproven, but the cognitive-harm fear is weaker than popular discussion implies. In the Sydney Memory and Aging Study, Samaras et al. followed 1,037 community-dwelling adults aged 70–90 and found statin use was not associated with faster decline in memory, global cognition, or brain volume over follow-up.6
Randomized trials in older or cognitively vulnerable groups have generally not shown a clear cognitive benefit either. PROSPER found pravastatin did not meaningfully change cognitive-function decline in older adults at vascular risk.8 LEADe tested atorvastatin in mild to moderate Alzheimer’s disease and did not establish a treatment effect on Alzheimer’s progression.7
There is also the acute-memory-complaint literature. Strom et al. found a short-term association between new statin exposure and acute memory-loss diagnosis, but the same pattern also appeared with nonstatin lipid-lowering drugs, pointing toward detection bias rather than a statin-specific neurotoxic effect.9 That fits the first-year spike in the Kaiser study: new medications bring patients into medical view.
Limitations of the Kaiser Target-Trial Emulation
Initiation is not perfect exposure. The study estimates an intent-to-treat effect of starting statins, not the effect of uninterrupted high-adherence statin therapy for 20 years. Many initiators stopped or had gaps, and some noninitiators later started statins.1
Statin type changed over time. Initial prescriptions from 2001 to 2010 were dominated by lovastatin and simvastatin because of the Kaiser formulary. The study cannot cleanly answer whether rosuvastatin, atorvastatin, lipophilic statins, hydrophilic statins, or high-intensity treatment differ for dementia risk.
Dementia subtype coding is noisy. AD/ADRD diagnoses came from routine clinical care, often in primary care rather than specialist dementia clinics. Mixed pathology is common in older adults, and clinical subtype labels do not always match autopsy findings.1
Residual confounding remains possible. Target-trial emulation improves observational inference; it does not create randomization. The strength of the paper is that the main long-term estimate is so close to null that a large ordinary statin-initiation effect becomes hard to defend.
Statins vs. Dementia: How to Interpret This Clinically
For cardiovascular prevention: the decision is unchanged. Statins prevent myocardial infarction, ischemic stroke, and vascular events in the populations for whom they are indicated.
For dementia prevention: do not start a statin mainly because it might protect the brain. The best target-trial-style evidence here does not show a long-term prevention signal after year 1.
For dementia fear: do not avoid an indicated statin because of the idea that statins quietly cause Alzheimer’s disease. The first-year diagnosis bump is more consistent with increased medical observation than with a drug-caused dementia process.
For patient conversations: the clearest wording is that statins may create a short-term bump in dementia diagnoses because starting a medication often coincides with more medical attention. Over the long run, in this large Kaiser analysis, they did not meaningfully increase or decrease dementia incidence after the first year.
The literature has spent years oscillating between “statins protect the brain” and “statins hurt memory.” Current evidence supports a narrower conclusion: treat the heart and blood vessels for the reasons already established, and do not borrow more certainty from the dementia literature than it has earned.
Questions About Statins and Dementia
Do statins prevent dementia?
Not on current evidence. Observational meta-analyses report lower dementia risk among statin users, but the best target-trial emulation to date found no long-term reduction after year 1: HR 1.00 for AD/ADRD.1,3
Do statins cause dementia?
The Kaiser target-trial data argue against a meaningful long-term hazard. The first-year diagnosis spike is better explained by increased medical observation than by dementia biology.1
What about people with APOE-e4?
Adjustment for APOE-e4 in the genetic subcohort did not materially change the result. The after-year-1 AD/ADRD HR was 0.97 (95% CI 0.91–1.07), which is compatible with no clear effect.1
Could some statins be better or worse for cognition?
Possibly, but this paper cannot answer that cleanly. Most initiations in the study period involved lovastatin or simvastatin, and many people switched over time. Drug-specific dementia claims need better designs than broad statin-user comparisons.
Should someone stop a statin because of memory concerns?
Not based on dementia fear alone. New or abrupt cognitive symptoms deserve evaluation, medication review, and a search for reversible causes, but the long-term population evidence does not support stopping indicated statin therapy to prevent dementia.
References
- Statin Initiation and Dementia Incidence in a Large Health Care System From 1997 to 2020: A Target Trial Emulation Study. Zimmerman SC, Choi M, Jiang C, et al. Neurology. 2025;105:e213855. doi:10.1212/WNL.0000000000213855
- Dementia prevention, intervention, and care: 2024 report of the Lancet standing Commission. Livingston G, Huntley J, Liu KY, et al. Lancet. 2024;404(10452):572–628. doi:10.1016/S0140-6736(24)01296-0
- Statin use and risk of dementia or Alzheimer’s disease: a systematic review and meta-analysis of observational studies. Olmastroni E, Molari G, De Beni N, et al. European Journal of Preventive Cardiology. 2022;29(5):804–814. doi:10.1093/eurjpc/zwab208
- Statins, cognition, and dementia-systematic review and methodological commentary. Power MC, Weuve J, Sharrett AR, Blacker D, Gottesman RF. Nature Reviews Neurology. 2015;11(4):220–229. doi:10.1038/nrneurol.2015.35
- Emulating a target trial of statin use and risk of dementia using cohort data. Caniglia EC, Rojas-Saunero LP, Hilal S, et al. Neurology. 2020;95(10):e1322–e1332. doi:10.1212/WNL.0000000000010433
- Effects of statins on memory, cognition, and brain volume in the elderly. Samaras K, Makkar SR, Crawford JD, et al. Journal of the American College of Cardiology. 2019;74(21):2554–2568. doi:10.1016/j.jacc.2019.09.041
- Randomized controlled trial of atorvastatin in mild to moderate Alzheimer’s disease: LEADe. Feldman HH, Doody RS, Kivipelto M, et al. Neurology. 2010;74(12):956–964. doi:10.1212/WNL.0b013e3181d6476a
- Pravastatin and cognitive function in the elderly: results of the PROSPER study. Trompet S, van Vliet P, de Craen AJM, et al. Journal of Neurology. 2010;257(1):85–90. doi:10.1007/s00415-009-5271-7
- Statin therapy and risk of acute memory impairment. Strom BL, Schinnar R, Karlawish J, Hennessy S, Teal V, Bilker WB. JAMA Internal Medicine. 2015;175(8):1399–1405. doi:10.1001/jamainternmed.2015.2092