
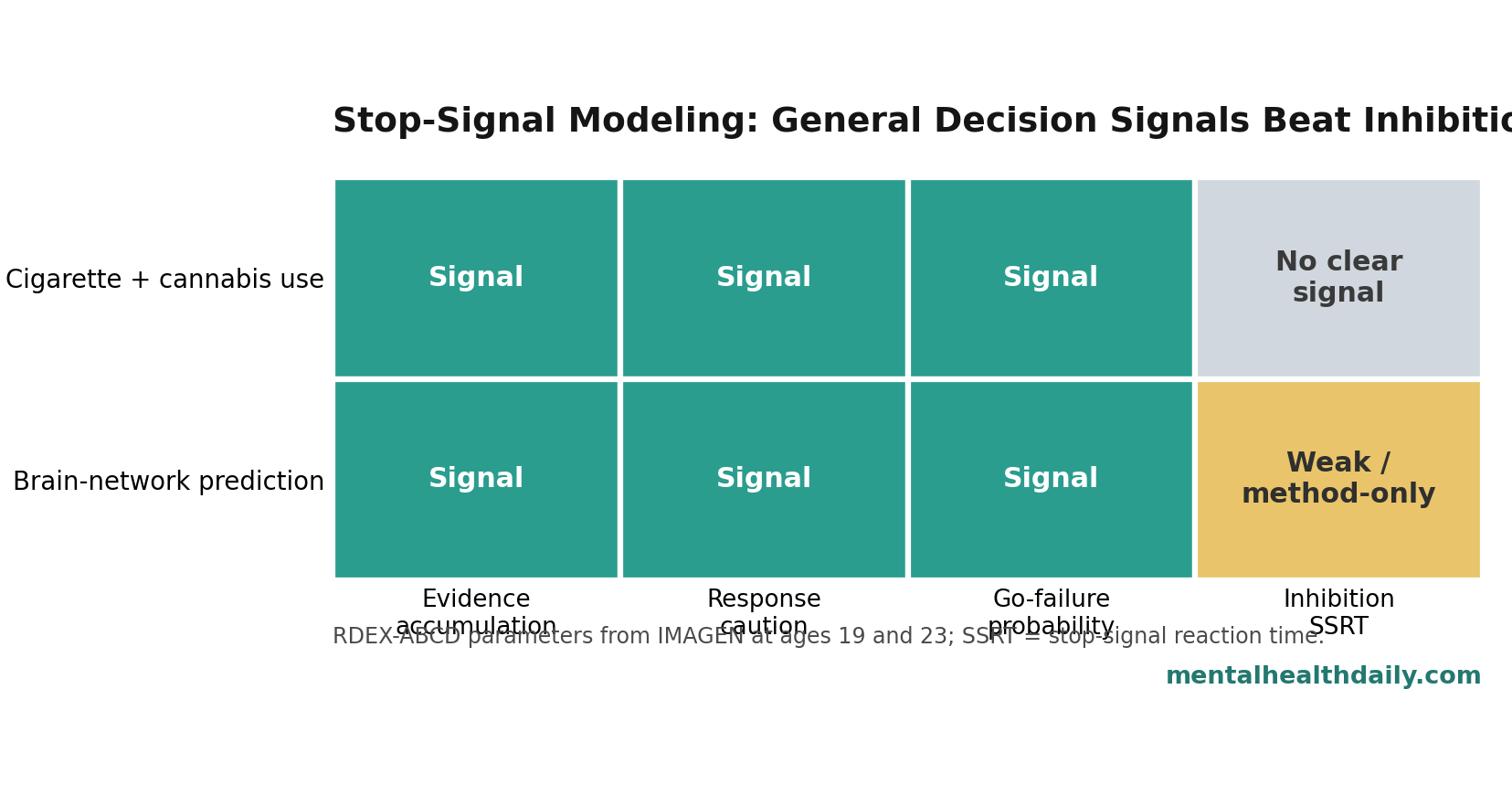
A 2026 IMAGEN stop-signal task analysis found that evidence accumulation, response caution, and go-failure probability predicted cigarette-plus-cannabis use at ages 19 and 23, while inhibition parameters showed no apparent substance-use association.1 The calibrated reading is direct: conventional “poor inhibition” language may be too crude when the cigarette-plus-cannabis signal sits in general decision-making efficiency instead.
Research Highlights
- Decision signals beat inhibition: In 1,256 age-19 and 1,089 age-23 IMAGEN participants, evidence accumulation, response threshold, and go-failure probability predicted cigarette-plus-cannabis use, while inhibition parameters did not.1
- The prediction was specific: Elastic Net models beat random-label permutation for cigarette-plus-cannabis use at ages 19 and 23 (P < 0.001), but no model parameter significantly predicted alcohol or other-drug factors.1
- Evidence accumulation stood out: Brain networks predicted evidence-accumulation efficiency at r = 0.37 at age 19 and r = 0.33 at age 23, both P < 0.01.1
- Conventional SSRT looked weaker: At age 23, network prediction was stronger for RDEX-derived SSRT than integration-method SSRT (r = 0.17 vs. r = 0.07; P = 0.019), but neither inhibition network correlated with cigarette-plus-cannabis use.1
- Small effects are not automatically noise: Large neuroimaging studies often find modest but more reproducible associations, and the authors explicitly framed these effects as population-level risk signals rather than clinical diagnostics.7
Stop-signal tasks ask participants to make fast button responses on ordinary “go” trials and withhold the response when an unpredictable stop cue appears. The usual headline measure is stop-signal reaction time (SSRT), a latent estimate of how quickly a person can cancel an action that is already being prepared.2
That sounds like a clean inhibition test, but task performance also depends on attention, response caution, sensory processing, and how efficiently a person accumulates evidence before choosing. Weng et al. used a computational model to separate those moving parts instead of treating SSRT as the whole story.1
IMAGEN Data Tested Stop-Signal Modeling at Ages 19 and 23
The researchers analyzed the IMAGEN cohort, a large European longitudinal neuroimaging study that followed community-recruited youth into young adulthood. Age-14 stop-signal data were excluded because the task program did not record responses needed for this modeling approach. The final model-estimation samples were 1,256 participants at age 19 and 1,089 participants at age 23.1
For fMRI prediction, the study excluded participants with excessive head motion, leaving 1,202 participants at age 19 and 1,045 at age 23. Substance use came from Timeline Followback interviews, which ask about alcohol, drug, and smoking behavior over the previous 30 days. Factor analysis grouped the substance measures into alcohol, cigarette-plus-cannabis, and other-drug factors.1
RDEX-ABCD modeling means Racing Diffusion Ex-Gaussian modeling adapted for the Adolescent Brain Cognitive Development stop-signal task. In plain English, the model treats task behavior as a race between processes that gather evidence for a go response and processes that describe stopping time. It estimates several latent ingredients:
- Evidence accumulation efficiency: how well the person gathers goal-relevant evidence for the correct response instead of the wrong response.
- Decision threshold: how much evidence the person requires before responding; lower values mean less response caution.
- Go-failure probability: the chance of missing or failing to respond to a go signal, which can reflect attention lapses.
- SSRT: the conventional latent stopping-speed estimate, either from the RDEX model or the standard integration method.
The task had 300 go trials and 60 stop trials. That imbalance becomes important later: go-process estimates are built from more observations, while stopping estimates rely on a smaller slice of behavior.
Cigarette-Plus-Cannabis Use Tracked General Decision Parameters
Weng et al. used Elastic Net regression, a machine-learning method that combines lasso and ridge penalties so a model can select stable predictors without letting correlated variables dominate too easily. The predictors were the RDEX-ABCD parameters plus age, sex, and site; the outcomes were the substance-use factor scores.1
The result was not a broad “substance use” finding. It was specific to the cigarette-plus-cannabis factor. Model performance for cigarette-plus-cannabis use was significantly better than random-label permutation at ages 19 and 23 (P < 0.001). No RDEX-ABCD parameter significantly predicted alcohol or other-drug use at either age.1
The top predictors were general decision-process parameters, not stopping parameters:
- Age 19: go-failure probability (β = 0.105), matching-choice evidence accumulation (β = −0.071), and decision threshold (β = −0.055) were the top feature weights.
- Age 23: matching-choice evidence accumulation (β = −0.119), go-failure probability (β = 0.061), and decision threshold (β = −0.023) were the top feature weights.
- Stability: those 3 predictors were selected in all 100 Elastic Net iterations at both ages.
Lower matching-choice evidence accumulation and lower decision threshold tracked higher cigarette-plus-cannabis use. Higher go-failure probability also tracked higher use. In reader language: the signal was noisier decision-making, lower response caution, and more lapses on ordinary go trials, not a clean stopping-speed deficit.
Brain Networks Supported Evidence Accumulation More Consistently Than Inhibition
The researchers also used connectome-based predictive modeling, a method that predicts individual behavior from whole-brain functional connectivity patterns. Functional connections were selected in training folds, then tested by cross-validation to see whether network strength predicted each model parameter.1
Combined brain networks significantly predicted evidence accumulation, decision threshold, and go-failure probability at both ages. Evidence accumulation had the strongest network prediction among the go-process parameters: r = 0.37 at age 19 and r = 0.33 at age 23, both P < 0.01. Go-failure probability was also stable at r = 0.28 at both ages. Decision threshold was smaller but still significant at r = 0.10 and r = 0.14.1
Network strength also showed some stability over time. Evidence-accumulation network strength correlated from age 19 to 23 at R = 0.60 (P = 3.02E-79). Decision-threshold network strength correlated at R = 0.30, go-failure probability at R = 0.25, RDEX-derived SSRT at R = 0.42, and integration-method SSRT at R = 0.25.1
Substance-use correlations narrowed the interpretation. At age 19, only the go-failure network correlated with cigarette-plus-cannabis use (rho = 0.07, P = 0.016). At age 23, evidence-accumulation and decision-threshold networks correlated with cigarette-plus-cannabis use (rho = −0.12 and rho = −0.11), while go-failure probability was borderline (rho = 0.06, P = 0.058). SSRT networks did not significantly correlate with cigarette-plus-cannabis use.1
Conventional Inhibitory-Control Framing Looks Overweighted
The stop-signal task is often introduced as an inhibitory-control task. That label is not wrong, but Weng et al. showed why it can become misleading when used as a one-word explanation for substance-use vulnerability.
Prior stop-signal guidance has already emphasized careful interpretation of SSRT and task design.2 Computational case-control work has also suggested that apparent inhibition deficits in ADHD and schizophrenia can reflect broader attentional or decision-processing problems rather than a pure stopping impairment.1
The substance-use result fits that larger pattern. SSRT was not useless as a modeling object. RDEX-derived SSRT had some brain-network predictability, and at age 23 it outperformed integration-method SSRT for network prediction (r = 0.17 vs. r = 0.07; P = 0.019). The problem is narrower: SSRT did not carry the cigarette-plus-cannabis association that the go-process parameters carried.
Fascher et al.’s 2024 meta-analysis reached a compatible caution from the substance-use-disorder side: neural evidence for response inhibition as a widely used construct was weak.6 Weng et al. added a large longitudinal modeling test in young adults, pointing toward evidence accumulation and response caution as more useful signals.
Evidence Accumulation May Be a Transdiagnostic Vulnerability Signal
Evidence accumulation is the process of gathering enough information to make a decision. In a lab task, it can be estimated from reaction time and accuracy patterns. In real life, the same broad mechanism maps onto how efficiently a person filters signal from noise before choosing an action.
That is why evidence accumulation has become attractive in computational psychiatry. Weigard et al. previously argued that task-general evidence accumulation may function as a neurocognitive trait relevant across clinical conditions.4 In a prospective substance-use study, lower evidence accumulation and related error-processing activity predicted greater use during emerging adulthood.3
Weng et al. did not prove that evidence accumulation causes cannabis or cigarette use. The safer interpretation is that inefficient decision evidence, low response caution, and attention lapses may mark a broader vulnerability system. That system can influence real-world choices where rewards are immediate, risks are delayed, and social context is noisy.
Clinical implication: the finding pushes assessment away from a single “inhibition problem” label. For prevention or treatment research, it may be more useful to ask whether a person has noisy evidence accumulation, low response caution, attentional lapses, or some combination of those processes.
Effect Sizes Were Modest but Not Disposable
Large neuroimaging and individual-difference studies often find small associations. Marek et al. argued that reproducible brain-wide association studies require thousands of individuals, partly because plausible brain-behavior correlations are usually modest.7 Weng et al. used more than 1,000 participants at each wave, so the small coefficients should not be dismissed automatically as underpowered noise.
Small effects also fit the outcome. Cigarette and cannabis use in young adults is shaped by availability, peers, family history, stress, impulsivity, economics, policy, advertising, and psychiatric symptoms. A single stop-signal model parameter should not be expected to classify individuals.
McCabe et al.’s longitudinal work adds the clinical bridge: higher substance-use disorder symptom severity at age 18 predicted adult prescription-drug misuse and later substance-use disorder outcomes.8 Weng et al. studied recent use factors rather than diagnosed disorder, but frequent use in late adolescence and early adulthood can still mark risk-relevant trajectories.
Limitations of This IMAGEN Stop-Signal Analysis
Several limits keep the article’s result in its proper lane.
- Outcome scope: the reliable prediction involved cigarette-plus-cannabis use, not alcohol or other-drug factors.
- Clinical scope: the study measured recent use, not diagnosed substance-use disorder, withdrawal, impairment, or treatment response.
- Causal scope: computational parameters and brain networks predicted or correlated with use. The design did not show that changing evidence accumulation would reduce use.
- Modeling scope: RDEX-ABCD is richer than a simple SSRT estimate, but it remains a model with assumptions about response-time distributions, evidence accumulation, and stop-process timing.
- Generalizability: IMAGEN is a valuable longitudinal cohort, but the findings still need replication in clinically diagnosed addiction samples and more diverse settings.
Those limits do not erase the main calibration. In this large young-adult sample, the substance-use signal was stronger for general decision-making mechanisms than for the conventional inhibition measure.
Questions About Stop-Signal Tasks and Substance Use
Did this study show that poor inhibition does not matter for addiction?
No. It showed that conventional inhibition parameters from this stop-signal modeling analysis did not predict cigarette-plus-cannabis use, while evidence accumulation, response caution, and go-failure probability did. Inhibition may still matter in other tasks, populations, or clinical addiction samples.
Why combine cigarette and cannabis use?
Factor analysis of the Timeline Followback items grouped cigarette and cannabis measures together. The model’s significant prediction applied to that combined factor, not to every substance category.
Does a negative beta for evidence accumulation mean evidence accumulation is harmful?
No. The negative coefficient means lower matching-choice evidence accumulation tracked higher cigarette-plus-cannabis use in the coded model. Lower evidence-accumulation efficiency is the risk marker in this coding, not harm from evidence accumulation itself.
Can this task diagnose future addiction risk?
No. The associations were modest and population-level. The task may help research on vulnerability mechanisms, but it is not a standalone clinical screening test.
What should future studies test next?
Replication should use clinical substance-use-disorder samples, longer follow-up, and interventions that test whether decision-making mechanisms can change. The most useful next step is not another simple inhibition label; it is a mechanism-specific test of evidence accumulation, response caution, and attention lapses.
References
- Weng Y, Boyle R, Lee CT, et al. Model-based analysis of stop-signal data reveals robust neural and clinical correlates of evidence accumulation but not inhibition. Neuropsychopharmacology. 2026. doi:10.1038/s41386-026-02401-6
- Verbruggen F, Aron AR, Band GPH, et al. A consensus guide to capturing the ability to inhibit actions and impulsive behaviors in the stop-signal task. eLife. 2019;8:e46323. doi:10.7554/elife.46323
- Weigard AS, Brislin SJ, Cope LM, et al. Evidence accumulation and associated error-related brain activity as computationally-informed prospective predictors of substance use in emerging adulthood. Psychopharmacology. 2021;238:2629–2644. PubMed
- Weigard A, Sripada C. Task-general efficiency of evidence accumulation as a computationally-defined neurocognitive trait: implications for clinical neuroscience. Biological Psychiatry Global Open Science. 2021;1:5–15. doi:10.1016/j.bpsgos.2021.04.001
- Weng Y, Kruschwitz J, Rueda-Delgado LM, et al. A robust brain network for sustained attention from adolescence to adulthood that predicts later substance use. eLife. 2024;13:RP97150. PubMed
- Fascher M, Nowaczynski S, Spindler C, Strobach T, Muehlhan M. Neural underpinnings of response inhibition in substance use disorders: weak meta-analytic evidence for a widely used construct. Psychopharmacology. 2024;241:1–17. PubMed
- Marek S, Tervo-Clemmens B, Calabro FJ, et al. Reproducible brain-wide association studies require thousands of individuals. Nature. 2022;603:654–660. doi:10.1038/s41586-022-04492-9
- McCabe SE, Schulenberg JE, Schepis TS, McCabe VV, Veliz PT. Longitudinal analysis of substance use disorder symptom severity at age 18 years and substance use disorder in adulthood. JAMA Network Open. 2022;5:e225324. doi:10.1001/jamanetworkopen.2022.5324