A 2026 PRISMA systematic review by Cavallo et al. in Cognitive, Affective, & Behavioral Neuroscience aggregates 43 neuroimaging studies of social cognition in adults with stroke or traumatic brain injury and finds the same handful of regions implicated again and again: the insula, cingulate cortex, middle frontal gyrus, and corpus callosum.1
Research Highlights
- Stroke/TBI social-cognition map: 43 neuroimaging studies covered 4 domains after acquired brain injury.1
- Four-region overlap: insula, middle frontal gyrus, cingulate cortex, and corpus callosum recurred across domains.1
- Insula repeat signal: the insula appeared in all 4 domains and was reported bilaterally.1
- Common deficits: emotion recognition is impaired in roughly 46–49% of stroke survivors and 13–39% of adults with TBI.1,6
- Convergent, not settled: the 43-study review could not run a quantitative meta-analysis because tasks and imaging methods varied.1
The evidence is convergent but heterogeneous. The review is a narrative synthesis — not a coordinate-based meta-analysis — pooling small samples across heterogeneous tasks, two very different injury mechanisms, and a 21-year publication window.
The convergent regions match what the healthy social-brain literature already pointed to.2,3
These deficits aren’t niche. Emotion recognition is impaired in roughly 46–49% of stroke survivors and 13–39% of adults with TBI; reduced emotional empathy is reported in around 61% of TBI samples.1,6 They often persist after general cognition recovers and predict social isolation, employment loss, and caregiver strain better than memory or attention scores do.7
Cavallo 2026: 43 Studies Across Stroke and TBI, Four Social-Cognition Domains
The review followed PRISMA 2020 with a PROSPERO-registered protocol (CRD42024528643). Two database sweeps (March 2024, November 2025) returned 2,896 records; 1,246 went to full-text review; 43 made the final cut. Inclusion was restricted to peer-reviewed primary studies of adults with stroke or TBI that combined a validated social-cognition assessment with structural or functional neuroimaging.1
The four domains carved out by Cavallo are now the standard taxonomy in the field:
- Emotion recognition. Identifying affect from faces, voices, or body posture — the lower-level, perceptually driven component.
- Theory of Mind. Inferring others’ beliefs, intentions, or mental states. Subdivided into cognitive (about thoughts) and affective (about emotions) variants.
- Perspective taking. Egocentric vs. allocentric frames; understanding what another agent visually or spatially experiences.
- Empathy. Sharing or resonating with another’s emotional experience — cognitive and affective components.
Stroke studies skewed toward voxel-based lesion-symptom mapping (VLSM) on structural MRI; TBI studies leaned more on functional MRI and diffusion-weighted imaging because the damage is diffuse rather than focal. That methodological asymmetry matters when reading the convergent-anatomy claim — stroke and TBI literature are looking at the brain through different lenses, and any overlap they produce has to survive that.1
Insula, Middle Frontal Gyrus, Cingulate, Corpus Callosum: The Convergent Four
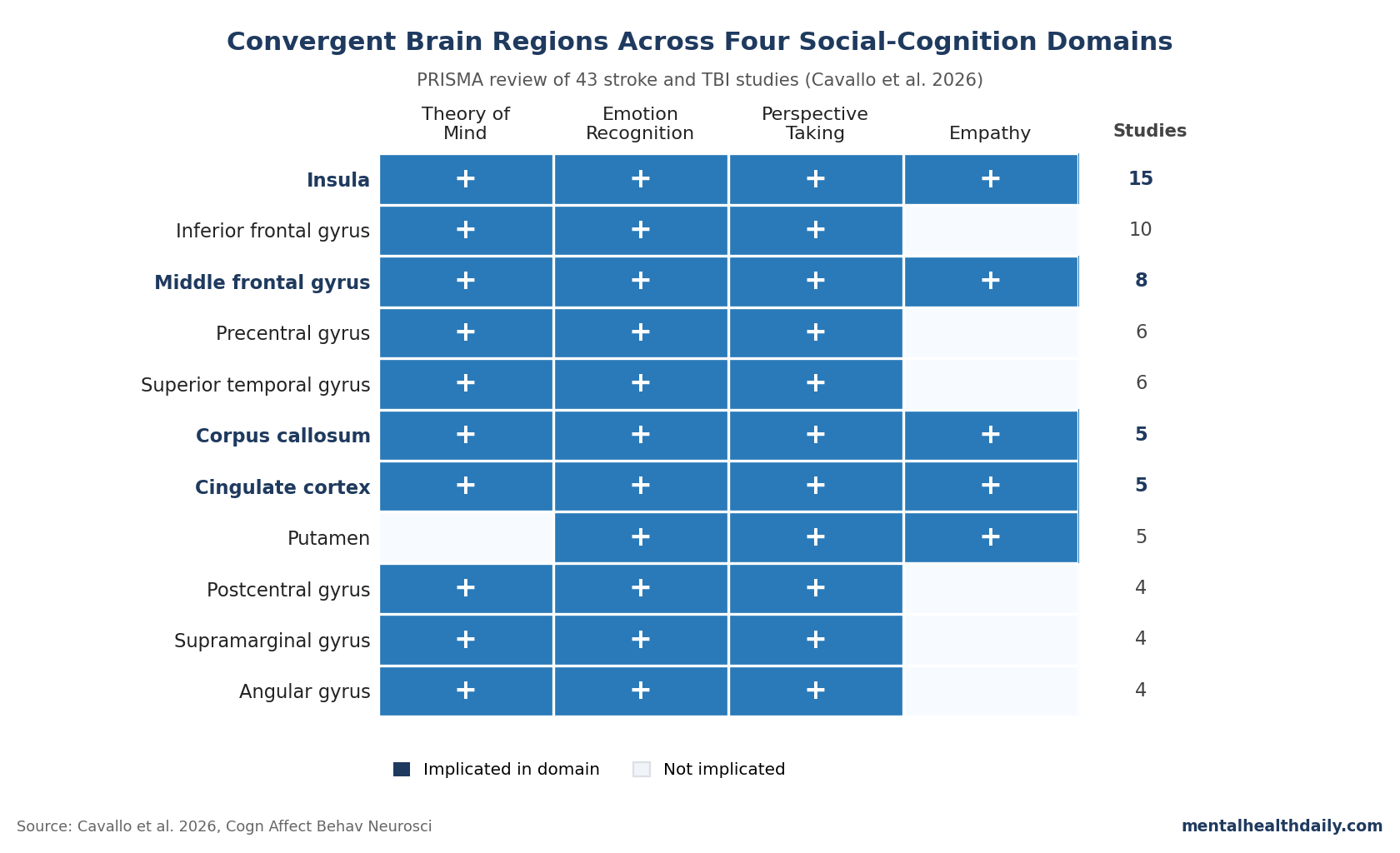
Across domains, four regions were implicated by at least three of the four social-cognition constructs:
- Insula — involved across all four domains, in 15 of 43 studies. Bilateral. The most consistently implicated single structure.
- Middle frontal gyrus — involved across all four domains, 8 studies. Right-lateralized in stroke; bilateral in TBI.
- Corpus callosum — flagged across all four domains, 5 studies. Genu and splenium tracked social inference in TBI specifically.8
- Cingulate cortex — 5 studies, anterior and posterior subregions, with variable lateralization.
A second tier — inferior frontal gyrus, precentral and postcentral gyri, supramarginal gyrus, angular gyrus, superior temporal gyrus, putamen — appeared in three of the four constructs.1
The insula finding is the most anatomically coherent. Cavallo lines it up with healthy-brain work positioning the anterior insula as a hub for interoceptive awareness, salience detection, and emotional simulation — functions that route directly into emotion recognition, empathic resonance, and affective Theory of Mind.9,10
The middle frontal gyrus story is more about cognitive control than social processing per se. It mediates inhibition, conflict resolution, and goal-directed behavior — capacities recruited whenever a social inference requires holding ambiguity or suppressing a default attribution.11 The corpus callosum implication in TBI fits a long-standing observation that diffuse axonal injury disrupts interhemispheric integration in ways focal stroke usually does not.8
Why ToM and Empathy Findings Diverge Across Stroke and TBI
The convergent-anatomy story does not extend cleanly to every domain. Empathy in particular splits along injury type:
Stroke. Empathy deficits track white matter pathology — fornix, uncinate fasciculus, sagittal stratum, body of the corpus callosum — and right-hemisphere cortical atrophy in cingulate and posterior regions. Right uncinate damage has been specifically linked to affective empathy reduction.1
TBI. Empathy deficits track cortical damage in ventrolateral prefrontal cortex, posterior temporal lobes, and bilateral insula. Self-report empathy correlates with insular damage on either side.1
Cavallo notes that no single cortical or subcortical region emerged as a consistent empathy correlate across both populations. The two literatures converge only at the level of right-hemisphere prevalence and insular involvement; below that, the lesion patterns diverge. The same is true for Theory of Mind: stroke ToM deficits sit in focal frontal-parietal cortical lesions, whereas TBI ToM deficits combine cortical damage with diffuse white-matter disconnection.1,5
The takeaway isn’t that the convergence claim is wrong — it’s that the convergence is at a coarser anatomical grain than the popular framing tends to imply. “The insula is the social-cognition hub” is broadly defensible. “The right anterior insula causes affective empathy” is a stronger claim than 7 stroke and 3 TBI studies, with very different methods, can support on their own.
Limitations of Pooling Stroke and TBI in One Review
Three caveats deserve weight:
- No quantitative synthesis. The authors planned a meta-analysis and abandoned it because the included studies did not report standardized spatial coordinates (MNI or Talairach) or comparable effect sizes. The synthesis is narrative, following SWiM guidelines, with region tallies rather than coordinate-based activation likelihood estimation. Convergence claims that would require an ALE meta-analysis to confirm formally remain inferential.1,12
- Stroke and TBI are mechanistically different injuries. Stroke produces focal vascular lesions; TBI produces diffuse axonal injury, contusions, and secondary inflammation. Pooling them at the level of “acquired brain injury” is convenient but obscures whether shared regional findings reflect shared social-cognition substrates or methodological artifacts of how each literature reports lesions. Cavallo flags this and explicitly cautions that any neural convergence reflects shared lesion- or network-level associations, not etiological equivalence.1
- Severity, time-since-injury, and task heterogeneity were not systematically extracted. Severity indices were inconsistently reported, time post-onset ranged from acute days to chronic decades, and tasks ranged from facial-emotion photographs to Theory-of-Mind story batteries to self-report empathy questionnaires. Each of these variables likely modulates both the deficit and its anatomical signature, and pooling across them is a real source of noise.1,4
The included samples are also small. Most individual studies run 20–40 patients. VLSM at those sizes can detect strong lesion-deficit associations but is underpowered to localize subcortical structures or fine cortical subdivisions cleanly.13 The review’s value is convergence across many small studies, not any single study’s causal claim.
Social-Cognition Rehabilitation Needs Domain-Specific Targets
The clinical pull from Cavallo isn’t a new biomarker. It’s a stronger case for what social-cognition rehabilitation programs already increasingly try to do: assess the four domains separately, and don’t assume a patient who recognizes facial anger fluently also reads sarcasm or takes a partner’s perspective.14
Four practical implications follow:
- Comprehensive assessment beats screening. The four domains dissociate neuroanatomically and behaviorally; a focal lesion can knock out one and leave the others intact.1,15
- Right-hemisphere stroke survivors are higher-prior for perspective-taking and empathy deficits than a standard cognitive screen will catch.1
- Diffuse-injury TBI patients with intact cortex on MRI may still have empathy and ToM deficits mediated by white-matter disconnection. Diffusion tensor imaging of the corpus callosum and uncinate fasciculus is more informative for this population.8
- Severity scores don’t closely predict the social-cognition picture. Standard rehabilitation triage can miss high-functioning patients with disabling social deficits.4,5
None of this is new advice; the McDonald rehabilitation work and the Henry meta-analytic synthesis already pointed there.14,4 Cavallo’s contribution is to harden the anatomical justification for keeping the four domains separate in routine assessment.
Region Tallies Do Not Prove Causal Social-Brain Hubs
The review surfaces several open questions it cannot resolve.
Causality vs. correlation in lesion mapping. Region-X-is-implicated-in-domain-Y is a correlational claim from observational lesion data, not a causal one. The healthy social-brain literature offers convergent functional evidence, but a region’s recurrent appearance across small lesion studies doesn’t formally demonstrate that the region is necessary for the function — only that damage including that region tends to co-occur with the deficit.13
Network-level vs. region-level inference. Cavallo’s convergent regions sit inside the canonical mentalizing network (medial prefrontal cortex, temporoparietal junction, posterior cingulate, superior temporal sulcus, temporal poles) and salience network (anterior insula, anterior cingulate). The next-generation question is whether brain-injury social-cognition deficits are best framed as network-level disconnection rather than focal regional damage — a framing the included studies generally lack the connectomic data to test.3,10
Treatment-mechanism translation. If the insula is doing this much social-cognitive work, does targeting insular function — via interoceptive training, transcranial stimulation, or cognitive remediation — rehabilitate social cognition more effectively than untargeted approaches? The mechanism finding licenses the hypothesis; the rehabilitation literature has not yet tested it cleanly.
What Patients and Caregivers Ask About Social Cognition Recovery
Are social-cognition deficits common after stroke and TBI?
Yes. Earlier prevalence work cited by Cavallo finds emotion-recognition deficits in roughly 46–49% of stroke survivors and 13–39% of adults with TBI, with reduced emotional empathy in around 61% of TBI samples. The deficits often persist after general cognition recovers.1,6
Which brain region is most consistently linked to social-cognition deficits?
The insula. It was implicated across all four social-cognition domains and appeared in 15 of the 43 included studies, with bilateral involvement. This converges with healthy-brain work positioning the anterior insula as a hub for interoceptive awareness and emotional simulation.1,9
Is this a meta-analysis?
No. Cavallo et al. planned a meta-analysis but abandoned it because the included studies did not report standardized brain coordinates or comparable effect sizes. The synthesis is narrative, following SWiM guidelines. A coordinate-based activation likelihood estimation meta-analysis would be the next quantitative step.1,12
Do stroke and TBI affect social cognition the same way?
Partially. Both populations show deficits across all four domains, and both implicate the insula, middle frontal gyrus, cingulate, and corpus callosum. But TBI deficits more often involve diffuse white-matter disconnection, while stroke deficits more often involve focal cortical or subcortical lesions. Empathy in particular shows divergent lesion patterns between the two.1
Does injury severity predict social-cognition deficits?
Not closely. Severity indices were not systematically extracted in the Cavallo review because they were inconsistently reported, but earlier meta-analyses in TBI find that ToM and emotion-recognition deficits do not closely track standard severity measures. High-functioning patients can still have disabling social-cognition deficits.4,5
What should clinicians do differently after this review?
Assess the four domains separately rather than relying on a single screen. Right-hemisphere stroke survivors warrant attention for perspective-taking and empathy. Diffuse-injury TBI patients with intact cortex may still have white-matter-mediated empathy and ToM deficits, which standard cortical imaging will miss.1,14
What would make the neural map more definitive?
A coordinate-based ALE meta-analysis on the subset of studies reporting standardized peaks. Larger single-site VLSM studies (200+ patients) with harmonized batteries. Diffusion connectomic analyses tying domain-specific deficits to white-matter disconnection profiles. Targeted rehabilitation trials testing whether interoceptive or insular-stimulation interventions move social-cognition outcomes.
References
- Neural correlates of social cognition in stroke and traumatic brain injury: a systematic review. Cavallo ND, Giacobbe C, Baiano C, et al. Cognitive, Affective, & Behavioral Neuroscience. 2026. doi:10.3758/s13415-026-01438-w
- The social brain: neural basis of social knowledge. Adolphs R. Annual Review of Psychology. 2009;60:693–716. doi:10.1146/annurev.psych.60.110707.163514
- Mechanisms of social cognition. Frith CD, Frith U. Annual Review of Psychology. 2012;63:287–313. doi:10.1146/annurev-psych-120710-100449
- Meta-analytic review of emotion recognition and theory of mind in moderate to severe traumatic brain injury. Babbage DR, Yim J, Zupan B, et al. Neuropsychology. 2011;25(3):277–285. doi:10.1037/a0021908
- Theory of mind in adults with traumatic brain injury: a meta-analysis. Bivona U, Formisano R, De Laurentiis S, et al. Neuropsychology Review. 2014;24:317–336. doi:10.1007/s11065-014-9266-5
- Inability to empathize following traumatic brain injury. Wood RL, Williams C. Journal of the International Neuropsychological Society. 2008;14(2):289–296. doi:10.1017/S1355617708080326
- A meta-analytic review of social cognitive function following stroke. Adams AG, Schweitzer D, Molenberghs P, Henry JD. Neuroscience & Biobehavioral Reviews. 2019;102:400–416. doi:10.1016/j.neubiorev.2019.03.011
- Adults with traumatic brain injury: three-year postinjury social communication skills and the connectivity of the corpus callosum. McDonald S, Dalton KI, Rushby JA, Landin-Romero R. Brain Injury. 2018;32(13–14):1750–1755. doi:10.1080/02699052.2018.1539248
- Anterior insular cortex and emotional awareness. Gu X, Hof PR, Friston KJ, Fan J. Journal of Comparative Neurology. 2013;521(15):3371–3388. doi:10.1002/cne.23368
- Structure and function of the human insula. Uddin LQ, Nomi JS, Hebert-Seropian B, Ghaziri J, Boucher O. Journal of Clinical Neurophysiology. 2017;34(4):300–306. doi:10.1097/WNP.0000000000000377
- Neural correlates of theory-of-mind reasoning: an activation likelihood estimation meta-analysis. Schurz M, Radua J, Aichhorn M, Richlan F, Perner J. Neuroscience & Biobehavioral Reviews. 2014;42:9–34. doi:10.1016/j.neubiorev.2014.01.009
- Synthesis without meta-analysis (SWiM) in systematic reviews: reporting guideline. Campbell M, McKenzie JE, Sowden A, et al. BMJ. 2020;368:l6890. doi:10.1136/bmj.l6890
- Voxel-based lesion-symptom mapping. Bates E, Wilson SM, Saygin AP, et al. Nature Neuroscience. 2003;6(5):448–450. doi:10.1038/nn1050
- Reliability and validity of The Awareness of Social Inference Test (TASIT): a clinical test of social perception. McDonald S, Flanagan S, Rollins J, Kinch J. Disability and Rehabilitation. 2003;25(11–12):572–579. doi:10.1080/0963828031000137090
- A meta-analytic review of social cognitive function in neurodegenerative disease and acquired brain injury. Henry JD, von Hippel W, Molenberghs P, Lee T, Sachdev PS. Nature Reviews Neurology. 2016;12(1):28–39. doi:10.1038/nrneurol.2015.229