Loneliness is now framed in mainstream coverage as a public-health emergency on par with cardiovascular risk factors. Surkalim and colleagues’ 2022 BMJ analysis estimated that around a quarter of older adults globally experience loneliness, with substantial regional variation,10 and the WHO Commission on Social Connection has formalized the topic as a public-health priority.
The associations between loneliness and bad outcomes are well-documented, but the popular framing flattens substantial uncertainty — about magnitude, about causal direction, and about which mental and cognitive outcomes loneliness most reliably predicts. The 2026 Rodrigues meta-analysis is the largest available synthesis at the loneliness/Alzheimer’s/suicide intersection, and reading its numbers carefully separates what the data show from what the headlines say.
Research Highlights
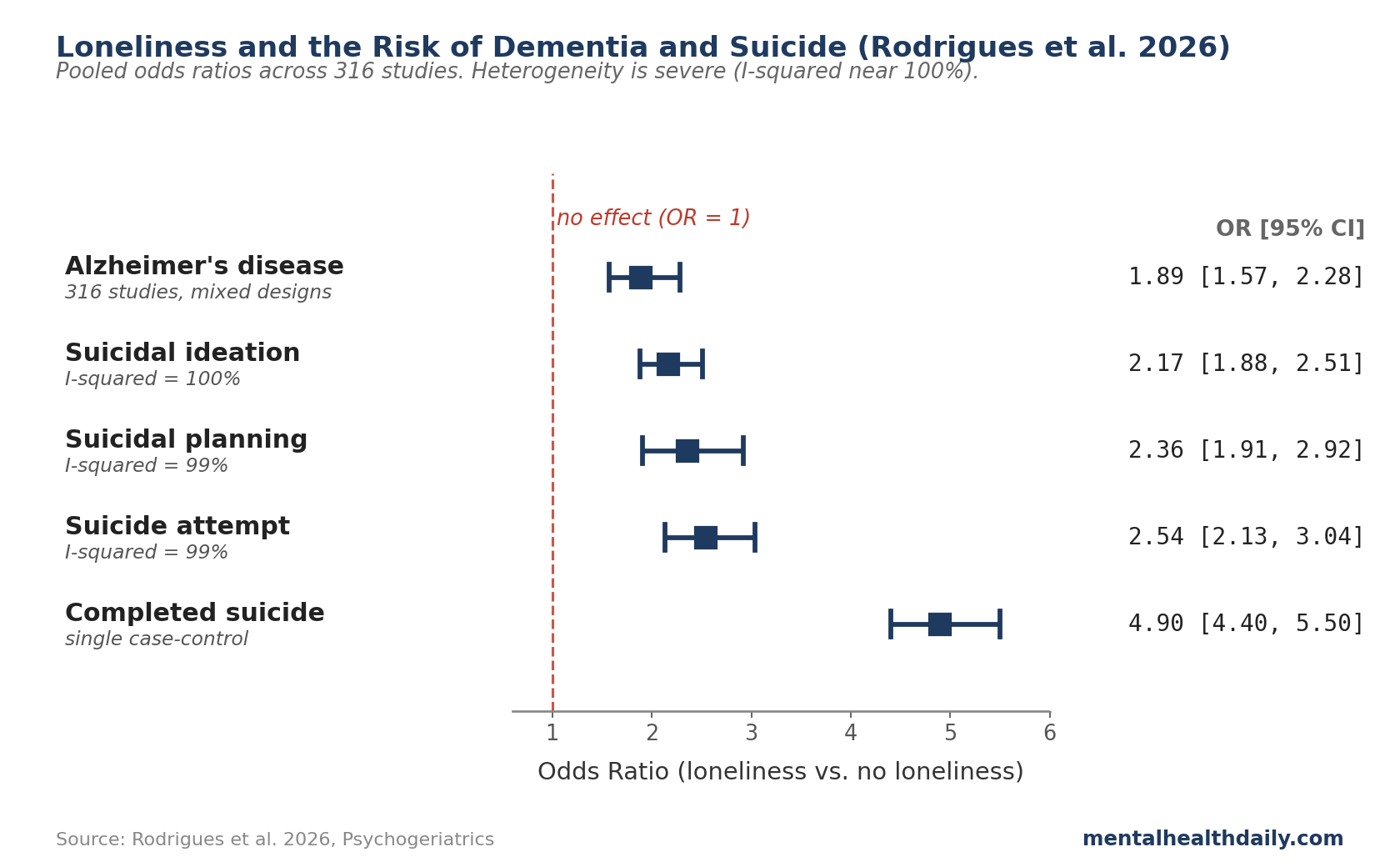
- Loneliness is associated with substantially elevated risk of both Alzheimer’s disease and suicide. The largest synthesis to date (Rodrigues et al. 2026, 316 studies) reports pooled odds ratios of 1.89 for AD, 2.17 for suicidal ideation, 2.36 for suicidal planning, and 2.54 for suicide attempt. The effect on completed suicide in case-control data was substantially larger (OR 4.9).
- Heterogeneity is severe and the data are dominated by cross-sectional designs. I² statistics in the pooled analyses sit near 100%, meaning studies disagree fundamentally on effect magnitude. Most evidence is correlational at a single timepoint — the question of whether loneliness causes AD or AD causes loneliness can’t be answered from cross-sectional data alone.
- Causal evidence exists, but it’s narrower than the headline ORs. Longitudinal cohorts find smaller hazard ratios (1.4 to 2.2 for incident dementia) than cross-sectional pooled estimates. A 2021 Mendelian randomization study, which uses genetic instruments to approximate randomization, found loneliness-associated genes predicted suicide attempt with OR 7.07 — suggestive of causality but with a wide confidence interval and a single instrument.
- Depression mediates a meaningful share of the loneliness-to-bad-outcome path. Across the meta-analysis, depression was the most frequently identified shared correlate connecting loneliness to both AD and suicide. The Van Orden interpersonal model places thwarted belongingness (the social-need analog of loneliness) at the center of suicide risk in older adults.
- The “loneliness kills” framing is directionally correct but quantitatively soft. Loneliness is a documented risk factor that warrants public-health attention. The popular “loneliness is as bad as smoking 15 cigarettes a day” claim, however, comes from a single 2010 meta-analysis estimate that has been overgeneralized far beyond its actual data.
Effect Sizes Across Outcomes in the Rodrigues Synthesis
Rodrigues and colleagues’ 2026 systematic review and meta-analysis in Psychogeriatrics screened 3,578 studies across seven multilingual databases, included 316 in the qualitative review, and pooled effect sizes from eligible studies in two parallel meta-analyses (loneliness-Alzheimer’s and loneliness-suicide), then ran a meta-analytic factor analysis to identify shared correlates.1 The headline odds ratios:
- Alzheimer’s disease: OR 1.89 (95% CI 1.57 to 2.28; p < 0.001).
- Suicidal ideation: OR 2.17 (95% CI 1.88 to 2.51; p < 0.001; I² = 100%).
- Suicidal planning: OR 2.36 (95% CI 1.91 to 2.92; p < 0.001).
- Suicide attempt: OR 2.54 (95% CI 2.13 to 3.04; p < 0.001; I² = 99%).
- Completed suicide (case-control): OR 4.9 (95% CI 4.4 to 5.5; p < 0.001) — from a single case-control study.1
(The odds ratio — OR — is roughly the multiplier on baseline risk. An OR of 2 means people experiencing the exposure have approximately twice the odds of the outcome compared to people not. The 95% confidence interval — CI — is the range the true effect is likely to sit in. I² is heterogeneity: how much trial-to-trial disagreement exists beyond what sampling noise alone would produce, with 100% meaning essentially all variation reflects true differences between studies.)
Two patterns are worth flagging at the outset:
- The risk climbs in steps as the outcome gets more severe. Suicidal ideation (OR 2.17), planning (2.36), attempt (2.54), and completed suicide (4.9) form a ladder where the strongest signal sits at the most severe outcome. That ordering is unusual — rare severe outcomes are usually harder to predict, not easier. The most defensible take: people who die by suicide tend to have had longer, deeper loneliness than people earlier on the suicidal-thinking spectrum.
- The studies disagree wildly on the size of the effect. The heterogeneity score (I²) sits near 100% across the suicide outcomes — meaning the trials don’t agree on how big the loneliness effect actually is. The pooled odds ratio averages across very different study designs (case-control, cohort, cross-sectional, Mendelian) and very different populations (teenagers through the elderly), where the true effect almost certainly varies. The pooled number points the right direction; the exact size can’t be pinned down from the data we have.
Loneliness and Dementia: Causal or Correlational?
The Rodrigues pooled OR of 1.89 for Alzheimer’s is consistent with several earlier longitudinal syntheses. Lara and colleagues’ 2019 systematic review in Ageing Research Reviews, which restricted to prospective cohort designs, reported a hazard ratio of approximately 1.26 (95% CI 1.14 to 1.40) for incident dementia among lonely individuals.2 Sutin and colleagues’ 2018 analysis of the Health and Retirement Study and similar large cohorts produced HRs in the 1.4 to 2.2 range across studies, depending on the loneliness measure and follow-up duration.3
The pattern across study types is telling. Cross-sectional studies (which measure loneliness and cognition at the same moment) produce the biggest numbers, partly because they have a chicken-and-egg problem — early cognitive decline itself makes people more isolated, which inflates the apparent loneliness-to-Alzheimer’s link.
Longitudinal studies (which measure loneliness first, then track who develops dementia later) adjust for starting cognition and produce smaller numbers. Those smaller, forward-looking estimates are the more credible read for whether loneliness actually drives dementia risk.
Several plausible mechanisms have been proposed:
- HPA-axis dysregulation and chronic cortisol elevation. Loneliness sustains low-grade physiological stress — elevated baseline cortisol, blunted diurnal rhythm — which has documented hippocampal effects in chronic-stress models.4,9
- Reduced cognitive reserve from disengagement. Social interaction is itself cognitively demanding; sustained loneliness reduces the regular cognitive workout that builds reserve.
- Inflammation. Lonely individuals show modestly elevated systemic inflammatory markers in some studies, though community-sample data complicate the picture (see the inflammation-and-depression piece for the full calibration).
- Health-behavior pathways. Lonely people exercise less, sleep worse, and have lower medication adherence — each of which independently predicts dementia risk.
None of these has been shown to be the mechanism whose blockade abolishes the loneliness-AD association. Multiple parallel pathways is the most defensible reading.
Loneliness and Suicide: A Stronger Signal With a Worse Evidence Base
The suicide numbers are bigger than the dementia number, but the studies behind them are weaker. The OR of 4.9 for completed suicide comes from a single case-control study, which is the design where researchers start with people who already died and look back at their history.
That design pumps up the apparent effect for two reasons: it oversamples the worst cases by definition, and the loneliness data is reconstructed after the fact by surviving family members. Cohort studies (which start with living people and follow them forward) produce hazard ratios in the 1.4 to 1.6 range — still meaningful, but a fraction of the case-control number.1
The clearest causal-leaning evidence comes from a 2021 Mendelian randomization analysis cited in the Rodrigues review.
Mendelian randomization is a clever workaround for the limits of observational data: it uses genetic variants linked to loneliness as a kind of natural experiment. Because the variants you inherit are essentially randomized at conception, downstream associations between those variants and an outcome approximate what an actual randomized trial would estimate — without needing to run one.
The reported OR of 7.07 (p = 0.05) for suicide attempt suggests loneliness may genuinely cause some suicide risk — but the confidence interval is wide and the p-value is right on the line. Read it as a hint pointing the right way, not as proof.1
Joiner’s interpersonal theory of suicide gives a useful way to make sense of this. The model puts two feelings at the center of suicide risk: thwarted belongingness (in plain terms, feeling like you don’t belong) and perceived burdensomeness (feeling like you’re a weight on the people around you). The third ingredient is the capability to actually act — which can come from past exposure to pain or violence.5
For older adults specifically, Van Orden’s “5 Ds” model lists depression, disconnectedness, debility, decreased mobility, and dependence as the main risk drivers — with disconnectedness (functionally, loneliness) called out as a primary one.6 Both frameworks fit the data; neither has been proven by trial evidence.
Three Loneliness Claims That Outrun the Data
Three claims get repeated more confidently than the data support:
- “Loneliness is as bad for you as smoking 15 cigarettes a day.” This quantitative claim traces to Holt-Lunstad and colleagues’ 2010 meta-analysis of social-relationship effects on mortality.7 The original analysis reported an OR of 1.50 for stronger social relationships on mortality — a meaningful effect, but the cigarette comparison was a rhetorical translation, not a direct empirical equivalence. Smoking’s mortality effect is also far from a single number; it depends on duration, intensity, age at cessation, and many other factors. The comparison has become a meme, repeated across coverage in ways that overstate the analogy’s precision.
- “Loneliness causes 871,000 deaths per year.” The Rodrigues review cites this figure approvingly in its introduction.1 The number derives from the WHO Commission on Social Connection’s headline projection, which extrapolates from observational associations. Treating it as a measured death count rather than a model-based estimate inflates the apparent precision. The directional claim — that loneliness and social isolation contribute meaningfully to mortality at population scale — is well-supported by the broader Holt-Lunstad 2015 mortality meta-analysis.8 The specific number is not.
- “Social media causes loneliness.” The empirical record is mixed at best. Heavy social-media use correlates with self-reported loneliness in cross-sectional samples, but longitudinal and quasi-experimental studies find effects close to zero or in mixed directions. The most defensible read is that social media displaces some types of higher-quality interaction for some users while substituting for unavailable interaction for others, with the net effect dependent on use patterns rather than total time. Treating screen time as a uniform loneliness driver overspecifies what the data show.
Where the Loneliness Literature Has Methodological Limits
Several structural limitations cut across the loneliness literature.
The studies disagree wildly on the size of the effect. The heterogeneity score (I²) sits near 100% in the Rodrigues analysis for both Alzheimer’s and suicide outcomes, meaning the pooled number averages across studies whose true effects are almost certainly different from each other.1 The pooled OR points the right way; the exact size can’t be pinned down.
Cross-sectional dominance limits causal inference. The Rodrigues review pooled results across case-control, cohort, cross-sectional, and Mendelian designs. Cross-sectional studies were the largest single category, and they cannot distinguish whether loneliness precedes the outcome or follows it. The smaller longitudinal hazard ratios are the more defensible estimates of forward causal effect.
Loneliness measurement is inconsistent. The construct is measured variously by single-item subjective rating (“How often do you feel lonely?”), the UCLA Loneliness Scale (3-item or 20-item versions), the de Jong Gierveld scale, or social-network size proxies (which conflate loneliness with social isolation — related but conceptually distinct constructs). Pooling across these measurement approaches is part of why heterogeneity is so high.
Depression is hard to fully account for. Depression overlaps with loneliness, dementia, and suicide as a shared driver in nearly every study.1 Most analyses try to control for it, but mild depressive symptoms below a clinical threshold likely still leak through — some of what looks like a loneliness effect may actually be uncaught depression.
Generalizability skews toward older adults and high-income settings. Most longitudinal data on loneliness and dementia come from cohorts in the US and Europe over age 60. Effect sizes in younger populations and in low- and middle-income settings are less well-characterized.
How to Act on Loneliness as a Clinical Risk Factor
Loneliness is a documented risk factor for both cognitive decline and suicide, and addressing it has essentially no medical downside. The calibration above is about the size and shape of the effect, not whether it’s worth taking seriously.
- Treat loneliness as a clinical signal, not a personality trait. Persistent loneliness in an older adult is associated with measurable downstream risk for dementia and depression. Asking about it directly — in primary care visits, in psychiatric assessments, in caregiver intake — is low-cost and high-yield. The single-item question “How often do you feel lonely?” carries most of the predictive signal of longer scales.
- Quality of social contact matters more than quantity. The literature consistently finds that perceived loneliness predicts outcomes more strongly than objective social-network size. Living with someone but feeling unseen is worse than living alone with regular meaningful contact. Interventions that focus on connection quality outperform those focused on activity scheduling alone.
- Group-based cognitive interventions show the most consistent benefit. Cognitive-behavioral group therapy adapted for loneliness, structured peer-support programs, and reminiscence therapy in older adults all show modest but measurable reductions in self-reported loneliness in randomized trials. Effect sizes are in the small-to-moderate range — meaningful, not dramatic.
- Address depression and loneliness together. Given depression’s role as the central shared correlate, untreated depression is a likely contributor to persistent loneliness in many cases. Standard depression treatments (CBT, antidepressants where indicated, behavioral activation) often produce secondary improvements in loneliness as a byproduct.
- Suicide-risk assessment in older adults should explicitly probe disconnection. Van Orden’s disconnectedness construct has direct clinical utility. Recent loss of a spouse, recent move from a long-term home, recent loss of community participation, and recent functional decline that reduces social access are all flags that should escalate concern in routine geriatric assessment.
What People Ask About Loneliness and Long-Term Risk
Does loneliness cause Alzheimer’s disease, or just predict it?
Both are partially true. Cross-sectional associations are inflated by reverse causation — people with early cognitive decline become more isolated. Prospective cohort data find smaller but persistent forward effects (HR ~1.26 to 1.4 in the cleanest analyses).2,3 The causal arrow from loneliness to incident dementia is plausible and supported by mechanism work but not formally proven by RCT evidence.
Is loneliness “as bad as smoking 15 cigarettes a day”?
The directional claim — that chronic loneliness is a meaningful mortality risk factor — is supported. The specific cigarette equivalence is a 2010 rhetorical translation of a single mortality OR and shouldn’t be read as a precise empirical match.7 The risk is well-documented; the comparison is loose.
How much loneliness is too much?
Persistent loneliness across months is the risk-relevant pattern; transient loneliness during life transitions is normative and not pathological. Most clinical screens flag scores corresponding to “frequent” or “always” responses on validated instruments. The single-item question “How often do you feel lonely?” with a “frequent/always” response carries clinically meaningful predictive value.
Does talking to people online count, or do I need in-person contact?
Mixed evidence. Synchronous high-quality online interaction (video calls with people you know well) appears comparable to in-person contact for loneliness reduction in the available data. Passive social-media consumption shows weaker or null effects. The question is less in-person vs. online and more about whether the contact involves genuine reciprocal attention.
Do loneliness interventions reduce it?
Modestly. Group-based CBT adapted for loneliness, structured peer-support programs, and reminiscence therapy all produce small-to-moderate reductions in self-reported loneliness in RCTs. The largest effects come from interventions that address the cognitive interpretation of social interaction (CBT-style) rather than just increasing the volume of activity. Befriending programs alone show smaller effects.
Is loneliness a risk factor for suicide independent of depression?
Partially. Depression mediates a meaningful share of the loneliness-suicide path, but loneliness shows independent predictive value in studies that adjust for depression.1,6 Joiner’s interpersonal theory and Van Orden’s older-adult model both treat disconnectedness as a primary risk factor distinct from depressed mood. If you are experiencing thoughts of suicide, please reach out to a trusted person or local crisis service.
References
- Loneliness as an Interface Between Alzheimer’s Disease and Suicidal Behaviour: A Systematic Review, Meta-Analysis and Meta-Analytic Factor Analysis. Rodrigues JFR et al. Psychogeriatrics. 2026;26:e70165. doi:10.1111/psyg.70165
- Does loneliness contribute to mild cognitive impairment and dementia? A systematic review and meta-analysis of longitudinal studies. Lara E et al. Ageing Research Reviews. 2019;52:7-16. doi:10.1016/j.arr.2019.03.002
- Loneliness and Risk of Dementia. Sutin AR et al. The Journals of Gerontology: Series B. 2020;75(7):1414-1422. doi:10.1093/geronb/gby112
- The neuroendocrinology of social isolation. Cacioppo JT et al. Annual Review of Psychology. 2015;66:733-767. doi:10.1146/annurev-psych-010814-015240
- The Interpersonal Theory of Suicide. Van Orden KA et al. Psychological Review. 2010;117(2):575-600. doi:10.1037/a0018697
- Suicides in late life. Conwell Y, Van Orden K, Caine ED. Psychiatric Clinics of North America. 2011;34(2):451-468. doi:10.1016/j.psc.2011.02.002
- Social relationships and mortality risk: a meta-analytic review. Holt-Lunstad J, Smith TB, Layton JB. PLOS Medicine. 2010;7(7):e1000316. doi:10.1371/journal.pmed.1000316
- Loneliness and social isolation as risk factors for mortality: a meta-analytic review. Holt-Lunstad J et al. Perspectives on Psychological Science. 2015;10(2):227-237. doi:10.1177/1745691614568352
- The Lonely Brain: Aberrant Engagement of Allostatic Networks in Loneliness. Lam JA et al. Neuropsychopharmacology Reviews. 2021;46:97-114. doi:10.1038/s41386-020-00838-x
- The global, regional, and national prevalence of loneliness in older adults: a systematic review and meta-analysis. Surkalim DL et al. BMJ. 2022;376:e067068. doi:10.1136/bmj-2021-067068