Cognitive impairment in first-episode schizophrenia (FES) is the symptom that does the most work blocking employment, relationships, and independent living — and the symptom current antipsychotics barely move. A 2026 RCT by Hu et al. in Psychological Medicine tested whether 20 sessions of low-frequency rTMS targeting the right orbitofrontal cortex (OFC) could improve cognition where pills don’t.1
Research Highlights
- Right-OFC target: Hu 2026 randomized 90 drug-naive first-episode schizophrenia patients to active or sham stimulation.1
- 20-session protocol: 1 Hz rTMS was delivered over 4 weeks, alongside olanzapine 10–20 mg/day.1
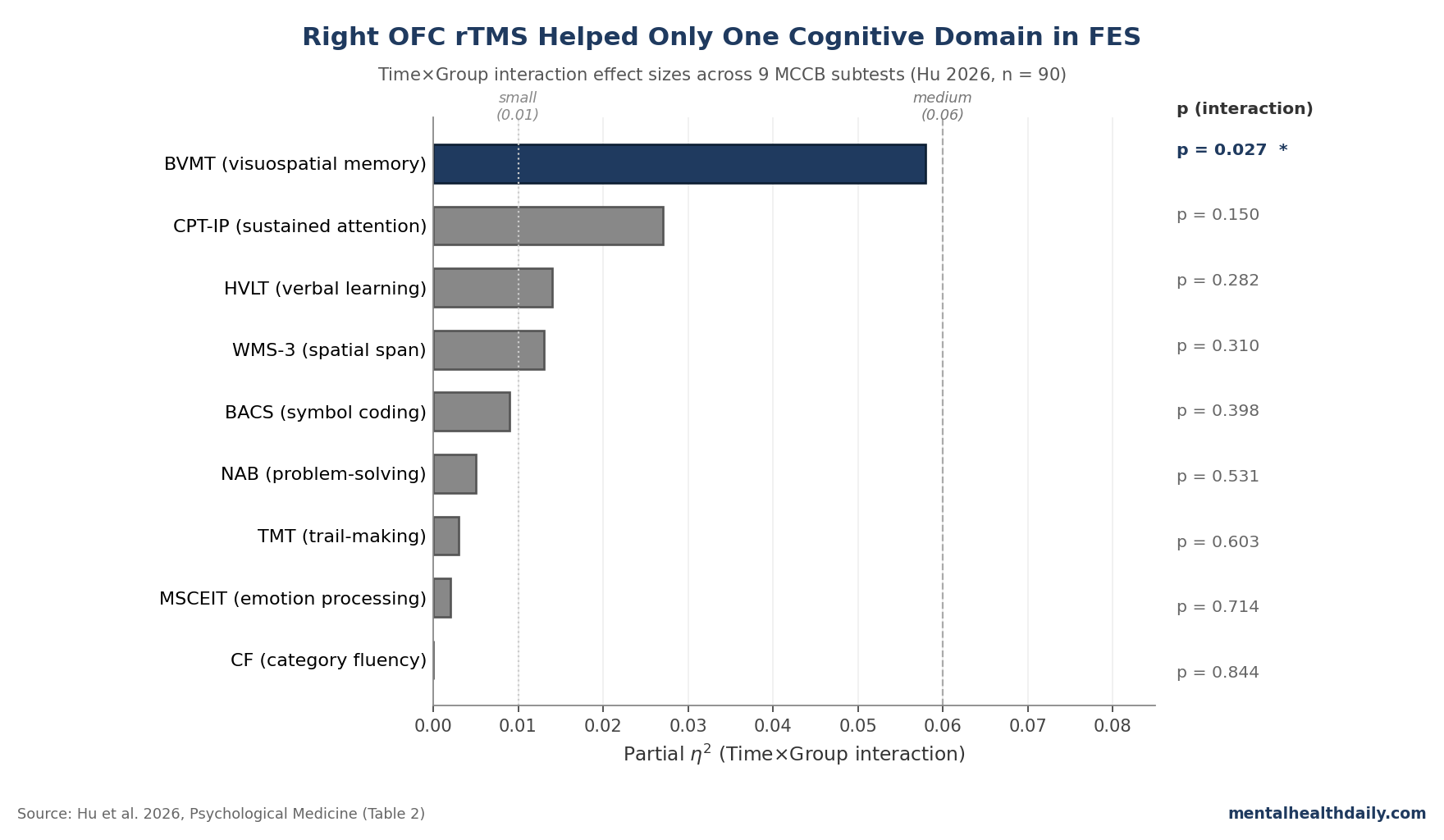
- Visuospatial memory signal: only BVMT improved significantly (F = 5.079, p = 0.027, η² = 0.058).1
- Eight null MCCB domains: the other 8 cognitive subtests showed no Time×Group interaction (all p > 0.05).1
- Research signal only: right-OFC rTMS is not clinic-ready after 1 schizophrenia cognition RCT.1,4
The honest read: one specific domain (visuospatial memory) improved meaningfully, the other 8 MCCB subtests did not, and the popular framing of “rTMS for schizophrenia cognition” needs to get a lot more domain-specific to be useful.
That places the Hu trial in the calibration zone the broader rTMS-in-schizophrenia literature has been stuck in for a decade: small samples, mixed targets, and domain-specific signals that don’t always replicate.2,3
Why OFC Differs from a Decade of DLPFC rTMS Trials in Schizophrenia
Almost every rTMS-in-schizophrenia trial before 2024 targeted one of two regions: the dorsolateral prefrontal cortex (DLPFC) for negative symptoms and cognition, or the left temporoparietal cortex for auditory hallucinations.2,5 Results have been mixed: pooled estimates suggest small-to-modest cognitive gains with high heterogeneity, and the multi-site RESIS trial (Wobrock et al.) found no meaningful negative-symptom effect from prefrontal high-frequency rTMS in 157 patients.3,6
The right OFC is a different bet. It sits at the junction of limbic, motivational, and cognitive networks, densely connected to amygdala and hippocampus on one side and lateral prefrontal regions on the other.7 Functionally, it builds “cognitive maps” that link cues, contexts, and outcomes — the substrate for visuospatial memory consolidation through OFC–hippocampal–parietal circuits.4
If that account is right, OFC stimulation should produce a different cognitive signature than DLPFC stimulation: less working-memory benefit, more memory-consolidation benefit. The Hu data are at least consistent with that prediction — though one trial in 90 patients can’t carry it alone.
The 1 Hz Right-OFC Protocol: 720 Pulses, 20 Sessions, 14,400 Total
The active protocol used 1 Hz stimulation at 110% of motor threshold over the AF8 site — the international 10–20 EEG location that maps onto the right lateral OFC in adult MRI co-registration studies.1 Each session ran 12 trains of 60 pulses with 30-second inter-train intervals: 720 pulses per session, 14,400 pulses across 20 sessions over 4 weeks.
Low-frequency (1 Hz) stimulation is generally considered inhibitory. The implicit hypothesis is that the right lateral OFC is hyperactive at baseline in FES and that selectively damping it normalizes downstream limbic-prefrontal coupling.1,7 The sham coil matched the active coil in appearance, weight, and acoustic click, with separate blinded teams handling assessment and administration — though blinding integrity was not formally verified at trial end.
All patients took olanzapine 10–20 mg/day; mean dose at week 4 was 16.5 mg active vs. 16.9 mg sham. Olanzapine has its own modest cognitive footprint, so the trial isolates rTMS-specific effects only through the Time×Group interaction — not through any single-arm change score.
BVMT Was the Only Cognitive Domain Where Active Beat Sham
Across 9 MCCB subtests, the Time×Group interaction reached significance for exactly one: the Brief Visuospatial Memory Test-Revised (BVMT). The active group’s within-group BVMT change was substantial (t = 3.631, df = 43, p = 0.0007); the sham group’s was non-significant (p = 0.312). The interaction effect size was η² = 0.058 — a medium effect by Cohen’s benchmarks (small = 0.01, medium = 0.06, large = 0.14).1
The other 8 domains looked like null results in every direction:
- Sustained attention (CPT-IP): showed a significant Group main effect (F = 4.005, p = 0.049) reflecting baseline-collapsed differences, but no Time×Group interaction (p = 0.150). The authors are careful to note this is not a treatment effect.
- Symbol coding (BACS), spatial span (WMS-3), problem-solving (NAB Mazes), trail-making (TMT): all showed Time effects (both groups improved with practice and symptom reduction) but no Time×Group separation.
- Verbal learning (HVLT), category fluency (CF), emotion processing (MSCEIT): no Time effect, no Time×Group effect, no signal.
The implication is that right-OFC rTMS is not a general cognitive enhancer in FES. It is, in this trial, a domain-specific intervention with one positive readout.
Why Visuospatial Memory and Not Anything Else?
The strongest mechanism is OFC–hippocampal–parietal circuitry. The right lateral OFC integrates spatial and contextual information with memory-encoding processes, and the BVMT asks patients to recall visual layouts over a delay — a task that loads exactly that circuit.4,7
Earlier TMS-EEG work from the same Shanghai group (Jiao 2024) showed altered global cortical responses to OFC stimulation in drug-naive schizophrenia, supporting the idea that the right OFC is plastic and modulable in this population.8
The story is plausible and the numbers fit, but a single positive subtest out of 9 also fits a multiple-comparisons explanation. The authors did not Bonferroni-correct the primary RMANOVA across cognitive domains. With 9 outcomes, the family-wise probability of at least one false positive at α = 0.05 is roughly 37%, and the BVMT result’s p = 0.027 would not survive a Bonferroni correction across 9 domains (corrected threshold ≈ 0.0056).
That limitation does not refute the finding — the within-group BVMT improvement is robust (p = 0.0007), the correlation with symptom reduction is independently significant after Bonferroni correction, and the mechanism was pre-specified. But a single trial is not enough. Replication in a larger pre-registered sample with BVMT as the primary outcome would settle it.
Cognitive Gains Tracked Symptom Reduction — in the Active Arm Only
Right OFC stimulation also reduced PANSS total scores more than sham (58.9 vs. 67.3, p = 0.003, Cohen’s d = 0.65 — a medium-to-large clinical effect). Within the active group, after Bonferroni correction:
- BVMT change correlated with PANSS-total change (r = 0.440, p = 0.003) and with PANSS-G change (r = 0.473, p = 0.001).
- NAB change correlated with PANSS-total change (r = 0.489, p = 0.001) and with PANSS-G change (r = 0.440, p = 0.003).
- No symptom-cognition correlations survived Bonferroni in the sham group — the practice-effect cognitive gains in sham did not track symptom relief.
The pattern is consistent with the OFC acting as a hub that couples emotional/motivational regulation with cognitive integration. When stimulation modulates the hub, both downstream outputs — symptom expression and memory consolidation — move in step. When the hub isn’t modulated, the modest cognitive gains from practice and antipsychotic effect are uncoupled from symptom change. Strong claim, single trial — but the directional pattern is informative.
Where Hu 2026 Fits in the Broader rTMS-for-Schizophrenia Evidence
Three foundational comparators frame how to read this trial:
- DLPFC for cognition (Jiang 2019 meta-analysis). Pooled across 9 trials of high-frequency DLPFC rTMS for cognitive deficit in schizophrenia (351 patients), the meta-analytic estimate showed a small working-memory benefit (SMD 0.34, p = 0.009).3 Hu 2026 doesn’t replicate the working-memory signal — spatial span and BACS were both null — consistent with the OFC vs. DLPFC dissociation.
- Multi-site DLPFC RCT (RESIS). The largest sham-controlled rTMS trial in schizophrenia (n = 157) tested 10 Hz left-DLPFC stimulation for negative symptoms and found no significant benefit, setting the bar that small positive single-site trials in this literature need to clear.6 Hu 2026 is well below that sample size and uses a different target; its 90-patient signal is hypothesis-generating, not confirmatory.
- Lefaucheur 2020 evidence-based guidelines. The European expert consensus rated rTMS for negative symptoms as Level C (possible efficacy) for left DLPFC at 10 Hz and noted the lack of consensus on cognitive applications.2 A 2026 right-OFC signal doesn’t move guidelines, but it opens a target the guidelines haven’t had reason to evaluate.
The accelerated SAINT protocols Cole and Williams developed for treatment-resistant depression (5 days of intermittent theta-burst with personalized fMRI targeting) have stayed in mood disorders so far.9 If the OFC-cognition signal holds up, an analogous accelerated personalized-targeting protocol for FES is the obvious next step.
Limitations of the Hu Trial
Five caveats deserve weight:
- Olanzapine confound. Every patient took 10–20 mg/day olanzapine throughout. While dose didn’t differ between groups, olanzapine has modest cognitive effects and the trial cannot fully separate rTMS-specific gains from antipsychotic effects potentiated in the active arm. A medication-free cohort would clarify this.
- Unequal arm sizes from differential dropout. 48 active vs. 42 sham, primarily because more sham patients withdrew. Differential dropout in psychiatric trials usually biases toward the active arm because sham patients with poorer response are more likely to drop, leaving sham completers enriched for natural improvers.
- Sample size and uncorrected RMANOVA. 90 patients across 9 cognitive domains with no Bonferroni correction on the primary analysis. The single positive BVMT signal needs replication in a pre-registered trial with BVMT as the named primary outcome before it can support clinical inference.
- Blinding integrity not formally tested. The trial did not include an end-of-study guess-the-arm question, the standard demand-effect probe. This leaves open whether expectancy contributed to either the cognitive or the symptom result.
- 4-week endpoint, no long-term follow-up. No information on whether the BVMT gain persists at 3, 6, or 12 months — the durability question that determines whether maintenance sessions would be needed clinically.
The trial is also a secondary analysis of an RCT whose primary symptom outcomes were already published.10 That doesn’t invalidate the cognitive findings, but it means the cognitive endpoints weren’t the primary registered outcome of the parent trial.
OFC rTMS Is Not Ready for Routine FES Cognitive Care
Right-OFC rTMS is not a clinical option for FES cognition in 2026. The Hu trial is the strongest single signal so far — a domain-specific effect on visuospatial memory in a small sample — but cognitive remediation therapy remains the established non-pharmacological cognition intervention in schizophrenia for clinics willing to deliver it.
The next evidentiary step is straightforward: larger pre-registered OFC trials with a visuospatial composite as the primary outcome, plus head-to-head OFC vs. DLPFC comparisons in matched FES samples. The pre-specified mechanism plus the Time×Group dissociation against 8 null domains justifies that trial design.
For FES patients and families: cognitive improvement in schizophrenia in 2026 still runs through symptom stabilization, sleep, exercise, and structured cognitive remediation when accessible. rTMS is a research target, not a treatment recommendation.
What Patients and Clinicians Ask About OFC rTMS
Is rTMS approved for schizophrenia anywhere?
rTMS is FDA-approved for major depressive disorder, OCD, smoking cessation, and migraine — not for schizophrenia. The European Lefaucheur guidelines rated rTMS for negative symptoms as Level C (possible efficacy) with left DLPFC stimulation, but no regulator currently recognizes rTMS as a schizophrenia treatment.2
Why does OFC stimulation matter if DLPFC has been studied longer?
DLPFC and OFC sit in different functional networks. DLPFC stimulation has produced mixed cognition results in schizophrenia across more than a decade of trials.3,6 OFC stimulation targets a region tied to memory consolidation and emotional-motivational integration, which Hu 2026 suggests may produce a visuospatial memory signal rather than the working-memory benefit DLPFC trials chase.1,4
How big was the BVMT effect in practical terms?
Medium (η² = 0.058). The active group’s BVMT score moved from 19.2 at baseline to 22.9 at 4 weeks; the sham group moved from 19.7 to 20.5.
The between-group difference at endpoint did not reach significance on a simple t-test (p = 0.156), so the “effect” is the differential improvement over time, not a cross-sectional gap at endpoint.1
Should patients with first-episode schizophrenia ask about rTMS?
Not as a treatment. The trial is a research finding in 90 patients with 1 positive cognitive subtest out of 9. The standard remains stable antipsychotic treatment, structured cognitive remediation when available, and supportive care — with rTMS reserved for clinical trials that patients can choose to enroll in.
Are there safety concerns with low-frequency OFC stimulation?
No serious adverse events in the Hu trial. The 1 Hz protocol with 30-second inter-train intervals is conservative on seizure-risk grounds, and standard rTMS side effects (transient headache, scalp discomfort, fatigue) were monitored on a 7-symptom checklist after each session.
OFC stimulation sits closer to the eye and frontal sinuses than DLPFC stimulation, which can produce more facial-area discomfort.1
References
- The effects of rTMS over orbitofrontal cortex on cognitive functions in first-episode schizophrenia. Hu Q, Jiao X, Ding Y, et al. Psychological Medicine. 2026;56:e119. doi:10.1017/S0033291726103912
- Evidence-based guidelines on the therapeutic use of repetitive transcranial magnetic stimulation (rTMS): an update (2014–2018). Lefaucheur JP, Aleman A, Baeken C, et al. Clinical Neurophysiology. 2020;131(2):474–528. doi:10.1016/j.clinph.2019.11.002
- Effects of high-frequency transcranial magnetic stimulation for cognitive deficit in schizophrenia: a meta-analysis. Jiang Y, Guo Z, Xing G, et al. Frontiers in Psychiatry. 2019;10:135. doi:10.3389/fpsyt.2019.00135
- The role of the lateral orbitofrontal cortex in creating cognitive maps. Costa KM, Scholz R, Lloyd K, et al. Nature Neuroscience. 2023;26(1):107–115. doi:10.1038/s41593-022-01216-0
- Examining transcranial direct-current stimulation (tDCS) as a treatment for hallucinations in schizophrenia. Brunelin J, Mondino M, Gassab L, et al. American Journal of Psychiatry. 2012;169(7):719–724. doi:10.1176/appi.ajp.2012.11071091
- Left prefrontal high-frequency repetitive transcranial magnetic stimulation for the treatment of schizophrenia with predominant negative symptoms: a sham-controlled, randomized multicenter trial. Wobrock T, Guse B, Cordes J, et al. Biological Psychiatry. 2015;77(11):979–988. doi:10.1016/j.biopsych.2014.10.009
- The multifaceted role of the ventromedial prefrontal cortex in emotion, decision making, social cognition, and psychopathology. Hiser J, Koenigs M. Biological Psychiatry. 2018;83(8):638–647. doi:10.1016/j.biopsych.2017.10.030
- Abnormal global cortical responses in drug-naive patients with schizophrenia following orbitofrontal cortex stimulation: a concurrent transcranial magnetic stimulation-electroencephalography study. Jiao X, Hu Q, Tang Y, et al. Biological Psychiatry. 2024;96(5):342–351. doi:10.1016/j.biopsych.2024.05.024
- Stanford Accelerated Intelligent Neuromodulation Therapy for treatment-resistant depression. Cole EJ, Stimpson KH, Bentzley BS, et al. American Journal of Psychiatry. 2020;177(8):716–726. doi:10.1176/appi.ajp.2019.19070720
- Early improvement of psychopathological symptoms with add-on repetitive transcranial magnetic stimulation treatment as the key contributor to improving remission in schizophrenia. Hu Q, Jiao X, Tang X, et al. Journal of Psychiatric Research. 2025;188:64–73. doi:10.1016/j.jpsychires.2025.05.045