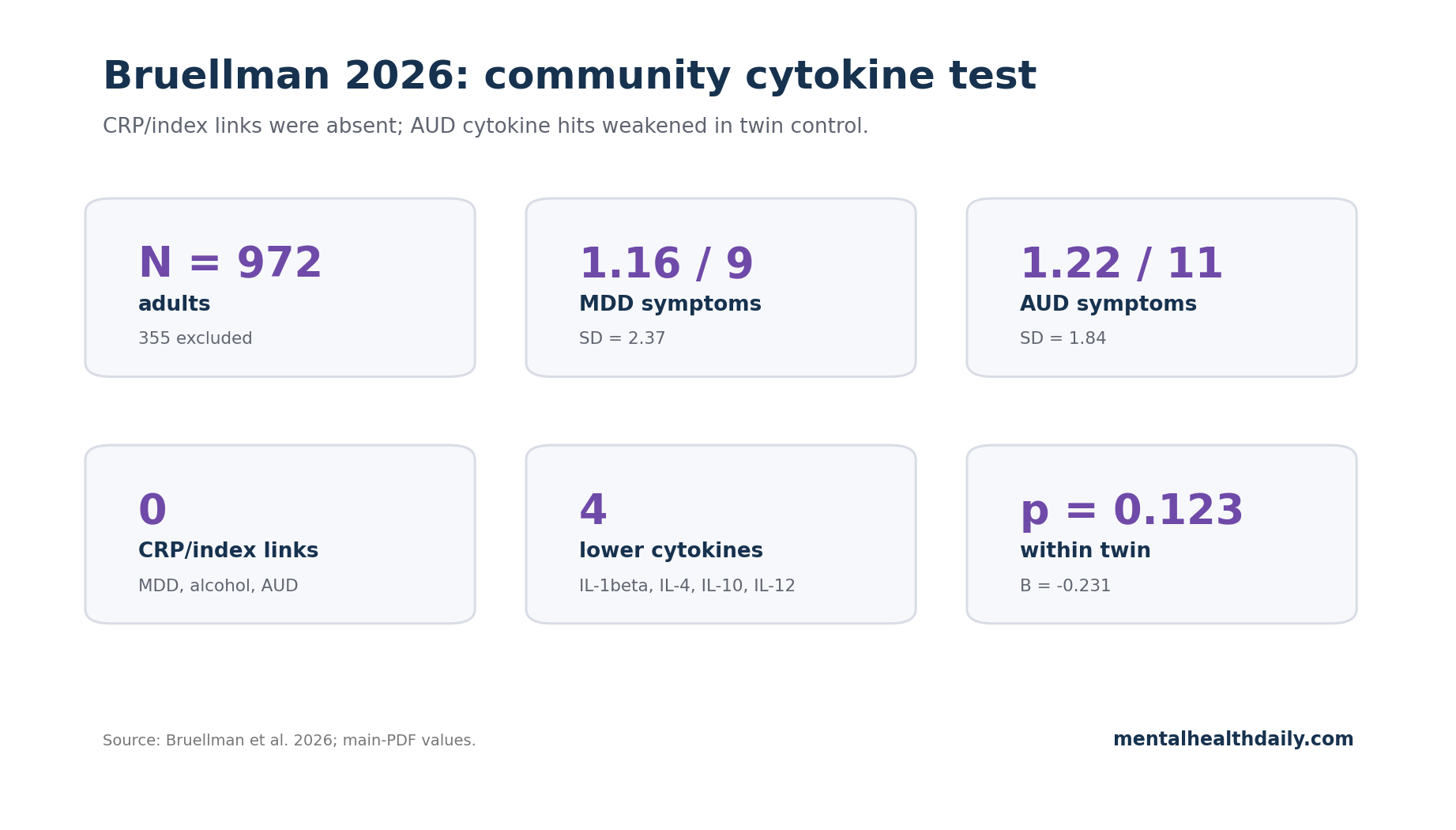
The broad cytokine story failed its most direct community test: in 972 adults, depression, alcohol use, and alcohol use disorder (AUD) were not associated with C-reactive protein (CRP) or a pre-registered pro-inflammatory cytokine index. The only multiple-testing-corrected cytokine hits ran opposite the hypothesis — AUD was linked to lower IL-1β, IL-4, IL-10, and IL-12 — and those inverse links became nonsignificant when twins were compared within families.1
Research Highlights
- Primary inflammation tests were null: depression symptoms, alcohol quantity, alcohol frequency, weekly drinks, and AUD symptoms showed 0 significant associations with CRP or the IL-1β/IL-6/TNF-alpha pro-inflammatory index in 972 community adults.1
- AUD effects reversed direction: Bruellman et al. expected heavier alcohol use and AUD to track higher cytokines, but AUD was associated with lower levels of 4 individual cytokines after the 0.00625 Bonferroni threshold.1
- Twin control weakened the finding: for IL-1β, the co-twin follow-up remained nonsignificant for both the between-family effect (B = −0.183, p = 0.182) and within-family effect (B = −0.231, p = 0.123).1
- Low symptom burden matters: the sample averaged 1.16 of 9 MDD symptoms and 1.22 of 11 AUD symptoms, so the result is strongest for generally healthy community adults rather than severe MDD or severe AUD.1
- Subgroup evidence narrows the cytokine claim: a 1,724-person CRP analysis found the depression-CRP link disappeared after confounder control, while inflammatory-challenge work still supports high-CRP depression as a narrower subtype.2,3
Cytokines are immune-signaling proteins that help coordinate inflammation. The depression version of the hypothesis usually focuses on pro-inflammatory markers such as IL-6, IL-1β, TNF-alpha, and CRP — not because they diagnose depression, but because they can signal immune activation that plausibly changes sleep, energy, reward sensitivity, pain, and stress biology.
Clinical studies have made that idea hard to ignore. Meta-analytic work has found higher inflammatory markers in major depression, and experimental inflammatory challenges can produce acute anhedonia in vulnerable depressed participants, especially when baseline CRP is already elevated.3,4
The question Bruellman et al. tested was narrower and more punishing: does the same pattern appear in a relatively healthy community sample when depression symptoms, alcohol behavior, CRP, cytokines, diet, antidepressant use, and family structure are measured together?
972 Adults Tested 2 Pre-Registered Cytokine Claims
Bruellman et al. used the Colorado Adoption/Twin Study of Lifespan behavioral development and cognitive aging (CATSLife1). The analyzed sample included 972 adults after 355 exclusions for missing blood draw, long timing gaps between blood and other measures, pregnancy, or medications that affect cytokines.
Mean age was 33.41 years, with a range from 28.06 to 48.98 years; 469 participants were female, 90 reported depression-medication use, and same-sex twin pairs allowed co-twin follow-up for significant findings.1
The pre-registered questions were explicit:
- Are heavier alcohol use and AUD symptoms associated with higher cytokine levels?
- Are higher cytokine levels associated with more major depressive disorder (MDD) symptoms?
The researchers hypothesized significant effects for both questions. If both directions had appeared, inflammation could have been tested as a possible mediator linking heavy drinking or AUD to depression.
Instead, the analysis did not establish the univariate links needed for mediation.
CRP is a liver-produced inflammation marker often used as a broad systemic signal. The pro-inflammatory cytokine index averaged standardized IL-1β, IL-6, and TNF-alpha values; those 3 markers correlated at r = 0.54–0.71 and produced internal consistency of 0.82, so the index was not an arbitrary bundle.
The study also examined individual cytokines including IL-4, IL-8, IL-10, IL-12, interferon-gamma, and IL-22 with a Bonferroni-corrected threshold of 0.05/8 = 0.00625.1
Depression Symptoms Did Not Track CRP or the Cytokine Index
MDD symptoms were low on average: 1.16 of 9 past-year symptoms, with a standard deviation of 2.37. Depression symptoms were not associated with CRP or with the pre-registered pro-inflammatory cytokine index.
Depression-medication use did show a strong positive association with the MDD outcome (B = 0.91, p < 0.001), which is expected because medication use marks people with more depression history or treatment contact rather than acting as an inflammation result.1
This is not a clean refutation of inflammatory depression. It is a boundary condition.
The result says a generally healthy adult community sample did not show the broad cytokine-depression association that clinical and high-inflammation samples often suggest.
That boundary fits adjacent evidence better than a simple yes/no fight over inflammation. Figueroa-Hall et al. analyzed 1,724 people and found that the CRP-depression association was explained by medical, social, and demographic confounders such as BMI.2
Savitz et al. tested an endotoxin inflammatory challenge in major depression and focused on elevated baseline CRP as the subgroup where anhedonic and inflammatory responses were most relevant.3 The stronger synthesis is specific: inflammation looks more plausible as a depression pathway in selected immune-metabolic subgroups than as a universal community-level depression signal.
AUD Linked to 4 Lower Cytokines Before Co-Twin Control
Alcohol behavior also failed the pre-registered primary tests. Alcohol quantity, alcohol frequency, weekly drinks, and AUD symptoms were not associated with CRP or the pro-inflammatory cytokine index.1
The individual-cytokine results were more surprising. AUD symptoms were associated with lower IL-1β, IL-4, IL-10, and IL-12 after correction for multiple testing.
The paper’s discussion states the direction plainly: “Contrary to our hypotheses,” the data provided little evidence that cytokines were biomarkers of AUD or MDD symptom severity, and the significant AUD effects indicated lower circulating cytokines.1
That does not make alcohol protective. IL-4 and IL-10 are usually described as anti-inflammatory cytokines, so lower levels can mean immune dysregulation rather than lower inflammatory danger.
More importantly, AUD severity was modest in this sample: participants averaged 1.22 of 11 AUD symptoms, alcohol frequency averaged 0.66 drinking days per week, and quantity averaged 2.00 drinks per drinking day. This was not a residential-treatment AUD cohort with liver disease, recurrent infections, withdrawal physiology, and heavy medical burden layered on top.1
Familial Confounding Weakens the Alcohol-Cytokine Signal
Co-twin control means comparing twins from the same family who differ on the exposure, rather than comparing unrelated people. The design controls many genetic and shared-family factors that can make twins similar before alcohol behavior enters the model.5
Bruellman et al. used co-twin control only after significant full-sample effects appeared. For IL-1β, the AUD between-family effect was negative but nonsignificant (B = −0.183, p = 0.182), and the within-family effect was also negative but nonsignificant (B = −0.231, p = 0.123).
Monozygotic-twin attenuation also pointed toward confounding (B = 0.159, p = 0.397). The researchers interpreted the inverse AUD-cytokine associations as likely explained by familial confounders rather than a direct effect of AUD lowering cytokines.1
That fits a broader alcohol-methodology lesson. Older observational studies sometimes made moderate alcohol use look biologically or medically protective, but systematic work has shown how reference-group bias, former-drinker effects, illness-related abstention, and other selection problems can bend the association.6,7
Bruellman et al. are not studying mortality, but the inference problem is similar: an inverse alcohol-health association is not automatically a protective alcohol effect.
Clinical AUD and Community AUD Are Not the Same Inflammation Test
Severe AUD samples can look immunologically different from this community sample. Leclercq et al., for example, studied alcohol-dependent subjects in a clinical context where intestinal permeability and inflammation were part of the biological picture.8
Bruellman et al. explicitly note that evidence for cytokines differentiating AUD status often comes from residential-treatment patients, where AUD is likely more severe and medical comorbidity is more common.1
Those 2 literatures can both be true. Heavy alcohol exposure can contribute to liver injury, gut barrier disruption, infection risk, and immune changes in severe AUD.
A community sample with low average AUD symptoms may instead show no CRP/index elevation and only fragile inverse individual-cytokine patterns. The clinical claim should therefore be staged by severity and comorbidity, not written as “alcohol raises cytokines” across every population.
Limits of This Cross-Sectional Twin Analysis
The design is stronger than a generic observational association, but it still has real limits.
Timing remains unresolved. Cytokines, depression symptoms, and alcohol behavior were measured cross-sectionally. The study cannot show whether changes in inflammation precede changes in mood or drinking, or whether drinking changes later cytokine trajectories.
Single blood draws are noisy. CRP and cytokines can move with infection, sleep loss, acute stress, recent exercise, and recent alcohol timing. A single measurement can miss within-person inflammatory patterns even when the assay is technically sound.
Severity range is restricted. The strongest inference applies to generally healthy adults aged 28–49 with low average MDD and AUD symptom counts. Treatment-resistant depression, autoimmune comorbidity, severe AUD, liver disease, older age, and high-CRP immune-metabolic depression remain different questions.
Main-PDF coefficients were limited. The paper reports the core direction and gives a co-twin IL-1β example in text, but many exact model coefficients sit in figures or supplements rather than clean main-text tables. Any quantitative visual for this draft therefore has to stay close to numbers that are actually printed in the source PDF, not reconstructed from figure images.
How to Use This Result
For depression, the Bruellman result argues against a blanket cytokine explanation. It does not argue against measuring CRP in selected patients, testing immune-metabolic subtypes, or studying anti-inflammatory adjuncts in high-inflammation depression.
A broad null in healthy community adults and a subgroup signal in inflamed clinical depression are compatible.
For alcohol, the practical correction is sharper: do not read lower cytokines in the AUD models as evidence that alcohol lowers inflammatory risk. The co-twin analyses make familial confounding the cleaner explanation, and severe AUD biology still carries plausible inflammatory and immune-disruption pathways.
Questions About This Cytokine Twin Study
Did this study disprove inflammatory depression?
No. It failed to find a broad CRP or pro-inflammatory cytokine-index association with MDD symptoms in 972 generally healthy community adults.
That weakens universal claims, but it leaves high-CRP depression, immune-metabolic depression, treatment-resistant depression, and medically inflamed subgroups open.
Did Bruellman et al. show alcohol is anti-inflammatory?
No. AUD was associated with lower levels of 4 individual cytokines in full-sample models, but those inverse links became nonsignificant in co-twin control analyses.
The cleaner interpretation is familial confounding or immune dysregulation, not a protective alcohol effect.
Why did IL-4 and IL-10 complicate the AUD finding?
IL-4 and IL-10 are usually considered anti-inflammatory cytokines. Lower levels of those markers do not mean the immune system is simply less inflamed; they may signal poorer regulation of inflammatory activity.
Why are twin comparisons useful here?
Twins share genes and family environment. If the twin with more AUD symptoms also had reliably lower cytokines than the co-twin, a direct exposure interpretation would look stronger.
That within-family pattern was not significant in the reported follow-up.
Should CRP guide depression treatment after this result?
This paper does not test treatment. It supports using CRP and cytokines carefully: useful for selected inflammatory-depression research or biomarker-guided trials, weak as a universal explanation for ordinary community depression symptoms.
References
- Bruellman R, Reynolds CA, Smolen A, et al. Inflammation, mental health, and alcohol behaviors: testing links leveraging a familial community sample. Brain, Behavior, & Immunity – Health. 2026;53:101229. doi:10.1016/j.bbih.2026.101229
- Figueroa-Hall LK, Xu B, Kuplicki R, et al. Psychiatric symptoms are not associated with circulating CRP concentrations after controlling for medical, social, and demographic factors. Translational Psychiatry. 2022;12(1):279. doi:10.1038/s41398-022-02049-y
- Savitz J, Figueroa-Hall LK, Teague TK, et al. Systemic inflammation and anhedonic responses to an inflammatory challenge in adults with major depressive disorder: a randomized controlled trial. American Journal of Psychiatry. 2025;182(6):560–568. doi:10.1176/appi.ajp.20240142
- Dowlati Y, Herrmann N, Swardfager W, et al. A meta-analysis of cytokines in major depression. Biological Psychiatry. 2010;67(5):446–457. PMID:20015486
- McGue M, Osler M, Christensen K. Causal inference and observational research: the utility of twins. Perspectives on Psychological Science. 2010;5(5):546–556. doi:10.1177/1745691610383511
- Sarich P, Gao S, Zhu Y, Canfell K, Weber MF. The association between alcohol consumption and all-cause mortality: an umbrella review of systematic reviews using lifetime abstainers or low-volume drinkers as a reference group. Addiction. 2024;119(6):998–1012. doi:10.1111/add.16446
- Stockwell T, Zhao J, Panwar S, Roemer A, Naimi T, Chikritzhs T. Do “moderate” drinkers have reduced mortality risk? A systematic review and meta-analysis of alcohol consumption and all-cause mortality. Journal of Studies on Alcohol and Drugs. 2016;77(2):185–198. doi:10.15288/jsad.2016.77.185
- Leclercq S, Cani PD, Neyrinck AM, et al. Role of intestinal permeability and inflammation in the biological and behavioral control of alcohol-dependent subjects. Brain, Behavior, and Immunity. 2012;26(6):911–918. doi:10.1016/j.bbi.2012.04.001
- Grant BF, Goldstein RB, Saha TD, et al. Epidemiology of DSM-5 alcohol use disorder: results from NESARC-III. JAMA Psychiatry. 2015;72(8):757–766. doi:10.1001/jamapsychiatry.2015.0584