
A 2026 secondary randomized-trial analysis found that low-intensity focused ultrasound and repetitive transcranial magnetic stimulation reached statistically similar 2-week post-treatment motor scores after subacute stroke, even though LIFU produced larger median Fugl–Meyer Assessment gains than rTMS: 7 vs. 2 upper-limb points and 3 vs. 1 lower-limb points.1 LIFU therefore carries the recovery-dynamics signal in this comparison, while rTMS carries a mature clinical evidence base.
Research Highlights
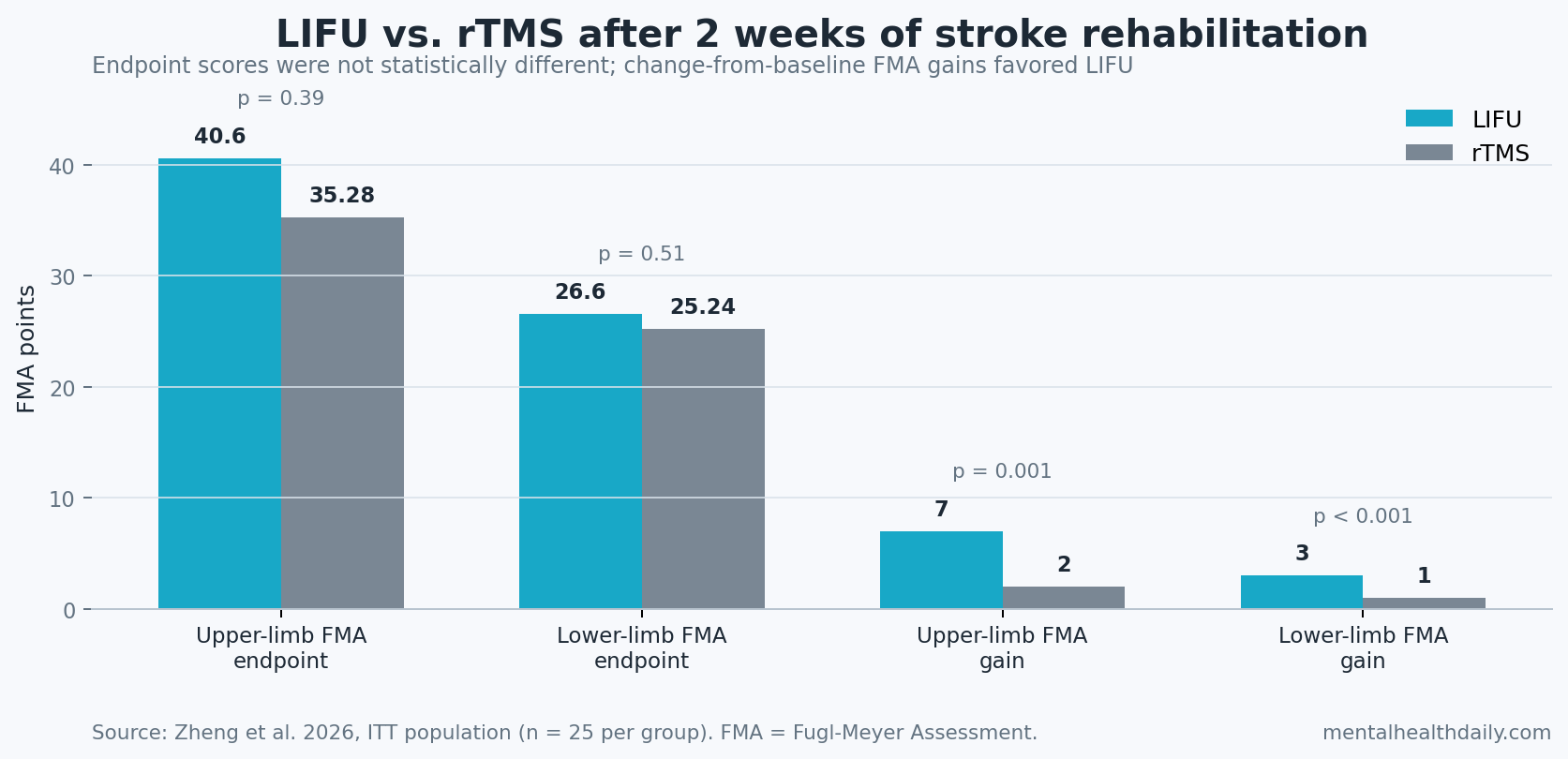
- Endpoint scores were not statistically different: after 2 weeks, upper-limb FMA was 40.60 with LIFU vs. 35.28 with rTMS (p = 0.39), and lower-limb FMA was 26.60 vs. 25.24 (p = 0.51).1
- Change scores favored LIFU: median FMA improvement was 7 vs. 2 upper-limb points (p = 0.001) and 3 vs. 1 lower-limb points (p < 0.001), which suggests a faster early motor-improvement pattern rather than proven superiority.1
- The comparison was small: 25 patients per arm were analyzed, 43 of 50 completed the full protocol, and post-hoc power was about 78% for a medium effect size.1
- Brain-activity data were exploratory: prefrontal fractional amplitude of low-frequency fluctuations increased after LIFU (p = 0.002), while connectivity changes did not survive false discovery rate correction.1
- Clinical choice still depends on evidence maturity: rTMS has a broader randomized stroke-rehabilitation literature, while human LIFU stroke work is still early, including phase I feasibility data from 2025.2,3
Low-intensity focused ultrasound (LIFU) uses focused acoustic energy to modulate neural tissue without surgery. The attraction is physical: ultrasound can be focused more tightly than magnetic stimulation and may reach deeper targets, although the clinical stroke evidence is still young.
Repetitive transcranial magnetic stimulation (rTMS) uses repeated magnetic pulses over cortex to shift cortical excitability. In stroke rehabilitation, rTMS is usually used as an adjunct to physical and occupational therapy, with the aim of improving motor-network plasticity while the patient is practicing movement.
Endpoint Scores Did Not Prove LIFU Beat rTMS
Zheng et al. analyzed 50 subacute stroke patients from a prospectively registered 3-arm randomized trial: 25 received standard rehabilitation plus LIFU, and 25 received standard rehabilitation plus rTMS.1 The standard rehabilitation-only arm was part of the parent trial but was excluded from this head-to-head comparison, so this was not a 3-way effectiveness analysis.
Protocol: both neuromodulation arms received 20-minute sessions, 5 days per week, for 2 weeks. LIFU targeted the ipsilesional primary motor cortex at 0.5 MHz with 10.2 W/cm² free-field spatial-peak pulse-average intensity, while rTMS used 10 Hz stimulation at 80% resting motor threshold with 1,000 pulses per session.
Primary clinical comparison: post-treatment scores were the main basis for comparing groups. On that test, LIFU did not statistically outperform rTMS: upper-limb FMA was 40.60 vs. 35.28 points (p = 0.39), lower-limb FMA was 26.60 vs. 25.24 (p = 0.51), and the Modified Barthel Index was 73.20 vs. 72.00 (p = 0.83).1
That endpoint result is the guardrail against overclaiming. A 5.32-point upper-limb endpoint gap may look clinically interesting, but this analysis did not statistically confirm it under the primary comparison. The fair conclusion is not that the treatments were identical; it is that this small secondary analysis did not prove a short-term endpoint advantage.
FMA Change Scores Favored LIFU Over rTMS
The change-from-baseline analysis pointed more strongly toward LIFU. Median upper-limb FMA improvement was 7 points with LIFU vs. 2 points with rTMS, and median lower-limb improvement was 3 vs. 1 point.1 Those between-group change differences were statistically significant.
How to read the split: endpoint scores answer where patients landed after 2 weeks. Change scores answer how far they moved from their own baseline. In a small subacute-stroke trial, both are relevant because spontaneous recovery, baseline severity, ceiling effects, and early rehabilitation response can all influence short-window outcomes.
Why LIFU still gets a directional nod: the change-score pattern was not a random one-off across 1 limb. It appeared in upper and lower extremities, and an analysis of covariance adjusting for baseline upper-limb FMA also favored LIFU (F = 9.901, p = 0.003), although lower-limb adjusted comparison remained nonsignificant (p = 0.076).1
Optimal interpretation: if forced to bet on the next trial’s active ingredient, lean toward LIFU as the more interesting experimental modality. If choosing a clinical service today, do not treat this 50-person secondary analysis as enough to replace the more established rTMS evidence base.
fNIRS Suggested Different Cortical Activity, Not a Confirmed Network Mechanism
Functional near-infrared spectroscopy (fNIRS) estimates cortical blood-oxygen changes from light absorption through the scalp. It is useful for bedside or rehabilitation-compatible cortical monitoring, but it mainly samples superficial cortex and is vulnerable to extracerebral blood-flow noise.
Zheng et al. used resting-state fNIRS in the 43 protocol completers. Prefrontal fractional amplitude of low-frequency fluctuations, a measure of spontaneous low-frequency cortical activity, increased after LIFU (p = 0.002; Cohen’s d = 0.54) but not after rTMS (p = 0.067).1 Motor-region change in fALFF also favored LIFU: 0.028 vs. −0.018 (p = 0.019; Cohen’s d = 0.74).
The connectivity story was weaker. Region-to-region matrices suggested more coupling after LIFU and less after rTMS, but no connectivity change survived false discovery rate correction. False discovery rate correction is a statistical adjustment used when many network comparisons are tested at once; it reduces the chance that 1 attractive-looking connection is just a multiple-testing artifact.
Mechanistic implication: LIFU may recruit a broader prefrontal-motor compensation pattern during early recovery, whereas rTMS may act more focally through motor-cortex excitability. That is a hypothesis for larger imaging trials, not proof that LIFU produces better long-term motor recovery.
rTMS Has More Stroke-Rehabilitation Evidence Than LIFU
rTMS is not new to post-stroke motor rehabilitation. A 2025 systematic review and meta-analysis summarized randomized rTMS studies for stroke motor recovery, reflecting a larger and more mature evidence base than focused ultrasound currently has in this indication.3 Evidence-based rTMS guidelines also give clinicians a safety and protocol framework that does not yet exist at the same depth for LIFU stroke rehabilitation.5
LIFU’s advantage is less about being clinically proven and more about targeting logic. Human ultrasound neuromodulation studies remain heterogeneous and early, but they support the idea that transcranial ultrasound can modulate human brain activity without invasive hardware.4 A 2025 phase I stroke study reported safety and feasibility for single-session LIFU in stroke survivors, which makes the Zheng trial a plausible next step rather than an isolated leap.2
- Why rTMS remains the default comparator: more randomized trials, more protocol experience, and broader clinical familiarity.
- Why LIFU deserves head-to-head testing: tighter spatial focus, potential access to deeper circuits, and an early FMA-change signal in the 2026 comparison.
- Why neither should be oversold: motor recovery after stroke depends on rehabilitation dose, lesion location, time since stroke, baseline impairment, and spontaneous recovery, not stimulation modality alone.
Study Design Limits Keep This in the Promising-Signal Category
This was a secondary analysis, not a trial independently powered around the LIFU vs. rTMS question. The researchers calculated about 78% power to detect a medium effect size, close to but still below the conventional 80% target.1 That makes the nonsignificant endpoint comparison hard to interpret: it might reflect real similarity, inadequate power, or a short follow-up window that missed later separation.
Time window: 2 weeks is enough to detect early movement on FMA and MBI, but it is not enough to know whether gains persist, plateau, or translate into durable independence. Stroke-recovery trials usually need longer follow-up because early motor change can be driven by spontaneous recovery and intensive practice as much as by the stimulation add-on.
Population: eligible patients were 40 to 80 years old, had first-ever stroke within 6 months, and had enough cognition and language capacity to cooperate with rehabilitation. Results should not be generalized to severe aphasia, major cognitive impairment, unstable hemorrhage, uncontrolled seizure disorders, or patients outside that subacute recovery window.
Imaging: fNIRS covered prefrontal, sensorimotor, and motor cortical regions, but it did not directly measure deep subcortical targets. That limitation is especially relevant for LIFU because part of the modality’s appeal is the ability to reach structures less accessible to standard non-invasive stimulation.
Questions About LIFU vs. rTMS After Stroke
Did LIFU beat rTMS in this trial?
Not on the main endpoint comparison. Post-treatment FMA, MBI, and Brunnstrom scores did not significantly differ between groups after 2 weeks.
Why mention LIFU if the endpoint comparison was nonsignificant?
The FMA gain analysis favored LIFU in both upper and lower limbs, and baseline-adjusted upper-limb analysis also favored LIFU. Those signals justify larger trials, but they do not establish clinical superiority.
Is rTMS still reasonable for stroke rehabilitation research?
Yes. rTMS has a larger evidence base, clearer safety infrastructure, and more clinical experience. The Zheng analysis makes LIFU more interesting as a comparator, not obsolete proof against rTMS.
What would settle the question?
A larger prospectively powered head-to-head trial should compare LIFU, rTMS, sham or rehabilitation-only control, and longer follow-up. Stratifying by lesion location, stroke phase, baseline impairment, and rehabilitation dose would make the result more clinically usable.
References
- Zheng S, Bian R, Song H, Liao Z, Gao T, Yan M, et al. A secondary head-to-head comparison of low-intensity focused ultrasound and repetitive transcranial magnetic stimulation for motor recovery after stroke. PLOS One. 2026;21(4):e0348030. https://doi.org/10.1371/journal.pone.0348030
- Huang Z, Charalambous CC, Chen M, Kim T, Sokhadze E, Song A, et al. Low intensity focused ultrasound stimulation in stroke: a phase I safety & feasibility trial. Brain Stimulation. 2025;18(1):179–187. https://doi.org/10.1016/j.brs.2025.01.015
- Xie G, Wang T, Deng L, Zhou L, Zheng X, Zhao C, et al. Repetitive transcranial magnetic stimulation for motor function in stroke: a systematic review and meta-analysis of randomized controlled studies. Systematic Reviews. 2025;14(1):47. https://doi.org/10.1186/s13643-025-02794-3
- Sarica C, Nankoo JF, Fomenko A, Grippe TC, Yamamoto K, Samuel N, et al. Human studies of transcranial ultrasound neuromodulation: a systematic review of effectiveness and safety. Brain Stimulation. 2022;15(3):737–746. https://doi.org/10.1016/j.brs.2022.05.002
- Lefaucheur JP, Aleman A, Baeken C, Benninger DH, Brunelin J, Di Lazzaro V, et al. Evidence-based guidelines on the therapeutic use of repetitive transcranial magnetic stimulation: an update (2014–2018). Clinical Neurophysiology. 2020;131(2):474–528. https://doi.org/10.1016/j.clinph.2019.11.002
- Keser Z, Ikramuddin S, Shekhar S, Feng W. Neuromodulation for post-stroke motor recovery: a narrative review of invasive and non-invasive tools. Current Neurology and Neuroscience Reports. 2023;23(12):893–906. https://doi.org/10.1007/s11910-023-01319-6