A 2026 survey of 230 Farsi-speaking refugees in German camps found a hard double signal: 69.1% screened above the RHS-15 threshold for depression, anxiety, and PTSD symptoms, while 4 protective factors explained 61% of posttraumatic-growth variance.1
Research Highlights
- High distress and growth coexisted: 159 of 230 participants (69.1%) scored ≥12 on the RHS-15 symptom scale, 158 (68.7%) scored ≥5 on the distress thermometer, and the average PTGI score was 2.61 (SD 1.52).1
- The growth model was not vague: resilience, psychological flexibility, meaning in life, and perceived social support together explained 61% of posttraumatic-growth variance in the cross-sectional regression.1
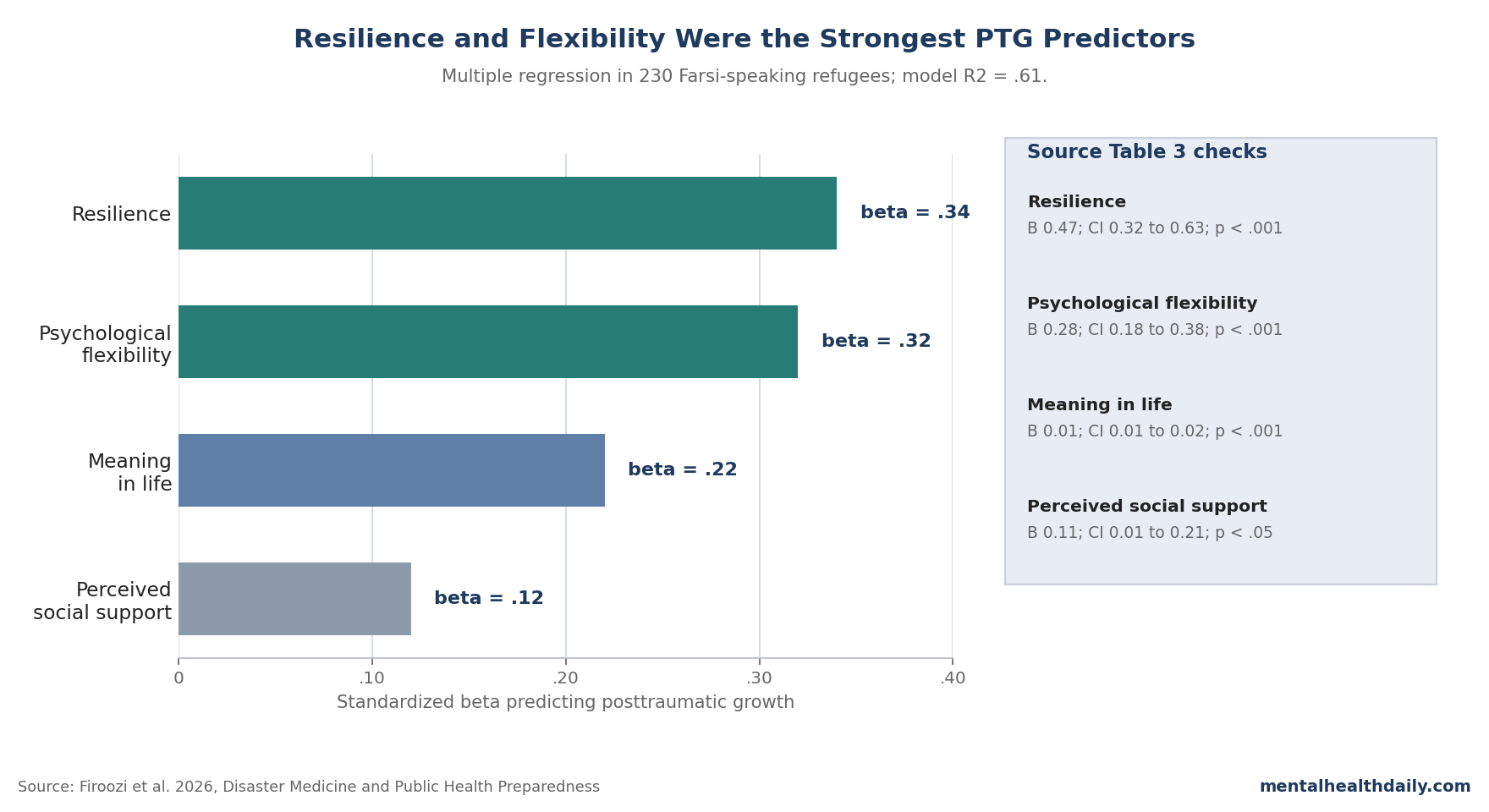
- Resilience carried the largest coefficient: resilience predicted posttraumatic growth with B = 0.47, 95% CI 0.32 to 0.63, standardized beta = 0.34, p < .001.1
- Flexibility and meaning were also substantial: psychological flexibility had standardized beta = 0.32, and meaning in life had standardized beta = 0.22; both were reported at p < .001.1
- Social support was real but smaller: perceived social support still predicted growth, but with a smaller standardized coefficient than resilience or psychological flexibility: B = 0.11, 95% CI 0.01 to 0.21, standardized beta = 0.12, p < .05.1
the calibrated interpretation is not that trauma produces growth, or that growth cancels psychological injury. The sharper finding is coexistence: a camp-based refugee sample showed very high distress burden and measurable growth-related resources at the same time.
Posttraumatic growth means positive psychological change after struggling with trauma, such as changed priorities, stronger relationships, spiritual change, personal strength, or new possibilities. In this paper, growth was not a diagnosis and not a treatment outcome; it was a self-reported adaptation construct measured beside symptom burden.
69.1% Screened High for Depression, Anxiety, and PTSD Symptoms
Firoozi et al. recruited 230 Farsi-speaking adults from refugee homes in Berlin and Brandenburg between August and November 2022.1 The sample included 137 men and 93 women, with a mean age of 30.6 years and an age range of 18–60.
The refugee-camp setting matters because this was not a settled community sample with stable housing and low administrative pressure. Participants were living in shelters, and 40 additional people declined or returned incomplete questionnaires because they worried about the research purpose or possible consequences for residence permits.
The distress numbers were not mild. The mean RHS-15 score was 17.05 (SD 11.8), the median was 14, and the range ran from 0 to 56.
On the standard RHS-15 symptom cutoff, 159 participants scored ≥12. On the distress thermometer, 158 scored ≥5, and 8 people scored the maximum value of 10.1
RHS-15 is the Refugee Health Screener-15, a brief instrument developed to screen refugees for anxiety, depression, and PTSD symptoms. A positive screen is not the same thing as a structured clinical diagnosis, but in a shelter population it is a serious service-planning signal.
Women and Asylum Seekers Had Higher Distress Scores
The study also tested whether distress differed by sex and residency status. Female participants had significantly higher distress scores than male participants: distress-thermometer t = −12.03, df = 226.71, p = .001; RHS-15 t = −12.93, df = 129.75, p = .001.1
Residency status showed a similar pattern. Asylum seekers had higher distress scores than refugees with residence status: distress-thermometer t = 7.54, df = 228, p = .001; RHS-15 t = 8.53, df = 138.59, p = .001.1
That status gradient fits adjacent German refugee research. Belz et al. reported PTSD and comorbid depression in a German refugee reception-center sample, and Boettcher and Neuner linked insecure asylum status with worse mental-health conditions after resettlement.2
Satinsky et al. also found that refugees and asylum seekers in Europe often have high mental-health needs and uneven access to care.3
Protective Factors Explained 61% of Posttraumatic-Growth Variance
The posttraumatic-growth side of the paper came from a multiple linear regression using 4 predictors: resilience, psychological flexibility, meaning in life, and perceived social support. The model explained 61% of PTG variance.1
- Resilience: B = 0.47, 95% CI 0.32 to 0.63, SE = 0.07, standardized beta = 0.34, p < .001.
- Psychological flexibility: B = 0.28, 95% CI 0.18 to 0.38, SE = 0.04, standardized beta = 0.32, p < .001.
- Meaning in life: B = 0.01, 95% CI 0.01 to 0.02, standardized beta = 0.22, p < .001.
- Perceived social support: B = 0.11, 95% CI 0.01 to 0.21, SE = 0.05, standardized beta = 0.12, p < .05.
Standardized betas make the ranking easier to read because the scales used different units. Resilience and psychological flexibility were nearly tied at the top.
Meaning in life was still clearly associated with growth. Perceived social support was statistically significant, but the coefficient was smaller than the personal psychological-resource measures.
Psychological Flexibility Needs a Careful Read
Psychological flexibility means being able to experience difficult thoughts and emotions without organizing life around avoidance, while still acting according to values. The study measured this domain with the Acceptance and Action Questionnaire-II (AAQ-II), a scale often described as measuring psychological inflexibility or experiential avoidance.8
Firoozi et al. discussed the predictor as psychological flexibility, and the regression table labeled it as flexibility. The safest interpretation is therefore directional but cautious: the flexibility-related measure was strongly associated with posttraumatic growth, but the cross-sectional design does not prove that increasing flexibility would cause growth to rise.
This matters for treatment translation. Acceptance and commitment therapy (ACT) targets psychological flexibility, but the Firoozi paper did not test ACT, did not randomize participants to therapy, and did not follow refugees over time.
The regression can justify interest in flexibility-focused care; it cannot prove that a flexibility intervention would reproduce the same coefficient.
Social Support Was Weaker Than the Personal-Resource Predictors
Social support often gets treated as the obvious refugee-protection variable. This paper complicates that easy version.
Perceived social support predicted posttraumatic growth, but its standardized beta was 0.12, smaller than resilience, psychological flexibility, and meaning in life.1
The result does not establish social support is unimportant. It means that, in this sample, support as perceived by the participant was a weaker statistical predictor of posttraumatic growth than the internal resources measured by the other scales.
Firoozi et al. also noted that social-support scores were relatively low, which makes sense in a refugee-camp sample where family separation, lost networks, and insecure residence status can make ordinary relationship resources harder to access.
Adjacent work points in the same general direction without making social support disappear. Walther et al. found that adult refugees in Germany described resilience and social support as adaptation resources.4
Kheirallah et al. studied Syrian refugee women and treated social support and posttraumatic growth as part of the same conflict-trauma mental-health landscape.5 Fisseha et al. separately modeled resilience as a mediator between post-migration adversity and refugee/asylum-seeker mental health.6
Posttraumatic Growth Is Not the Opposite of PTSD
One common mistake is to place PTSD symptoms and posttraumatic growth on opposite ends of the same line. Firoozi et al. are better read as evidence against that simple line.
The same sample had high distress screens and moderate posttraumatic growth.
Tedeschi and Calhoun’s PTG model allows distress and growth to coexist, which is exactly why this paper measured both rather than treating growth as a marker that symptoms were absent.9 Mangelsdorf and Eid also connected growth with meaning, social support, and positive emotional processes across intense-event contexts, supporting the broader idea that growth is a process domain, not a clean replacement for suffering.7
Clinically, that means posttraumatic growth should not be used as a sentimental label for refugee endurance. A refugee can report meaning, new priorities, spiritual change, or personal strength while still needing treatment for PTSD symptoms, depression, anxiety, sleep disturbance, legal stress, or unsafe housing.
Limits of the Firoozi Refugee-Camp Study
Cross-sectional timing: all measures were collected at one time point. The regression cannot show whether resilience produced growth, growth strengthened resilience, or a third factor influenced both.
Camp-based sampling: participants came from refugee homes in Berlin and Brandenburg. Findings may not generalize to Farsi-speaking refugees in private housing, later integration stages, other German states, or other countries.
Self-report and trust: all main constructs came from questionnaires. In a population where some people feared participation could affect residence status, self-report may reflect trust, language, perceived safety, and cultural fit as well as the target constructs.
Growth is not a treatment endpoint here: the study suggests which factors are associated with PTG, but it does not test whether strengthening those factors changes PTSD, depression, anxiety, or posttraumatic growth over time.
Questions Refugees, Clinicians, and Policy Teams Ask
Does the 69.1% number mean 69.1% had diagnosed PTSD, anxiety, or depression?
No. It means 159 of 230 participants crossed the RHS-15 screening threshold for depression, anxiety, and PTSD symptoms.
A screen is not a structured diagnostic interview, but it is a strong signal that camp-based Farsi-speaking refugees need accessible mental-health assessment and care.1
How should I read the 61% regression number?
The 4-factor model explained 61% of variance in PTGI scores within this sample. That is a large association for psychosocial data, but it is not a causal estimate because the study measured predictors and posttraumatic growth at the same time.1
Why did social support look weaker than resilience and flexibility?
The paper measured perceived social support, not objective network size. In refugee shelters, relationships may exist but still fail to feel usable, safe, or sufficient.
The regression model found that support was significant, but its standardized beta = 0.12 was smaller than resilience beta = 0.34 and psychological flexibility beta = 0.32.1
Does this support ACT or meaning-centered therapy for refugees?
It supports testing those approaches, not assuming they work. The flexibility and meaning coefficients make ACT-style and meaning-focused interventions plausible candidates, but randomized or longitudinal studies are needed before the Firoozi associations can be translated into treatment effects.
Should clinicians encourage posttraumatic growth directly?
Carefully. Clinicians can support meaning-making, flexible coping, social reconnection, and resilience without implying that trauma is beneficial or that refugees are supposed to grow from it.
Growth language becomes harmful when it minimizes distress, asylum insecurity, poverty, family separation, or untreated PTSD symptoms.
Are these findings specific to Farsi-speaking refugees in Germany?
The exact estimates should be treated as sample-specific: 230 Farsi-speaking adults from Iran and Afghanistan in Berlin/Brandenburg refugee shelters. The broader pattern — distress plus resilience-related adaptation — is consistent with adjacent refugee research, but service design should still be culturally and locally adapted.4,6
References
- Mental Health and Posttraumatic Growth of Farsi-Speaking Refugees in Germany: A Cross-Sectional Study. Firoozi AA, Yilmaz-Aslan Y, Brzoska P. Disaster Medicine and Public Health Preparedness. 2026;20:e96. doi:10.1017/dmp.2026.10363
- Posttraumatic stress disorder and comorbid depression among refugees: assessment of a sample from a German refugee reception center. Belz M et al. Transcultural Psychiatry. 2017;54(5-6):595–610. doi:10.1177/1363461517745473
- Mental health care utilisation and access among refugees and asylum seekers in Europe: a systematic review. Satinsky E et al. Health Policy. 2019;123(9):851–863. doi:10.1016/j.healthpol.2019.02.007
- A qualitative study on resilience in adult refugees in Germany. Walther L et al. BMC Public Health. 2021;21:828. doi:10.1186/s12889-021-10817-6
- The association of conflict-related trauma with markers of mental health among Syrian refugee women: the role of social support and post-traumatic growth. Kheirallah KA et al. International Journal of Women’s Health. 2022;14:1251–1266. doi:10.2147/IJWH.S360465
- Post-migration life adversity and mental health of refugees and asylum seekers: the mediating role of resilience between perceived discrimination, socio-economic strains, structural strains, and mental health. Fisseha IF et al. Behavioral Sciences. 2022;12(7):208. doi:10.3390/bs12070208
- What makes a thriver? Unifying the concepts of posttraumatic and postecstatic growth. Mangelsdorf J, Eid M. Frontiers in Psychology. 2015;6:813. doi:10.3389/fpsyg.2015.00813
- Preliminary psychometric properties of the Acceptance and Action Questionnaire-II: a revised measure of psychological inflexibility and experiential avoidance. Bond FW et al. Behavior Therapy. 2011;42(4):676–688. doi:10.1016/j.beth.2011.03.007
- The Posttraumatic Growth Inventory: measuring the positive legacy of trauma. Tedeschi RG, Calhoun LG. Journal of Traumatic Stress. 1996;9(3):455–471. doi:10.1002/jts.2490090305