A 2026 DIVERGE analysis of 3,677 antidepressant-exposed patients with major depressive disorder in Pakistan classified 34% as treatment resistant, while 86% received psychotropic polypharmacy and only 6% received psychotherapy.1 The CYP2C19 signal is real enough to study prospectively, but the main treatment-system finding is medication stacking in a setting where psychological care was rare.
Research Highlights
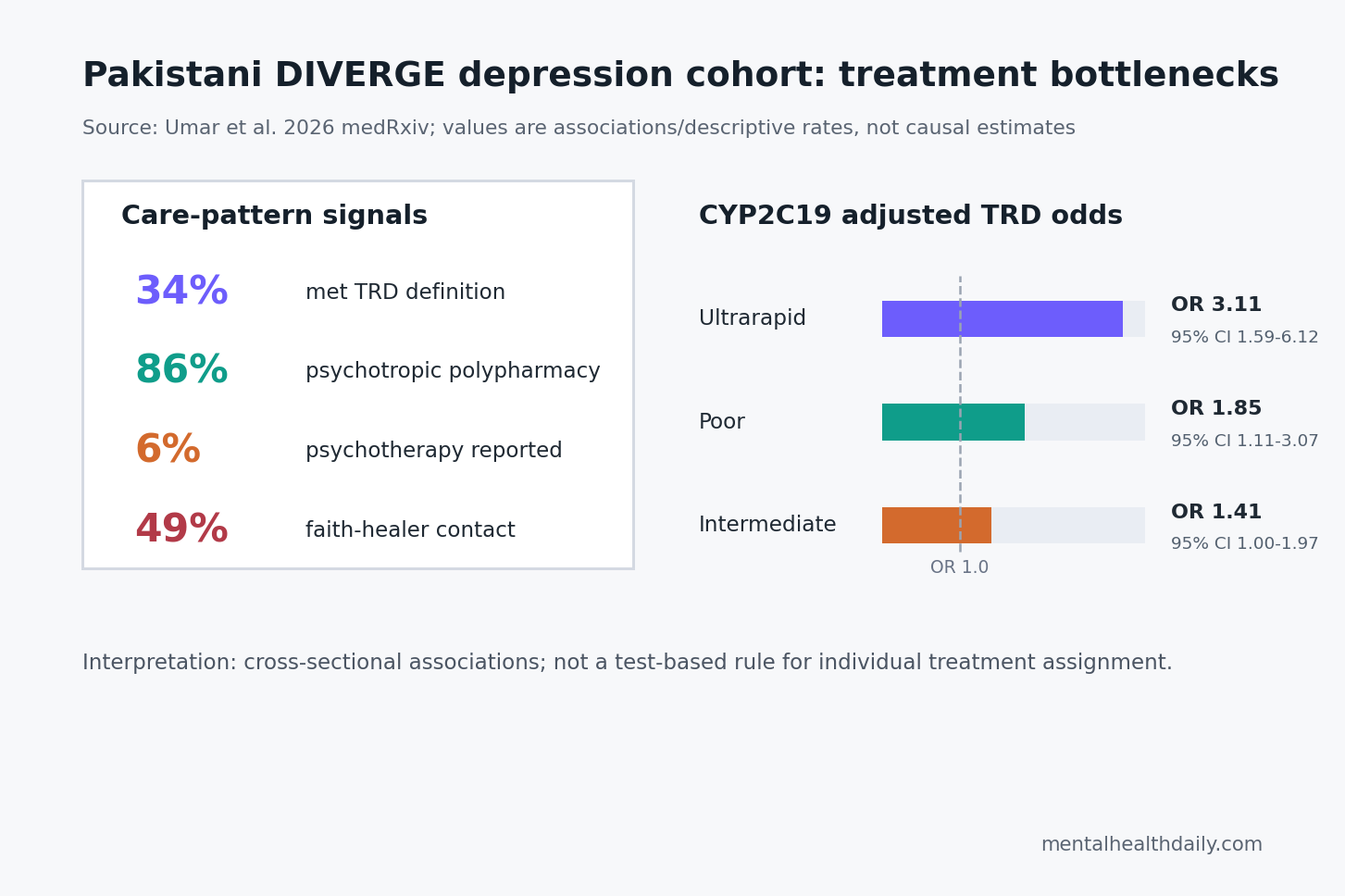
- TRD was common: 1,265 of 3,677 eligible treated patients met the DIVERGE definition of treatment-resistant depression, or 34% (95% CI 32% to 36%).1
- Medication stacking dominated care: 86% received at least 1 additional psychotropic drug with an antidepressant, including 29% on multiple antidepressants and 52% on antidepressant-plus-antipsychotic or mood-stabilizer augmentation.1
- Psychotherapy was scarce: only 6% reported psychotherapy, while 49% had visited a religious leader or faith healer for mental-health problems.1
- Social support carried the largest non-drug signal: strong support was associated with lower TRD odds, OR = 0.55 (95% CI 0.44 to 0.69; p = 1.4 x 10-7).1
- CYP2C19 needs calibration: ultrarapid metabolizer status was associated with higher TRD odds, OR = 3.11 (95% CI 1.59 to 6.12), but the pharmacogenetic analysis was cross-sectional and did not prove a test-based treatment rule.1
Treatment-resistant depression usually means major depressive disorder that has not responded to adequate antidepressant treatment. Many observational studies define it as failure of 2 adequate antidepressant trials from different classes, but Umar et al. used a pragmatic Pakistani psychiatric-care definition: minimal or no symptom relief after at least 12 weeks of adherent antidepressant therapy.1
That definition matters because the local prescribing pattern made the classic 2-trial definition hard to apply. Only 14% of the eligible patients received a single antidepressant alone. Most were already receiving additional psychotropic medication, so “failed 2 clean antidepressant trials” did not map cleanly onto the care actually recorded in the clinics.
3,677 Treated Patients Made Up the TRD Analysis
DIVERGE, short for Depression in Diverse Populations: Unravelling the Interplay Between Genes and Environment, recruited adults with major depressive disorder from psychiatric care facilities across Pakistan between September 27, 2021, and June 30, 2025. The parent dataset included 13,393 participants, with 9,278 major-depression cases and 4,115 controls.1
When the researchers ran the treatment-response analysis, 8,360 depression cases were available. Of those, 1,954 patients, or 23%, were medication naive and excluded from the TRD analysis. Among 6,406 patients with medication history, adherence was reported as good in 41%, moderate in 57%, and poor in 2%. The final TRD-eligible sample included 3,677 patients.1
Sample shape: the cohort was 56% female, mean age was 38 years, mean depression onset was 30 years, and average illness duration was 7 years. Comorbidity was common: 32% had another psychiatric condition and 42% had a physical comorbidity, including gastrointestinal disorders in 17% and hypertension in 15%.1
86% Received Psychotropic Polypharmacy With Antidepressants
Psychotropic polypharmacy means prescribing more than 1 medication that affects the brain or mental state. In this DIVERGE analysis, it was not a marginal pattern. Among 3,677 TRD-eligible treated patients, 86% received another psychotropic drug with an antidepressant, including another antidepressant, a mood stabilizer, an antipsychotic, an anxiolytic, or a benzodiazepine.1
Combination antidepressant therapy appeared in about 29% of eligible patients. Augmentation therapy, defined as an antidepressant plus a mood stabilizer or antipsychotic, appeared in 52%. Even medication-naive patients were often started on multi-drug regimens: 84% received a second psychotropic drug, and 39% received antidepressant-plus-antipsychotic or mood-stabilizer augmentation.1
Umar et al. compared this pattern with prior high-income prescribing data: antipsychotic adjunctive use in their sample was 47%, compared with 3% in UK primary care and 14% to 21% in US-based studies.1 That comparison does not prove the Pakistani prescribing pattern caused TRD. It shows that imported TRD definitions and treatment assumptions can break when the baseline care environment is different.
Psychotherapy Was 6%, While Faith-Healer Contact Was 49%
Non-drug care showed the opposite imbalance. Only about 6% of patients reported psychotherapy, and psychotherapy was more common in non-TRD patients than TRD patients, 7% vs. 4% (p = 0.0003). Electroconvulsive therapy was also reported by about 6%.1
Faith-healer or religious-leader contact was much more common: 49% of patients had visited a religious leader or faith healer in relation to mental-health problems. The useful clinical read is not to mock or romanticize that pattern. In a setting with constrained psychotherapy access, cultural help-seeking and family support may be part of the actual care pathway even when they sit outside formal psychiatric treatment.
Psychotherapy access is relevant because treatment-resistant depression care involves more than medication sequencing. Rogan and Wilkinson reviewed psychotherapy’s role in TRD management, and many high-income guidelines still recommend combining medication strategies with evidence-based psychological care when depression persists.5 DIVERGE suggests that the Pakistani treatment environment may have had much more medication intensification than structured psychotherapy.
Social Support Was Linked to Lower TRD Odds
The strongest non-drug association was social support. Compared with poor support, moderate support was associated with lower TRD odds, OR = 0.64 (95% CI 0.53 to 0.76), and strong support was associated with OR = 0.55 (95% CI 0.44 to 0.69).1
Oslo Social Support Scale scores measure perceived support, including available help and social ties. The researchers checked whether higher support scores reflected real support structures rather than only mood-biased reporting. Moderate or high support was much more frequent when relatives lived in the same area compared with no relatives, OR = 4.20 (95% CI 3.60 to 4.95; p = 3.9 x 10-71). Larger household structure also tracked higher perceived support.1
Family-structure signal: parents being first cousins was associated with lower TRD odds, OR = 0.81 (95% CI 0.69 to 0.96), but that should not be read as a biological protection claim. Umar et al. interpreted it through possible family-structure and support pathways.1
The cross-sectional design cannot separate cultural support, family proximity, illness severity, treatment access, and genetic explanations.
Divorce or separation moved in the opposite direction. Compared with married patients, divorced or separated patients had higher TRD odds, OR = 1.81 (95% CI 1.18 to 2.78). Psychotic symptoms were also associated with TRD, OR = 1.37 (95% CI 1.04 to 1.82), and suicidal behavior score was associated with TRD, OR = 1.03 (95% CI 1.01 to 1.05).1
CYP2C19 Was Associated With TRD, But CYP2D6 Was Not
CYP2C19 and CYP2D6 are liver-enzyme genes that affect how quickly many antidepressants and other psychiatric drugs are metabolized. A poor metabolizer may have higher drug exposure at a standard dose, while an ultrarapid metabolizer may clear some drugs faster and receive less exposure than intended.
In DIVERGE, star-allele and metabolizer phenotype data were available for 3,217 participants, and 1,085 overlapped with the TRD-eligible sample. CYP2C19 poor metabolizers were 8% of the Pakistani sample, compared with 13% in East Asian and 2% in European comparator frequencies cited by the researchers.1
Provincial differences: CYP2C19 ultrarapid metabolizers were 5.6% in Khyber Pakhtunkhwa vs. 1.5% in Sindh, while poor metabolizers were 10.5% in Punjab vs. 5.6% in Khyber Pakhtunkhwa.1
CYP2C19 metabolizer status was associated with TRD in the adjusted pharmacogenetic model:
- Poor metabolizer: OR = 1.85, 95% CI 1.11 to 3.07, p = 0.018.
- Intermediate metabolizer: OR = 1.41, 95% CI 1.00 to 1.97, p = 0.048.
- Ultrarapid metabolizer: OR = 3.11, 95% CI 1.59 to 6.12, p = 0.001.
CYP2D6 metabolizer status showed no evidence of association with TRD. The paper also found no evidence that currently reported side effects were linked to CYP2C19 or CYP2D6 status, though side-effect data were not available across the full illness course.1
Pharmacogenetics Explains Exposure Better Than TRD Prediction
The CYP2C19 result is biologically plausible. Milosavljevic et al. found that CYP2C19 and CYP2D6 poor and intermediate metabolizer status were associated with antidepressant and antipsychotic exposure differences, and CPIC guidelines now include genotype-based recommendations for several serotonin reuptake inhibitors.3,4
The calibration is that exposure is not the same as outcome prediction. A genotype can affect drug level, tolerability, and dose fit without automatically determining whether a patient becomes treatment resistant. Umar et al. explicitly noted that other large studies failed to identify a consistent CYP2C19-antidepressant-response association in major depression.1
Clinical implication: the DIVERGE CYP2C19 signal should justify prospective pharmacogenetic studies in Pakistani depression care. It should not be inflated into a claim that CYP2C19 testing can now diagnose or prevent TRD by itself.
High-Income TRD Evidence Does Not Transfer Cleanly
Fabbri et al. used UK primary-care records to study genetic and clinical characteristics of treatment-resistant depression, while Lundberg et al. used population-wide data to connect TRD with worse outcomes and greater health-care utilization.2,6 Those studies help show why TRD matters: persistent nonresponse is not a cosmetic label; it tracks disease burden, service use, and later risk.
DIVERGE adds a different layer. South Asian and low- or middle-income settings have been underrepresented in TRD predictor studies, and Pakistani psychiatric care has distinctive access constraints, family structures, prescribing cultures, and pharmacogenetic frequencies. A predictor model trained in UK records or a treatment algorithm built around high-income psychotherapy access may not describe the same clinical problem.
Evidence-strength note: the Umar paper is a medRxiv preprint, and the analysis was cross-sectional. It can identify who had TRD and what was associated with it inside the DIVERGE sample. It cannot prove that polypharmacy, low psychotherapy exposure, low social support, divorce/separation, psychotic symptoms, suicidal behavior, or CYP2C19 status caused treatment resistance.
Questions About TRD in Pakistan and CYP2C19
Did this study use the standard 2-failed-antidepressant TRD definition?
No. Umar et al. defined TRD as minimal or no symptom relief after at least 12 weeks of adherent antidepressant therapy. They used this definition because heavy psychotropic polypharmacy made clean 2-trial sequencing hard to reconstruct in a retrospective cross-sectional dataset.1
Does 34% mean 34% of all depression patients in Pakistan have TRD?
No. The denominator was 3,677 antidepressant-exposed, TRD-eligible patients presenting to psychiatric care facilities. It does not estimate national population prevalence or primary-care prevalence.
Should Pakistani patients get CYP2C19 testing based on this paper?
The paper supports more prospective testing of pharmacogenetics in Pakistani depression care. It does not prove that CYP2C19 testing alone should guide treatment or predict individual TRD risk.
Why is psychotherapy access part of the TRD story?
TRD is often discussed as a medication problem, but persistent depression care can involve psychotherapy, adherence support, safety monitoring, family support, medication review, and treatment sequencing. In DIVERGE, only 6% reported psychotherapy, while medication stacking was common.
What should readers take from the Pakistan DIVERGE TRD data?
Pakistan-specific TRD research needs to study treatment sequencing, psychotherapy access, social support, and pharmacogenetics together. The DIVERGE data suggest that importing high-income TRD assumptions without checking local care patterns would miss much of the signal.
References
- Umar M, Hussain F, Khizar B, et al. Understanding response to treatment in depression: Insights from the Pakistani DIVERGE study. medRxiv. 2026. doi:10.64898/2026.04.13.26350625
- Fabbri C, Hagenaars SP, John C, et al. Genetic and clinical characteristics of treatment-resistant depression using primary care records in 2 UK cohorts. Molecular Psychiatry. 2021;26(7):3363–3373. doi:10.1038/s41380-021-01062-9
- Milosavljevic F, Bukvic N, Pavlovic Z, et al. Association of CYP2C19 and CYP2D6 poor and intermediate metabolizer status with antidepressant and antipsychotic exposure: A systematic review and meta-analysis. JAMA Psychiatry. 2021;78(3):270–280. doi:10.1001/jamapsychiatry.2020.3643
- Bousman CA, Stevenson JM, Ramsey LB, et al. Clinical Pharmacogenetics Implementation Consortium guideline for CYP2D6, CYP2C19, CYP2B6, SLC6A4, and HTR2A genotypes and serotonin reuptake inhibitor antidepressants. Clinical Pharmacology & Therapeutics. 2023;114(1):51–68. doi:10.1002/cpt.2903
- Rogan T, Wilkinson ST. The role of psychotherapy in the management of treatment-resistant depression. Psychiatric Clinics of North America. 2023;46(2):349–358. doi:10.1016/j.psc.2023.02.006
- Lundberg J, Cars T, Loov SA, et al. Association of treatment-resistant depression with patient outcomes and health care resource utilization in a population-wide study. JAMA Psychiatry. 2023;80(2):167–175. doi:10.1001/jamapsychiatry.2022.3860