
A 2026 mixed-methods study of 32 chronic non-cancer pain patients found the strongest satisfaction signal when prescribed cannabis-based medicines affected stress, sleep, coping, anxiety, appetite, and daily function — not pain intensity alone.1
Research Highlights
- 32 patients were interviewed: Pombeiro Stein et al. studied adults from a German pain clinic who had used physician-prescribed cannabis-based medicines for at least 6 months.1
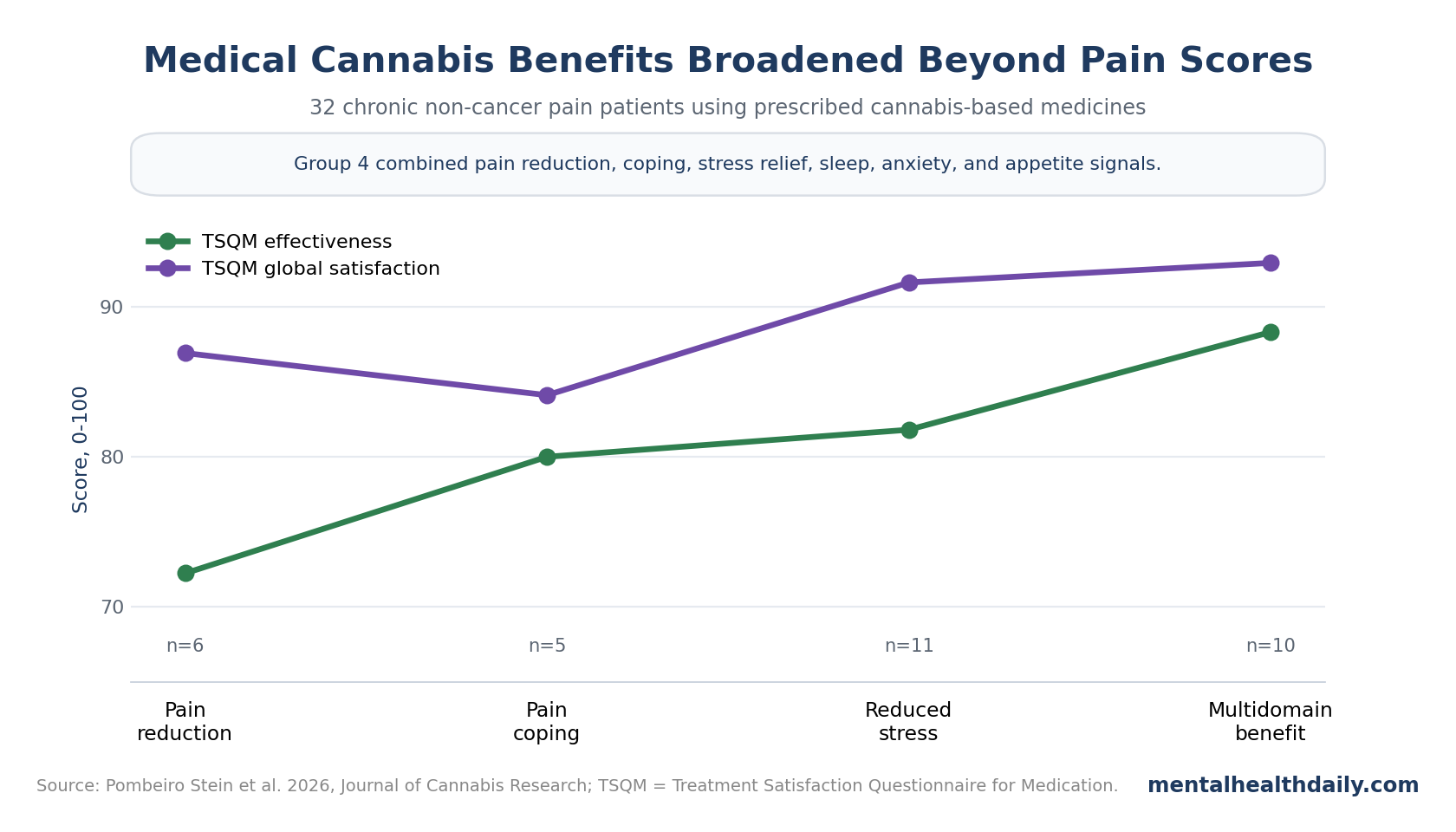
- 4 response patterns emerged: interviews separated patients into pain-reduction, pain-coping, reduced-stress, and multidimensional-benefit groups.1
- Satisfaction tracked breadth: the multidimensional group had the highest Treatment Satisfaction Questionnaire for Medication global satisfaction score, 92.9 out of 100.1
- Pain-only measurement looked incomplete: 94% scored at least 70 on global satisfaction, while patients described effects on stress management, sleep quality, relaxation, anxiety, appetite, and family or work function.1
- Side effects were easy to undercount: 29 of 32 patients spontaneously discussed side effects in interviews, and 15 who did not report TSQM side effects still described issues such as cognitive impairment or fatigue.1
Cannabis-based medicines are prescribed cannabinoid products such as medical cannabis flowers, extracts, dronabinol, or nabiximols-like preparations used under medical supervision. The important claim here is not that cannabis broadly “works” for chronic pain; it is that chronic-pain benefit may be misread when trials measure pain intensity while patients judge treatment by coping, stress, sleep, mood, and function.
32 Chronic-Pain Patients Described 4 Cannabis Response Patterns
Pombeiro Stein et al. recruited patients from the Hannover Medical School Pain Clinic after they had used prescribed cannabis-based medicines for at least 6 months. The researchers used semi-structured interviews plus the Treatment Satisfaction Questionnaire for Medication (TSQM), a 0-100 medication-satisfaction scale covering effectiveness, side effects, convenience, and global satisfaction.1
Grounded theory is a qualitative method that builds categories from interviews instead of forcing responses into a preselected checklist. In this study, the researchers coded interviews until theoretical saturation, meaning new interviews were no longer adding major new themes.
The 4 groups were clinically different:
- Pain reduction: 6 patients mainly described lower pain intensity.
- Pain coping: 5 patients described pain still being present but easier to live with, distance from pain, or better management.
- Reduced stress: 11 patients described pain changes plus relaxation, calming, and stress reduction.
- Multidimensional benefit: 10 patients described pain reduction, coping, stress reduction, sleep improvement, lower anxiety, appetite changes, and broader quality-of-life gains.
That ordering is the center of the result. Patients who only described pain intensity were not the most satisfied group. The highest satisfaction appeared when the medicine changed several parts of the chronic-pain system at once.
Stress, Sleep, and Coping Carried the Highest Satisfaction Signal
Chronic non-cancer pain means persistent pain not caused by active cancer. It often behaves less like a single injured tissue and more like a whole-system disorder involving pain sensitivity, sleep disruption, fear, avoidance, stress physiology, and mood.
Pombeiro Stein et al. interpreted the interview pattern through a biopsychosocial model. Biopsychosocial pain means pain is shaped by biological factors, psychological factors, and social context at the same time. That model fits chronic primary pain and nociplastic pain, where the nervous system can amplify pain even when tissue damage is not enough to explain the symptom burden.
The TSQM results matched that broader framing:
- 94% of participants scored ≥70 for global satisfaction.
- 59% scored ≥90 for global satisfaction.
- 83% scored ≥70 for effectiveness.
- 81% scored ≥80 for side-effect tolerability.
When TSQM scores were linked back to the 4 interview groups, the multidimensional group had the highest global satisfaction score at 92.9 and the highest effectiveness score at 88.3. The pain-reduction group had an effectiveness score of 72.25, while the pain-coping group had the lowest global satisfaction score at 84.1.1
The pattern is not proof of causality. Patients were not randomized into response groups, and group assignment came from interviews. Still, the data explain why a trial can show a modest pain-intensity effect while some patients report a large life effect: the life effect may be distributed across sleep, stress, appetite, anxiety, body relaxation, and willingness to move or work.
Pain Intensity Alone Can Miss the Patient-Reported Benefit
Randomized trials of cannabis-based medicines for chronic pain have produced uneven results. Products differ by tetrahydrocannabinol (THC), cannabidiol (CBD), route, dose, duration, and pain condition. Outcomes also differ: some trials emphasize pain intensity, while others measure sleep, function, global impression, or adverse events.
A 2021 BMJ systematic review of medical cannabis or cannabinoids for chronic pain found modest average benefits, but the evidence was limited by product heterogeneity and adverse effects such as dizziness, sedation, and cognitive symptoms.3 That evidence does not support a simple “cannabis is a strong analgesic” claim.
Longer observational studies often sound broader. Bialas et al. reviewed long-term observational studies involving around 2,500 chronic non-cancer pain patients and reported improvements across pain intensity, function, sleep quality, depression, anxiety, and general quality of life. Around 16% of patients stopped opioid medication during cannabis-based-medicine therapy.2
The useful calibration is direct:
- Randomized-trial signal: average pain reduction is usually modest, product-dependent, and limited by adverse effects.
- Patient-experience signal: some patients describe broader changes in coping, sleep, stress, anxiety, and function.
- Measurement problem: a pain-intensity endpoint can miss a benefit that operates through the emotional and functional load of pain.
This does not make qualitative interviews stronger than randomized trials. It makes them useful for choosing better trial endpoints. A trial that measures only daily pain score may miss whether a patient sleeps through more nights, uses fewer rescue medications, avoids less activity, or feels less threatened by pain.
Medical Cannabis Looked More Like a Coping Drug Than a Pure Analgesic
Pleiotropy means 1 substance has several effects across different systems. Cannabis-based medicines plausibly fit that word because cannabinoid receptors are involved in pain processing, stress biology, reward, appetite, sleep, memory, and autonomic regulation.
In the Pombeiro Stein et al. interviews, patients repeatedly described effects that were adjacent to pain rather than identical to pain relief. Reduced stress, muscle relaxation, falling asleep, fewer fear-driven limitations, and a more positive morning state were part of the reported benefit package.1
That pattern matches older qualitative work. Lavie-Ajayi and Shvartzman interviewed chronic-pain patients and described a “restored self” theme: cannabis could change the relationship to pain, identity, and daily participation even when pain did not disappear.4 Piper et al. also found that medical-cannabis users reported substituting cannabis for medications used for pain, anxiety, migraine, and sleep.5
The clinical interpretation should stay bounded. A patient saying “I cope better” is not the same as a blinded trial showing a large analgesic effect. It is also not meaningless. For chronic pain, coping, sleep, and stress are part of the disease burden.
Best endpoint set: future trials should measure pain intensity, function, sleep, anxiety, stress, rescue-medication use, driving limitation, cognitive side effects, and global impression at the same time. That would test the multidomain hypothesis without pretending that interviews alone prove it.
Side Effects Were Reported Differently in Interviews vs. Questionnaires
Side-effect reporting was one of the most useful parts of the study because the 2 methods disagreed. Most patients, 29 of 32, spontaneously mentioned side effects in interviews. Yet 15 of 32 did not report side effects in the TSQM while still describing cognitive impairment, fatigue, dry mouth, dizziness, inner tension, or gastrointestinal symptoms in interviews.1
That mismatch has a practical explanation. Patients may notice side effects but not count them as medication problems if the side effect feels tolerable, expected, or smaller than the benefit. A questionnaire can then underestimate the real cognitive or fatigue load.
The most relevant safety domains in this paper were not exotic:
- Cognitive impairment: 10 patients described it despite some not listing TSQM side effects.
- Fatigue: 5 patients described tiredness or sedation-type effects.
- Dry mouth: 4 patients described it.
- Driving limits: restricted ability to drive lowered global satisfaction.
- Stigma and access: some patients described bureaucracy, cost coverage barriers, and being labeled negatively for medical cannabis use.
Those details are clinically more actionable than a generic “well tolerated” label. Medical cannabis may be acceptable to a patient and still cause cognitive slowing, fatigue, driving restrictions, or stigma that should be monitored directly.
Evidence Strength: Hypothesis-Generating, Not Practice-Changing
This study is useful because it explains a measurement problem. It is not a reason to start cannabis-based medicines broadly for chronic pain.
What the design can support: the study can show how a small, supervised chronic-pain sample described cannabis-based-medicine effects after at least 6 months of use, and how those descriptions lined up with medication-satisfaction scores.
What the design cannot support: it cannot prove that cannabis caused the multidimensional benefits, identify the best THC/CBD ratio, estimate addiction risk, compare cannabis with guideline pain treatments, or show that recreational use has the same profile.
The safest reading is that chronic-pain cannabis trials need better endpoint architecture. Pain intensity should stay in the trial, but it should not be the whole trial. If the hypothesized benefit is biopsychosocial, the measurement set has to be biopsychosocial too.
Questions About Medical Cannabis for Chronic Pain
Did this study show that medical cannabis reduces chronic pain?
Not by itself. It interviewed 32 patients already using prescribed cannabis-based medicines and linked their experiences to satisfaction scores. The study is hypothesis-generating, not causal proof.
What was the main signal?
The strongest satisfaction signal appeared when patients reported broader effects across pain coping, stress reduction, sleep, anxiety, appetite, and function. Pain reduction alone was not the highest-satisfaction pattern.
Does this conflict with randomized trials showing modest cannabis pain effects?
No. It helps explain the gap. Randomized trials often focus on pain intensity and adverse events, while satisfied chronic-pain patients may judge benefit through sleep, stress, function, and whether pain feels less consuming.
What should clinicians or patients monitor?
Track pain intensity, sleep, stress, anxiety, function, rescue-medication use, cognitive slowing, fatigue, driving restrictions, and stigma or access problems. A single pain score is too narrow for this kind of treatment claim.
References
- Pombeiro Stein ICA, Fitzner F, Dusch M, et al. The greater the pleiotropic effects, the greater the benefits – cannabis as a biopsychosocial drug: a mixed-methods study on chronic non-cancer pain. Journal of Cannabis Research. 2026;8:54. doi:10.1186/s42238-026-00440-w
- Bialas P, Fitzcharles MA, Klose P, Hauser W. Long-term observational studies with cannabis-based medicines for chronic non-cancer pain: a systematic review and meta-analysis of effectiveness and safety. European Journal of Pain. 2022;26:1221-1233. PubMed
- Wang L, Hong PJ, May C, et al. Medical cannabis or cannabinoids for chronic non-cancer and cancer related pain: a systematic review and meta-analysis of randomized clinical trials. BMJ. 2021;374:n1034. doi:10.1136/bmj.n1034
- Lavie-Ajayi M, Shvartzman P. Restored self: a phenomenological study of pain relief by cannabis. Pain Medicine. 2019;20:2086-2093. PubMed
- Piper BJ, DeKeuster RM, Beals ML, et al. Substitution of medical cannabis for pharmaceutical agents for pain, anxiety, and sleep. Journal of Psychopharmacology. 2017;31:569-575. doi:10.1177/0269881117699616
- Ng JY, Abrams A, Pathak A, Tahir U, Jomy J. What are the experiences of patients using cannabis for pain? A systematic review of qualitative studies. European Journal of Integrative Medicine. 2022;49:102098. doi:10.1016/j.eujim.2021.102098