Research Highlights
- Exercise works. Across the strongest available meta-analyses, regular exercise produces a moderate-to-large reduction in depression symptoms (SMD around −0.66 to −0.97) and a smaller but real reduction in anxiety (SMD around −0.66) — a clinically meaningful effect, in the same range as what antidepressants produce in trials.
- Cardio may be modestly better for depression; weight training modestly better for anxiety — but the difference isn’t statistically confirmed. Point estimates lean those directions in the most recent meta-analysis, but the formal between-group tests don’t reach significance (p = 0.591 for depression, p = 0.683 for anxiety). Optimal recommendation: do both. If you have to pick one, lean toward the type the data favors for your symptom — aerobic for depression, resistance for anxiety.
- Anxiety evidence is thinner than depression evidence. 11 trials in the most recent meta-analysis vs. 25 for depression. The signal is real, but with fewer studies backing it, the estimate is less precise.
- Studies disagree on size, not direction. Heterogeneity is high (I² above 85%) — individual trials disagree on how large the benefit is. The direction of effect (exercise reduces symptoms) is robust; the precise effect size is not.
- You don’t need to hit official guidelines. Only 3 of 30 trials met WHO weekly physical activity targets, yet meaningful clinical improvement was observed across the full set.
Exercise reduces depression and anxiety symptoms — that finding has held up across decades of meta-analyses. The trickier questions are by how much, in what form, and compared to what. Popular coverage tends to overstate the gap between cardio and resistance training, oversell exercise as a one-to-one substitute for antidepressants, and treat single-paper findings as settled science.
The Headline Numbers, Read Carefully
The most recent comprehensive synthesis is Banyard and colleagues’ 2025 systematic review and meta-analysis in the International Journal of Mental Health Nursing, which pooled 32 randomized controlled trials (3,243 participants), with 26 trials (2,681 participants) included in the quantitative meta-analyses.1 The headline pooled effects:
- Depression: SMD −0.97 (95% CI −1.28 to −0.66) across 25 studies — a large effect favoring exercise.1
- Anxiety: SMD −0.66 (95% CI −1.09 to −0.23) across 11 studies — a moderate effect.1
(SMD, or standardized mean difference, lets us compare studies that used different symptom scales. Negative numbers favor exercise. Rough benchmarks: 0.2 small, 0.5 moderate, 0.8 large. Antidepressants vs. placebo typically produce SMDs around 0.3–0.5. The 95% CI — confidence interval — is the range the true effect is likely to sit in; narrower means more precise.)
These numbers sit inside a remarkably stable historical band:
- Cooney 2013 (Cochrane): SMD −0.62 when restricted to higher-quality trials — the conservative reference point.2
- Schuch 2016: Large unadjusted effect that shrank to roughly moderate after correcting for publication bias (the tendency for small flattering studies to be over-represented in the literature).3
- Heissel 2023 (BJSM): Comprehensive review across 40+ trials with meta-regression on dose; effect again landed in the moderate-to-large range with a detectable dose-response gradient.4
The convergence matters. Different research groups, different inclusion criteria, different statistical adjustments — all yield effect sizes that are real and clinically meaningful.
The disagreement is over magnitude, not direction; the gap is mostly explained by how aggressively each analysis adjusts for publication bias.
Aerobic vs. Resistance Training: Both Work About Equally
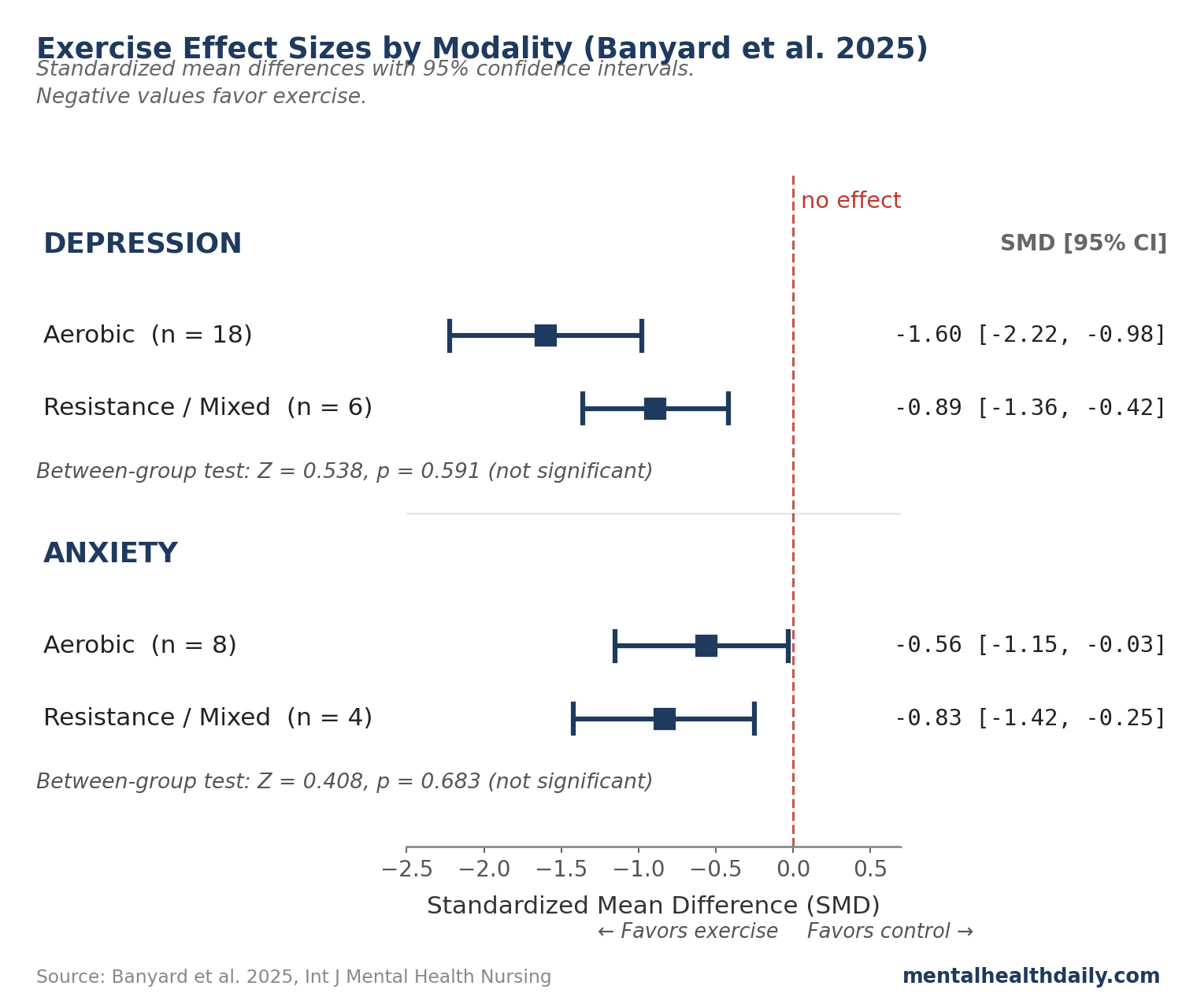
Banyard’s review ran subgroup analyses comparing aerobic to resistance/mixed exercise for both primary outcomes. Point estimates — best-guess effect sizes for each subgroup, before factoring in uncertainty — differ in the direction popular coverage emphasizes. For depression, aerobic studies (n = 18) yielded SMD −1.60 (CI −2.22 to −0.98), while resistance/mixed studies (n = 6) yielded SMD −0.89 (CI −1.36 to −0.42). For anxiety, the direction reversed: aerobic (n = 8) yielded SMD −0.56, while resistance/mixed (n = 4) yielded SMD −0.83.1
What rarely gets quoted is the formal between-subgroup test — the actual statistical question of whether aerobic and resistance differ from each other beyond what could be due to chance. The Z-statistic measures how many standard deviations a result sits from zero; values close to zero mean the difference is small or noisy, and |Z| above roughly 1.96 corresponds to p < 0.05.
- Depression between-group test: Z = 0.538, p = 0.591 — not significant.1
- Anxiety between-group test: Z = 0.408, p = 0.683 — not significant.1
Those p-values are nowhere near significance — the data don’t have enough power to confirm a difference between exercise types. But it would be an overcorrection to call them identical. The point estimates lean in directions worth taking seriously:
- For depression, both types clearly beat control (aerobic Z = 4.74, p < 0.001; resistance/mixed Z = 3.72, p < 0.001). The point-estimate gap (−1.60 vs. −0.89) suggests aerobic may be modestly stronger, but isn’t formally distinguishable from resistance.
- For anxiety, only resistance/mixed clearly beat control (Z = 2.79, p = 0.005). Aerobic alone did not (Z = 1.88, p = 0.090). The point-estimate gap (−0.83 vs. −0.56) plus the within-subgroup pattern both suggest resistance is the safer bet for anxiety.
Banyard’s own discussion is careful: “the mode of exercise prescription did not influence the beneficial effect” on depression, with “some influence on anxiety symptoms.” Gordon and colleagues’ 2018 meta-analysis in JAMA Psychiatry, examining resistance training across 33 trials, found an overall effect of SMD around −0.66 for depression — well within the range from aerobic-heavy reviews.5
The practical read: exercise reliably reduces symptoms; the differences between exercise types claimed in trade press are real as directional signals but overstated as confirmed differences. Six of the 32 trials in Banyard’s review prescribed a combined aerobic + resistance protocol, and those mixed studies worked well.
Optimal strategy: do both. If time, energy, or preference forces a single choice, lean toward what the data favors for your symptom — aerobic for depression, resistance for anxiety — with the understanding that either is much better than nothing, and that sticking with it matters more than which type you pick.
How Exercise Compares to Antidepressants
The most direct head-to-head data come from the SMILE and SMILE-II trials by Blumenthal and colleagues, included in Banyard’s review.6 In SMILE-II, supervised aerobic exercise produced remission rates broadly comparable to sertraline (an SSRI, the most commonly prescribed class of antidepressants) at 16 weeks in adults with major depressive disorder, though the medication showed a faster onset of action. Older patients in the original SMILE trial showed similar parity at four months, with exercise associated with lower relapse rates at ten-month follow-up.7
For context, modern meta-analyses of SSRIs versus placebo find SMDs in the range of approximately −0.30 to −0.50 for depressive symptoms in adults with major depression, depending on the agent and outcome scale.8 So the claim that exercise produces effects in the same order of magnitude as antidepressants is defensible. The stronger claim that exercise matches or beats antidepressants requires more caveats than it usually receives:
- Different participants enroll in exercise trials than in pharmacotherapy trials.
- Blinding is impossible in exercise interventions — participants know whether they’re exercising, which can inflate apparent effects.
- Most exercise trials excluded patients with severe or psychotic depression, where pharmacotherapy’s edge over alternatives is largest.
The clinical read: for mild to moderate depression, exercise is in the same evidentiary tier as first-line antidepressant treatment. For severe depression, the comparison breaks down, and exercise is best treated as an add-on rather than a replacement.
Why Exercise Helps: The Mechanisms
Several biological pathways are routinely invoked. Each is supported by correlational human data and animal models. None has been shown to be the mechanism whose blockade abolishes the clinical effect.
- BDNF and hippocampal growth. Aerobic exercise raises BDNF (brain-derived neurotrophic factor — a growth factor for brain cells). Erickson and colleagues showed one year of aerobic training in older adults grew hippocampal volume by ~2%, effectively reversing a year of normal age-related shrinkage.9
- Stress-system regulation. Exercise normalizes the HPA axis (the body’s main stress-response system), lowering basal cortisol and restoring its daily rhythm in depressed populations.10
- Anti-inflammatory effects. Inflammatory cytokines such as IL-6 and TNF-alpha, elevated in a subset of depressed patients, are reduced by exercise. Whether this reduction causes mood improvement or merely co-occurs with it remains an open question.
- Other plausible pathways. Endocannabinoid signaling, central serotonin tone, and shifts in brain-network connectivity have all been implicated, with consistent biochemical signals but inconsistent translation to clinical outcomes.
Multiple mechanisms acting in parallel is the most defensible reading. Anyone claiming a single clean explanation has read past the data.
Where the Evidence Falls Short
Several limitations cut across nearly every meta-analysis in this area, and any rigorous reading should weight them.
High heterogeneity. Banyard’s I² statistic was 90.1% for depression and 85.8% for anxiety,1 meaning most variation between studies reflects real underlying differences, not sampling error. The pooled SMD averages across studies that disagree substantively about how large the benefit is.
Risk of bias is high. 59% of trials in Banyard’s review were rated high risk of bias — participant blinding is impossible in exercise interventions, and outcome assessors were often unblinded too.1 Sample-size calculations were reported in only 28% of trials; 18 of 26 enrolled 50 or fewer participants.
Publication bias is detectable. Funnel plots show small flattering trials are over-represented. The gap between unadjusted and adjusted effect sizes in Schuch’s analysis is the cleanest direct evidence.3
Generalizability is narrower than headlines suggest. Banyard’s inclusion limited the population to adults aged 18–64.1 Severe depression with active suicidality, comorbid bipolar disorder, and psychotic-spectrum presentations are routinely excluded from exercise trials.
Exercise Recommendations for Depression and Anxiety
Exercise has essentially no medical downside for the vast majority of adults, and the upside on depression and anxiety symptoms is real and clinically meaningful. The calibration above is about the size and shape of the effect, not whether to do it.
- Do both aerobic and resistance training; if forced to choose, lean with the data. Aerobic has a slightly larger point-estimate effect for depression; resistance has a slightly larger one for anxiety and is the only type reaching within-subgroup significance for anxiety. Neither difference is formally confirmed, but the directional signal is real. Mixed protocols (aerobic + resistance) showed up in 6 of 32 trials and worked well — doing both probably captures the directional advantages of each.
- Pick what you’ll stick with. Consistency is the largest practical predictor of benefit. If a type of exercise feels like a chore, switch to one you actually enjoy — the best exercise for mental health is the one you keep doing.
- Sub-guideline volumes work. Only 3 of 30 studies in Banyard’s review met WHO weekly activity guidelines, yet meaningful clinical improvement was observed across the full set.1 Two short sessions a week is a defensible starting point, with no evidence that pushing to WHO targets adds proportionate benefit.
- Severity gates the role. For mild to moderate depression, exercise sits alongside (not after) medication and therapy. For severe depression — particularly with suicidality or psychotic features — exercise is an add-on to primary treatment, not a substitute.
- Make it specific. “I’ll exercise more” predicts almost nothing. “Tuesday and Thursday at 7am, 25 minutes” predicts a great deal. Specificity beats ambition.
Frequently Asked Questions
How much exercise do I need to see a benefit on mood?
Less than the 150 minutes per week of moderate aerobic activity recommended by the WHO. Only 3 of 30 trials in the most recent meta-analysis met WHO targets, yet clinical-grade improvement was observed across the full set.1 Prospective dose-response data on depression risk show the steepest gains at the lowest doses, with diminishing returns thereafter.11
Should I do cardio or resistance training?
Ideally both. Combined protocols showed up in 6 of 32 trials in the most recent meta-analysis and worked well. If forced to choose: aerobic leans modestly better for depression (SMD −1.60 vs −0.89), resistance leans modestly better for anxiety (SMD −0.83 vs −0.56, and resistance is the only type reaching within-subgroup significance for anxiety: Z = 2.79, p = 0.005, vs aerobic Z = 1.88, p = 0.090).1 Neither preference is formally confirmed (between-group p = 0.591 and 0.683), but the directional signal is real and worth using to set a starting point.
How quickly do mood effects from exercise appear?
Most trials show measurable symptom reduction by four weeks, with continued improvement through 12 to 16 weeks. Antidepressants generally show a slightly faster onset; exercise’s effect appears more durable after the formal trial period ends.7
Does exercise help severe depression?
The evidence base is dominated by mild and moderate cases. For severe major depression — particularly with suicidality, hospitalization, or psychotic features — exercise should be considered an add-on to evidence-based primary treatment, not a substitute.
What if I can’t exercise consistently?
Inconsistent activity still beats no activity in the available data. The trials with the lowest prescribed volumes still produced measurable benefit.1 Locking in a fixed time and place, with low initial volume and gradual scaling, predicts adherence better than ambition does.
References
- Banyard H, Edward K-L, Garvey L, Stephenson J, Azevedo L, Benson AC. The Effects of Aerobic and Resistance Exercise on Depression and Anxiety: Systematic Review With Meta-Analysis. International Journal of Mental Health Nursing. 2025;34:e70054. doi:10.1111/inm.70054
- Cooney GM, Dwan K, Greig CA, et al. Exercise for depression. Cochrane Database of Systematic Reviews. 2013;(9):CD004366. doi:10.1002/14651858.CD004366.pub6
- Schuch FB, Vancampfort D, Richards J, Rosenbaum S, Ward PB, Stubbs B. Exercise as a treatment for depression: A meta-analysis adjusting for publication bias. Journal of Psychiatric Research. 2016;77:42-51. doi:10.1016/j.jpsychires.2016.02.023
- Heissel A, Heinen D, Brokmeier LL, et al. Exercise as medicine for depressive symptoms? A systematic review and meta-analysis with meta-regression. British Journal of Sports Medicine. 2023;57(16):1049-1057. doi:10.1136/bjsports-2022-106195
- Gordon BR, McDowell CP, Hallgren M, Meyer JD, Lyons M, Herring MP. Association of Efficacy of Resistance Exercise Training With Depressive Symptoms: Meta-analysis and Meta-regression Analysis of Randomized Clinical Trials. JAMA Psychiatry. 2018;75(6):566-576. doi:10.1001/jamapsychiatry.2018.0572
- Blumenthal JA, Babyak MA, Doraiswamy PM, et al. Exercise and Pharmacotherapy in the Treatment of Major Depressive Disorder. Psychosomatic Medicine. 2007;69(7):587-596. doi:10.1097/PSY.0b013e318148c19a
- Babyak M, Blumenthal JA, Herman S, et al. Exercise Treatment for Major Depression: Maintenance of Therapeutic Benefit at 10 Months. Psychosomatic Medicine. 2000;62(5):633-638.
- Cipriani A, Furukawa TA, Salanti G, et al. Comparative efficacy and acceptability of 21 antidepressant drugs for the acute treatment of adults with major depressive disorder: a systematic review and network meta-analysis. The Lancet. 2018;391(10128):1357-1366. doi:10.1016/S0140-6736(17)32802-7
- Erickson KI, Voss MW, Prakash RS, et al. Exercise training increases size of hippocampus and improves memory. Proceedings of the National Academy of Sciences. 2011;108(7):3017-3022. doi:10.1073/pnas.1015950108
- Schuch FB, Stubbs B. The Role of Exercise in Preventing and Treating Depression. Current Sports Medicine Reports. 2019;18(8):299-304. doi:10.1249/JSR.0000000000000620
- Pearce M, Garcia L, Abbas A, et al. Association Between Physical Activity and Risk of Depression: A Systematic Review and Meta-analysis. JAMA Psychiatry. 2022;79(6):550-559. doi:10.1001/jamapsychiatry.2022.0609