
Adding music to ketamine psychotherapy failed to provide extra antidepressant benefit over matched non-music support in a 2026 randomized clinical trial (RCT; a study that assigns participants to groups by chance), even though the full 6-infusion ketamine-psychotherapy course was followed by large depression-score reductions.
Research Highlights
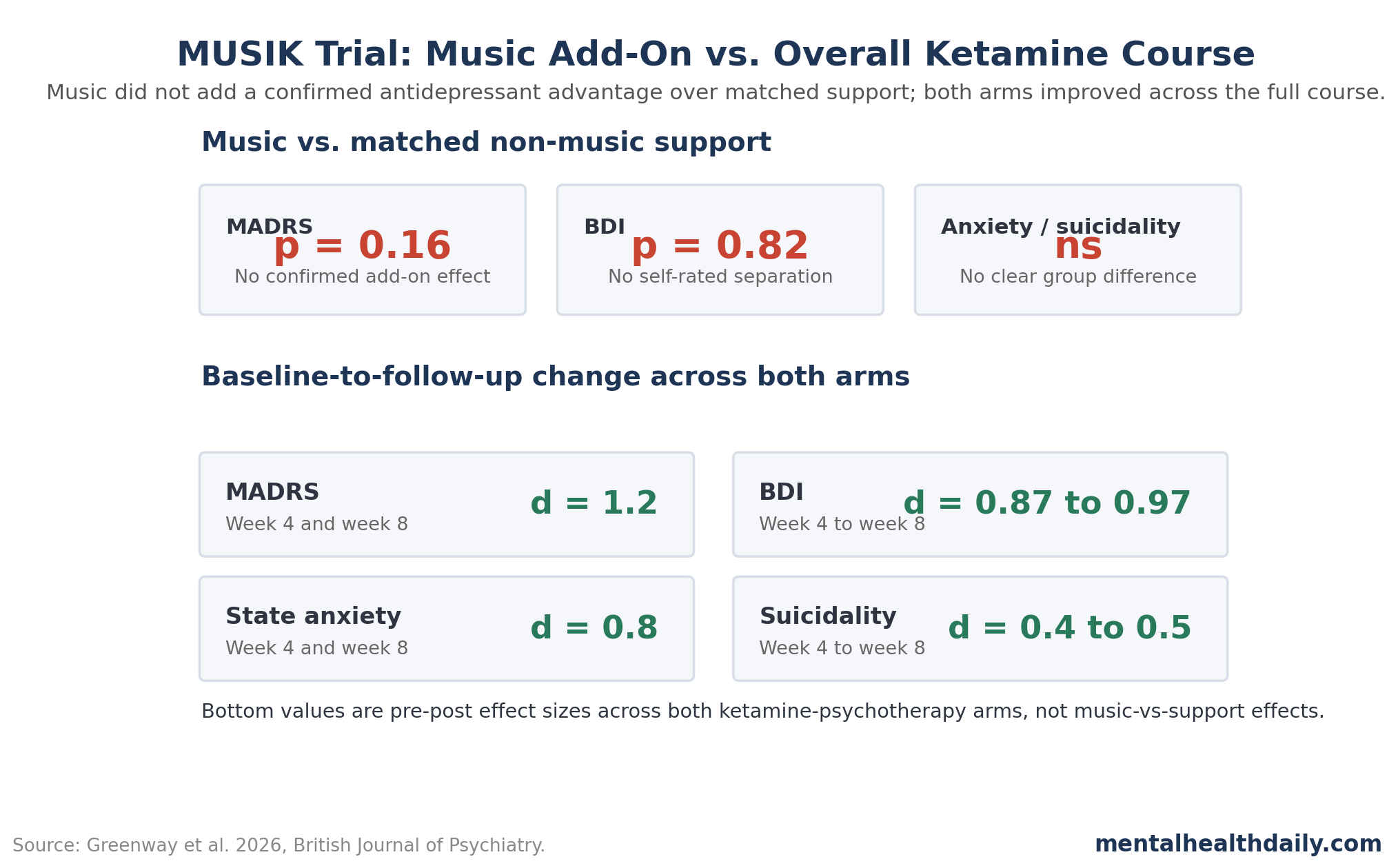
- Music added no confirmed MADRS benefit: in the MUSIK trial, the music and matched-support groups showed no significant difference in Montgomery-Asberg Depression Rating Scale (MADRS; a clinician-rated depression scale) change at 4 weeks, t(29) = −1.44, p = 0.16.1
- Depression scores fell substantially overall: across both groups, average MADRS scores decreased from 31.5 to 19.7 at 4 weeks, t(31) = −5.54, p < 0.001, d = 1.2, and the reduction was maintained at 8 weeks.
- The sample was clinically severe: 32 participants had a mean Dutch Measure for quantification of Treatment Resistance in Depression score of 16.7, 81% had a personality disorder, 78% had significant suicidal ideation, and 53% had a prior suicide attempt.
- Mystical-type experience tracked later improvement: higher-than-usual Mystical Experience Questionnaire scores predicted larger subsequent decreases in MADRS (β = −1.21, p = 0.015) and Beck Depression Inventory scores (β = −1.42, p = 0.004).
- Evidence strength is promising but limited: the 32-person randomized comparison tested music vs. matched support, while the broader ketamine-psychotherapy signal came from a small open-label treatment course without a ketamine-only or placebo-infusion arm.
Treatment-resistant depression (TRD; depression that persists despite adequate medication or therapy attempts) is a setting where ketamine can work quickly, but standard intravenous ketamine effects often fade after days or weeks. That durability problem has pushed researchers toward repeated dosing, psychotherapy, and treatment environments designed to shape the drug experience.23
Greenway et al. tested a specific version of that approach: 6 subanesthetic ketamine infusions over 4 weeks, embedded in psychological support, with music during the dosing sessions for 15 participants and matched non-music support for 17 participants.1 Subanesthetic means the dose was below the level used to produce surgical anesthesia; in this trial, participants received 0.5 mg/kg intravenous ketamine over 40 minutes.
Music Added No Clear Antidepressant Boost Over Matched Support
The study was built from the MUSIK trial, a 2-center, single-blind trial in Montreal that originally examined whether music improved ketamine hemodynamic tolerability. Hemodynamic tolerability refers to cardiovascular responses such as blood-pressure increases during infusion. The primary JAMA Network Open report found that music reduced the systolic blood-pressure rise during ketamine compared with non-music support.4
The 2026 British Journal of Psychiatry paper focused on depression, anxiety, suicidality, and psychedelic-like experience. The depression result was direct: music during ketamine added no statistically confirmed advantage over matched non-music support on the primary therapeutic outcome, MADRS change at 4 weeks, t(29) = −1.44, p = 0.16. Beck Depression Inventory (BDI; a self-report depression scale) change at 4 weeks also showed no group separation, t(21) = −0.23, p = 0.82.
That result calibrates the role of music. Kaelen et al. argued from psilocybin-session data that music can function as a “hidden therapist,” shaping emotion, imagery, and meaning during psychedelic treatment.5 The MUSIK data support a narrower antidepressant interpretation:
- Music may improve tolerability: the earlier MUSIK report found a smaller systolic blood-pressure rise during ketamine when music was used.4
- Music did not visibly increase depression response: MADRS and BDI changes were statistically similar under music and matched support.
- Music was tested against an active context: the control condition included supportive staff presence, encouragement to engage with the experience, and post-infusion discussion, so it was stronger than an ordinary silent infusion.
- Music may still help the treatment experience: music may improve comfort, blood-pressure tolerability, emotional engagement, or patient preference; this trial failed to show that it added measurable antidepressant reduction beyond matched support.
That control design is the likely reason music failed to add much. Both groups received ketamine in a supportive room, with psychological preparation, accompaniment, and integration. If the non-music condition already provided interpersonal support and permission to engage with the ketamine experience, music had less room to produce a separate antidepressant effect.
Depression, Anxiety, and Suicidality Improved Across the Full Course
The whole-group change was much larger than the between-group music comparison. Across all 32 participants, the researchers administered 181 of 194 planned ketamine infusions, a 94% delivered-dose rate. A total of 28 participants, or 88%, completed all visits per protocol.
At baseline, this was a heavily ill group:
- Depression severity: mean MADRS 31.5 and mean BDI 37.8, both consistent with severe depressive symptoms.
- Treatment resistance: mean Dutch Measure for quantification of Treatment Resistance in Depression score 16.7, with an average current episode duration of 5.9 years.
- Psychiatric comorbidity: 81% had a personality disorder, 63% had an anxiety disorder, 25% had posttraumatic stress disorder, and participants averaged 3.3 psychiatric diagnoses.
- Suicide risk: 78% had significant suicidal ideation and 53% had a prior suicide attempt.
- Prior intensive treatment: 22% had received electroconvulsive therapy during the current depressive episode.
Against that baseline, the 4-week symptom change was substantial. Mean MADRS decreased from 31.5 to 19.7, a decrease of 11.8 points, with t(31) = −5.54, p < 0.001, and d = 1.2.
Other 4-week outcomes: Cohen’s d is a standardized effect size; values around 0.8 are usually considered large, so d = 1.2 is large in statistical terms. The BDI also improved, t(31) = −4.57, p < 0.001, d = 0.87. State anxiety improved, t(31) = −3.92, p < 0.001, d = 0.8. Suicidal ideation improved more modestly, t(31) = −2.12, p = 0.04, d = 0.4.
At 8 weeks, the depression effects were maintained. The MADRS reduction stayed at about 11.7 points, t(28) = −5.20, p < 0.001, d = 1.2. BDI improvement remained large, t(31) = −4.72, p < 0.001, d = 0.97. Anxiety and suicidality also remained improved, although the researchers reported that the suicidality findings at both 4 and 8 weeks, plus anxiety at 8 weeks, lost significance after Bonferroni correction, a stricter adjustment for multiple tests.
Mystical-Type Experience Predicted Later Depression Change
The study also measured psychedelic-like experience during ketamine sessions. The Mystical Experience Questionnaire (MEQ; a scale measuring experiences such as unity, transcendence of time and space, positive mood, and ineffability) and the Emotional Breakthrough Inventory (EBI; a scale measuring release or confrontation of emotionally important material) were collected across the infusion course.67
Across 181 infusions, mean MEQ score was 66.6 with standard deviation (SD) 35.3, and mean EBI score was 35.7 with SD 18.4. Peak within-person scores averaged 88.7 for MEQ and 60.0 for EBI. Music and non-music groups showed similar experience scores, so the experience analysis was mostly about what happened across all ketamine sessions rather than about music as the active ingredient.
The strongest mechanistic result favored MEQ over EBI. In multilevel models, treatment number predicted larger depression reductions, as expected: each additional ketamine session was associated with lower later MADRS (β = −2.49, p < 0.001) and lower later BDI (β = −2.13, p < 0.001). Treatment number also predicted higher EBI scores (β = 3.17, p < 0.001), which complicated EBI interpretation because emotional breakthrough increased as treatment progressed.
After controlling for treatment number, higher-than-usual MEQ scores at one session predicted lower depression scores at the next session:
- MADRS: within-person MEQ at the prior timepoint predicted later MADRS decrease, β = −1.21, p = 0.015.
- BDI: within-person MEQ at the prior timepoint predicted later BDI decrease, β = −1.42, p = 0.004.
- Directionality check: prior depression scores failed to predict later MEQ scores, with p = 0.72 for MADRS and p = 0.43 for BDI.
Peak MEQ scores also correlated with week-4 depression improvement. Peak MEQ explained 35.6% of relative MADRS change variance and 48.9% of relative BDI change variance, both with p < 0.001. Average MEQ scores were also associated with MADRS and BDI improvement.
The EBI pattern was weaker. Peak EBI scores were unrelated to MADRS improvement, adjusted R2 = 0.061, p = 0.21, and unrelated to BDI improvement, adjusted R2 = 0.076, p = 0.16. Average EBI reached significance for BDI but only approached significance for MADRS. This suggests that the mystical-type component of ketamine experience was more consistently tied to later antidepressant change than emotional breakthrough in this small trial.
Ketamine Experience Is Different from Simple Dissociation
Ketamine is often described as a dissociative anesthetic. Dissociation means a feeling of detachment from body, self, time, surroundings, or ordinary perception. In psychiatry trials, dissociation is commonly measured with the Clinician-Administered Dissociative States Scale (CADSS). Ballard and Zarate reviewed the ketamine literature and concluded that dissociation measured this way has an inconsistent relationship with antidepressant benefit.8
The MUSIK trial points toward a more specific measurement problem. A patient can experience ketamine as disorienting, frightening, emotionally meaningful, spiritually charged, peaceful, or some mixture of these. Lumping the whole psychoactive state into “dissociation” may miss the parts that predict improvement.
A 2024 randomized trial by Aepfelbacher et al. found that awe during ketamine treatment mediated antidepressant effects, while dissociation did not mediate the same outcome.9 Awe and mystical-type experience are overlapping but distinct constructs. Both capture a positively valenced, meaning-rich state more directly than a generic dissociation score.
That measurement distinction has practical consequences. A clinic that merely tolerates ketamine’s psychoactive effects may produce a different psychological state than a clinic that prepares, supports, and helps patients integrate the experience. The MUSIK trial cannot isolate which component produced durability, but it gives a reason to measure the subjective state in more detail than “dissociated or not.”
Evidence Strength for Ketamine Psychotherapy in Resistant Depression
Evidence strength: moderate for the music-vs.-support comparison, preliminary for the broader ketamine-psychotherapy model. The randomization makes the music comparison valuable. Blinded MADRS raters reduce one important source of bias. The 181-infusion dataset also gives more repeated-measures information than a single-dose ketamine study.
The broader treatment interpretation is weaker. The trial had 32 participants, no ketamine-only group, no saline or active-placebo infusion group, and an open treatment context for participants and clinicians.
Bundled treatment context: psychological support, treatment room, clinician presence, repeated dosing, expectancy, and ketamine pharmacology all arrived together. The data can support a serious hypothesis that ketamine plus psychotherapy-like context produces more durable benefit than ordinary ketamine delivery, but that hypothesis needs head-to-head testing.
Adjacent literature keeps the result plausible. Garel et al. described the Montreal Model as an integrated biomedical-psychedelic approach to ketamine for severe TRD.3 A 2022 narrative systematic review found that ketamine-assisted psychotherapy studies were heterogeneous and early, with encouraging signals but no settled protocol.10
The current trial adds a more rigorous repeated-measures dataset, while still leaving the central clinical comparison unresolved: ketamine alone, ketamine plus standard monitoring, ketamine plus structured psychotherapy, or ketamine in a psychedelic-style support model.
Adverse-event reporting was reassuring but small. The researchers recorded no serious adverse events.
Discontinuations and urgent contacts: 1 participant in the non-music group dropped out after 4 treatments because of intolerable psychoactive effects, another non-music participant discontinued after 2 treatments because of a family issue, 2 music-group participants presented to the emergency room for increased suicidal ideation during treatment, and 1 music-group participant was withdrawn for driving within 24 hours of infusions. No participant was hospitalized.
Questions About Ketamine Psychotherapy and Music
Did music make ketamine more antidepressant in the MUSIK trial?
No significant depression advantage appeared for music over matched non-music support. MADRS change at 4 weeks had p = 0.16, and BDI change had p = 0.82.
Did the overall ketamine-psychotherapy course reduce depression?
Yes. Across both groups, MADRS scores fell by 11.8 points at 4 weeks and stayed down by 11.7 points at 8 weeks. The clinician-rated depression effect size was d = 1.2 at both timepoints.
Does this prove ketamine psychotherapy is better than ordinary ketamine infusions?
The trial supports that possibility, but proof would require a direct comparison against ordinary ketamine delivery. Every participant received ketamine with psychological support, so the study cannot separate ketamine pharmacology from the therapeutic context.
What should future ketamine trials measure?
Future trials should measure more than dissociation. Mystical-type experience, awe, emotional breakthrough, anxiety during dosing, perceived support, and integration quality may explain why the same ketamine dose produces different clinical trajectories.
References
- The Music for Subanesthetic Infusions of Ketamine Randomized Clinical Trial: Ketamine as a Psychedelic Treatment for Highly Refractory Depression. Greenway KT et al. British Journal of Psychiatry. 2026. doi:10.1192/bjp.2025.102
- Ketamine and Other Glutamate Receptor Modulators for Depression in Adults with Unipolar Major Depressive Disorder. Dean RL et al. Cochrane Database of Systematic Reviews. 2021;(9):CD011612. doi:10.1002/14651858.cd011612.pub3
- The Montreal Model: An Integrative Biomedical-Psychedelic Approach to Ketamine for Severe Treatment-Resistant Depression. Garel N et al. Frontiers in Psychiatry. 2023;14:1268832. doi:10.3389/fpsyt.2023.1268832
- Music as an Intervention to Improve the Hemodynamic Response of Ketamine in Depression: A Randomized Clinical Trial. Greenway KT et al. JAMA Network Open. 2024;7(1):e2354719. doi:10.1001/jamanetworkopen.2023.54719
- The Hidden Therapist: Evidence for a Central Role of Music in Psychedelic Therapy. Kaelen M et al. Psychopharmacology. 2018;235:505-519. doi:10.1007/s00213-017-4820-5
- Validation of the Revised Mystical Experience Questionnaire in Experimental Sessions with Psilocybin. Barrett FS et al. Journal of Psychopharmacology. 2015;29(11):1182-1190. doi:10.1177/0269881115609019
- Emotional Breakthrough and Psychedelics: Validation of the Emotional Breakthrough Inventory. Roseman L et al. Journal of Psychopharmacology. 2019;33(9):1076-1087. doi:10.1177/0269881119855974
- The Role of Dissociation in Ketamine’s Antidepressant Effects. Ballard ED et al. Nature Communications. 2020;11:6431. doi:10.1038/s41467-020-20190-4
- Experiences of Awe Mediate Ketamine’s Antidepressant Effects: Findings from a Randomized Controlled Trial in Treatment-Resistant Depression. Aepfelbacher J et al. Biological Psychiatry Global Open Science. 2024;4(3):100316. doi:10.1016/j.bpsgos.2024.100316
- Ketamine Assisted Psychotherapy: A Systematic Narrative Review of the Literature. Drozdz SJ et al. Journal of Pain Research. 2022;15:1691-1706. doi:10.2147/jpr.s360733