A 2026 resting-state fMRI study of 800 adults found intra-thalamic hypoconnectivity across schizophrenia, bipolar disorder, and major depression, but schizophrenia showed far broader subcortical dysconnectivity than bipolar disorder or depression.1 The calibrated read is that these diagnoses may share a thalamic vulnerability while diverging in striatal and limbic circuitry.
Research Highlights
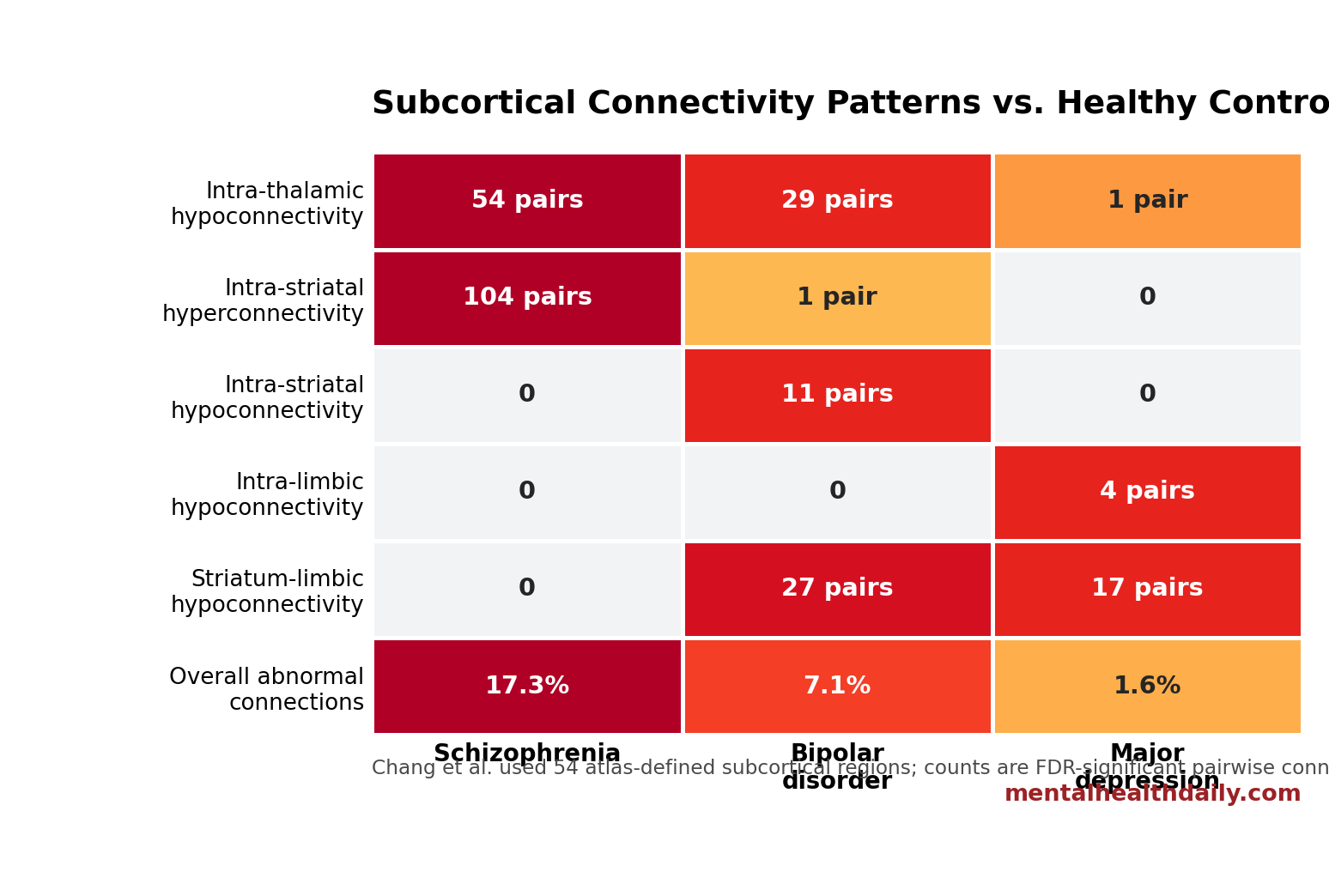
- Shared thalamic deficit: In 800 participants, decreased intra-thalamic connectivity appeared in 54 schizophrenia connections, 29 bipolar-disorder connections, and 1 major-depression connection after FDR correction.1
- Schizophrenia was broader: Abnormal subcortical connectivity affected 17.3% of tested connections in schizophrenia, compared with 7.1% in bipolar disorder and 1.6% in major depression.1
- Striatal direction separated diagnoses: Schizophrenia showed 104 increased intra-striatal connections, while bipolar disorder showed 11 decreased intra-striatal connections and major depression showed 0 intra-striatal hits.1
- Limbic findings leaned depressive: Major depression showed 4 decreased intra-limbic connections and 17 decreased striatum-limbic connections, including amygdala-putamen hypoconnectivity with peak t = -4.4.1
- Clinical use is not ready: The cross-sectional, mostly medicated cohort can map circuit patterns, but it cannot diagnose individuals or prove whether the 54-region connectivity differences cause symptoms.1
Subcortical connectivity means coordinated activity among deep brain structures such as the thalamus, striatum, amygdala, and hippocampus. These regions help gate sensory information, reward learning, action selection, memory, and emotion, so altered connectivity can plausibly affect psychosis, mood instability, and depression symptoms.
Chang et al. used resting-state functional magnetic resonance imaging (resting-state fMRI), which measures slow, spontaneous blood-oxygen-level fluctuations while a person is not doing a task. The researchers mapped pairwise connectivity among 54 subcortical regions, then compared schizophrenia, bipolar disorder, major depression, and healthy-control groups.1
800 Participants Were Split Into 4 Groups of 200
The study recruited 200 adults with schizophrenia, 200 with bipolar disorder, 200 with major depressive disorder, and 200 healthy controls from a single Taiwanese medical center. Diagnoses were based on clinical interviews and the Mini International Neuropsychiatric Interview Plus. The single-site design reduced scanner and protocol variation, but it also means the result still needs external replication.1
Participants with major depression were older on average and more often female than the other groups. Illness duration also differed: around 11 years for schizophrenia and bipolar disorder vs. around 7 years for major depression. Most patients were taking psychotropic medication, including antipsychotics in 89.5% of the schizophrenia group, 70.0% of the bipolar-disorder group, and 21.5% of the depression group.1
The atlas mattered: researchers divided each hemisphere into 8 thalamic regions, 12 striatal regions, and 7 hippocampal-amygdala regions. That produced 54 subcortical regions and 1,431 possible region-to-region connections per diagnostic comparison. Across 3 patient groups, the analysis involved 4,293 pairwise tests, corrected with a false-discovery-rate threshold of q < 0.05.1
Thalamic Hypoconnectivity Was the Shared Cross-Diagnostic Signal
The thalamus is a deep relay-and-gating structure that helps coordinate information flow between sensory systems, cortical networks, attention systems, and motor circuits. In this study, reduced connectivity within the thalamus was the most consistent cross-diagnostic abnormality.
Compared with healthy controls, schizophrenia showed 54 decreased intra-thalamic connections, bipolar disorder showed 29, and major depression showed 1. Prior work had already linked thalamocortical dysconnectivity to schizophrenia and bipolar illness, and a psychosis meta-analysis identified thalamic dysconnectivity as a recurring signal.2,4
Chang et al. sharpened that older pattern by looking inside the subcortical system itself. The result does not make thalamic hypoconnectivity a diagnostic test. It does make the thalamus a plausible shared vulnerability node across severe psychiatric disorders, especially where sensory gating, attention, and cognitive integration are impaired.
Schizophrenia Showed Widespread Thalamic-Striatal-Limbic Dysconnectivity
Schizophrenia had the broadest subcortical signature. Overall, 17.3% of tested subcortical connections differed from healthy controls, compared with 7.1% in bipolar disorder and 1.6% in major depression.1
The pattern had a different direction plus a larger burden. Schizophrenia combined intra-thalamic hypoconnectivity with intra-striatal hyperconnectivity and increased connectivity between the thalamus, striatum, and limbic regions. Table 2 listed 104 increased intra-striatal connections, 53 increased basal-ganglia-thalamus connections, 9 increased basal-ganglia-limbic connections, and 21 increased thalamus-limbic connections.1
Interpretation: schizophrenia looked less like one isolated deep-brain deficit and more like a distributed subcortical over-engagement pattern sitting on top of thalamic under-coordination. That fits earlier schizophrenia work showing thalamic dysconnectivity and striatal-network abnormalities, but it also warns against reducing the finding to a single dopamine story.3,6
Bipolar Disorder Had Intermediate Striatal and Striatum-Limbic Deficits
Bipolar disorder also showed intra-thalamic hypoconnectivity, but its striatal pattern diverged from schizophrenia. Instead of widespread intra-striatal hyperconnectivity, bipolar disorder showed 11 decreased intra-striatal connections and reduced connectivity between the thalamus and striatum, plus reduced connectivity between the striatum and limbic structures.1
The amygdala-putamen connection was a clear example. Bipolar disorder showed significant hypoconnectivity between the amygdala and putamen, with peak t = -4.17 and p < 0.0001. That matters mechanistically because the putamen is part of the striatum involved in action selection and habit learning, while the amygdala helps assign emotional salience to stimuli.
Prior bipolar neuroimaging reviews have emphasized reward and mood-regulation circuitry rather than a simple replication of schizophrenia connectivity. Chang et al. fit that view: bipolar disorder shared the thalamic deficit but sat between schizophrenia and major depression in overall dysconnectivity burden.7
Major Depression Looked More Limbic Than Striatal
Major depression showed the narrowest subcortical abnormality load in this cohort. Its most distinct within-subcortical finding was reduced connectivity inside the hippocampal-amygdala complex: 4 decreased intra-limbic connections, including left medial-to-lateral amygdala connectivity and left-right hippocampal connectivity.1
Between structures, major depression showed 17 decreased basal-ganglia-limbic connections and only 1 increased thalamus-limbic connection. Amygdala-putamen hypoconnectivity reached peak t = -4.4 with p < 0.00001. Earlier adolescent-depression and bipolar-vs.-unipolar studies also support the idea that amygdala connectivity can carry mood-disorder information.5,8
Clinical reading: depression involves cortical, endocrine, inflammatory, cognitive, sleep, and social systems too. Inside this 54-region subcortical atlas, the strongest depression-specific signal was limbic and striatum-limbic hypoconnectivity rather than widespread thalamic-striatal disruption.
Symptom Correlations Were Exploratory, Not Diagnostic
Exploratory symptom analyses linked some connectivity measures to severity, but the correlations were small. In schizophrenia, intra-striatal connectivity correlated with clinical severity at r = 0.14 and intra-thalamic connectivity at r = 0.17. In bipolar disorder, intra-striatal and intra-thalamic connectivity correlated negatively with psychotic symptom severity at r = -0.24 and r = -0.20. In major depression, intra-thalamic and intra-limbic connectivity correlated with depressive symptom severity at r = 0.22 and r = 0.20.1
Those values are not strong enough for individual-level classification. They are better treated as clues that subcortical circuitry may track symptom burden differently across diagnoses. A small but consistent brain-behavior correlation can still be useful for mechanism research, but it is not a clinical readout for one patient sitting in an exam room.
Limitations of This Subcortical Connectivity Study
Several design features keep the findings in a research lane.
- Cross-sectional design: the study cannot tell whether connectivity differences came before illness, emerged with illness progression, or followed treatment exposure.
- Medication exposure: most patients were medicated. Sensitivity analyses suggested core intra-subcortical abnormalities persisted in antipsychotic non-use subsamples, but medication effects cannot be fully removed.
- Depression-group differences: the major-depression group differed in age, sex distribution, and illness duration, leaving possible residual confounding even after covariate adjustment.
- Single-site sampling: one scanner and one protocol improve internal consistency, but multisite replication is needed before treating the pattern as a robust biomarker.
- No diagnosis engine: the study compared group averages. It did not build or validate a clinical classifier for schizophrenia, bipolar disorder, or depression.
The strongest conclusion is therefore circuit-level, not diagnostic. Thalamic hypoconnectivity crossed diagnoses, schizophrenia carried the broadest subcortical dysconnectivity burden, bipolar disorder showed an intermediate thalamic/striatal profile, and depression leaned toward limbic and striatum-limbic hypoconnectivity.
Questions About Subcortical Connectivity in Psychiatric Disorders
Does this mean schizophrenia, bipolar disorder, and depression share the same brain abnormality?
No. The shared feature was intra-thalamic hypoconnectivity. The broader pattern differed: schizophrenia showed widespread subcortical dysconnectivity, bipolar disorder showed intermediate thalamic and striatal abnormalities, and major depression showed a more focal limbic pattern.
Can subcortical fMRI diagnose these conditions?
No. This was a group-comparison study, not a validated diagnostic test. Individual diagnosis still depends on symptoms, course, impairment, differential diagnosis, and clinical context.
Why focus on the thalamus, striatum, amygdala, and hippocampus?
Those deep structures sit at the intersection of sensory gating, reward learning, emotional salience, action selection, and memory. Psychiatric symptoms are not generated by one region, but subcortical circuits can shape how cortical systems process information.
What would make this finding clinically stronger?
Replication in independent multisite cohorts, first-episode or unmedicated samples, longitudinal follow-up, and prediction of treatment response would move the finding closer to clinical use. The current study is best read as a mechanistic map.
How should the shared-thalamus finding change the interpretation?
The result argues against a single generic “psychiatric brain disorder” map. Shared thalamic dysfunction may exist, but striatal and limbic patterns still separate schizophrenia, bipolar disorder, and depression in ways that matter for mechanism research.
References
- Chang WC, Hung DP, Chen MH, et al. Distinct and common subcortical functional connectivity revealed across three major psychiatric disorders. Psychological Medicine. 2026;56:e137. doi:10.1017/s0033291726103377
- Anticevic A, Cole MW, Repovs G, et al. Characterizing thalamo-cortical disturbances in schizophrenia and bipolar illness. Cerebral Cortex. 2014;24(12):3116–3130. doi:10.1093/cercor/bht165
- Ferri J, Ford JM, Roach BJ, et al. Resting-state thalamic dysconnectivity in schizophrenia and relationships with symptoms. Psychological Medicine. 2018;48(15):2492–2499. doi:10.1017/s003329171800003x
- Ramsay IS. An activation likelihood estimate meta-analysis of thalamocortical dysconnectivity in psychosis. Biological Psychiatry: Cognitive Neuroscience and Neuroimaging. 2019;4(10):859–869. doi:10.1016/j.bpsc.2019.04.007
- Korgaonkar MS, Erlinger M, Breukelaar IA, et al. Amygdala activation and connectivity to emotional processing distinguishes asymptomatic patients with bipolar disorders and unipolar depression. Biological Psychiatry: Cognitive Neuroscience and Neuroimaging. 2019;4(4):361–370. doi:10.1016/j.bpsc.2018.08.012
- Li A, Zalesky A, Yue W, et al. A neuroimaging biomarker for striatal dysfunction in schizophrenia. Nature Medicine. 2020;26(4):558–565. doi:10.1038/s41591-020-0793-8
- Bi B, Che D, Bai Y. Neural network of bipolar disorder: toward integration of neuroimaging and neurocircuit-based treatment strategies. Translational Psychiatry. 2022;12:143. doi:10.1038/s41398-022-01917-x
- Cullen KR, Westlund MK, Klimes-Dougan B, et al. Abnormal amygdala resting-state functional connectivity in adolescent depression. JAMA Psychiatry. 2014;71(10):1138–1147. doi:10.1001/jamapsychiatry.2014.1087