A 2026 exploratory analysis of the ABCD cancer dyspnea trial found that higher baseline cytokines predicted less placebo symptom improvement than lower baseline cytokines across 33 of 40 cytokine-symptom combinations at day 7 and 29 of 40 at day 14.1 The signal is not ready for clinical prediction, but it sharpens a trial-design problem: patients with more inflammation may be less likely to improve on placebo, which can change how symptom trials are interpreted.
Research Highlights
- Placebo trends moved one way: higher baseline TNFα, IL-6, IL-8, and IL-10 pointed toward less placebo symptom improvement in 33 of 40 combinations at day 7 (p < 0.001) and 29 of 40 at day 14 (p = 0.006).1
- 5 symptoms showed day-7 signals: at least 1 cytokine significantly predicted less placebo response at higher baseline cytokine levels for pain, nausea, drowsiness, dyspnea, and appetite at day 7; 3 of 10 symptoms showed significant signals at day 14.1
- Dyspnea was the clearest example: placebo response was lower at higher baseline IL-6 than lower baseline IL-6 for dyspnea at day 7 (slope 0.51; p < 0.0001) and day 14 (slope 0.61; p < 0.0001).1
- Dexamethasone did not mirror placebo: the active-drug arm showed 14 of 40 positive slopes at day 7 (p = 0.08) and 12 of 40 at day 14 (p = 0.02), a different pattern from the placebo arm.1
- The evidence is exploratory: only 45 of 128 randomized trial participants had blood data, including 11 placebo patients, so the result is a hypothesis-generating biomarker signal rather than a clinical test.1
Placebo response means symptom improvement observed in the placebo group of a trial. It can include expectation, regression to the mean, attention from study staff, co-interventions, and real brain-body mechanisms triggered by treatment context.2
In cancer symptom trials, that response is not a nuisance detail. It can shrink the apparent difference between a drug and placebo, make an active intervention look weaker, or reveal that the measured symptom is highly sensitive to context and patient expectations.3
45 Cancer Patients Had Cytokines Measured During the ABCD Trial
The ABCD trial randomized patients with cancer-related dyspnea to dexamethasone or placebo. Dexamethasone is a corticosteroid used to reduce inflammation and sometimes relieve cancer-related symptoms such as breathlessness, appetite loss, nausea, or fatigue.
Hui et al. analyzed the subgroup with blood specimens. The sample was small but clinically concrete:
- Trial pool: 128 enrolled patients in the parent ABCD trial.
- Biomarker subgroup: 45 patients (35%) provided blood specimens.
- Randomized arms: 11 patients received placebo and 34 received dexamethasone.
- Measured immune markers: tumor necrosis factor (TNFα), interleukin-6 (IL-6), interleukin-8 (IL-8), and interleukin-10 (IL-10).
- Symptom scale: the Edmonton Symptom Assessment System (ESAS), an 11-point patient-reported scale covering pain, fatigue, nausea, depression, anxiety, drowsiness, dyspnea, appetite, sleep, and well-being.
Cytokines are immune-signaling proteins. TNFα, IL-6, and IL-8 are usually treated as inflammatory markers; IL-10 can act as inflammatory or anti-inflammatory depending on context.
ESAS symptom change runs in the opposite direction from ordinary “improvement” language. Higher ESAS scores mean worse symptoms, so a negative change from baseline means improvement. In Hui et al.’s models, a positive slope meant that higher baseline cytokines were associated with a smaller symptom decrease, or weaker response.
Higher Baseline Cytokines Pointed to Weaker Placebo Improvement
The main pattern was not one cytokine perfectly predicting one symptom. It was a repeated direction across many symptom-cytokine pairs.
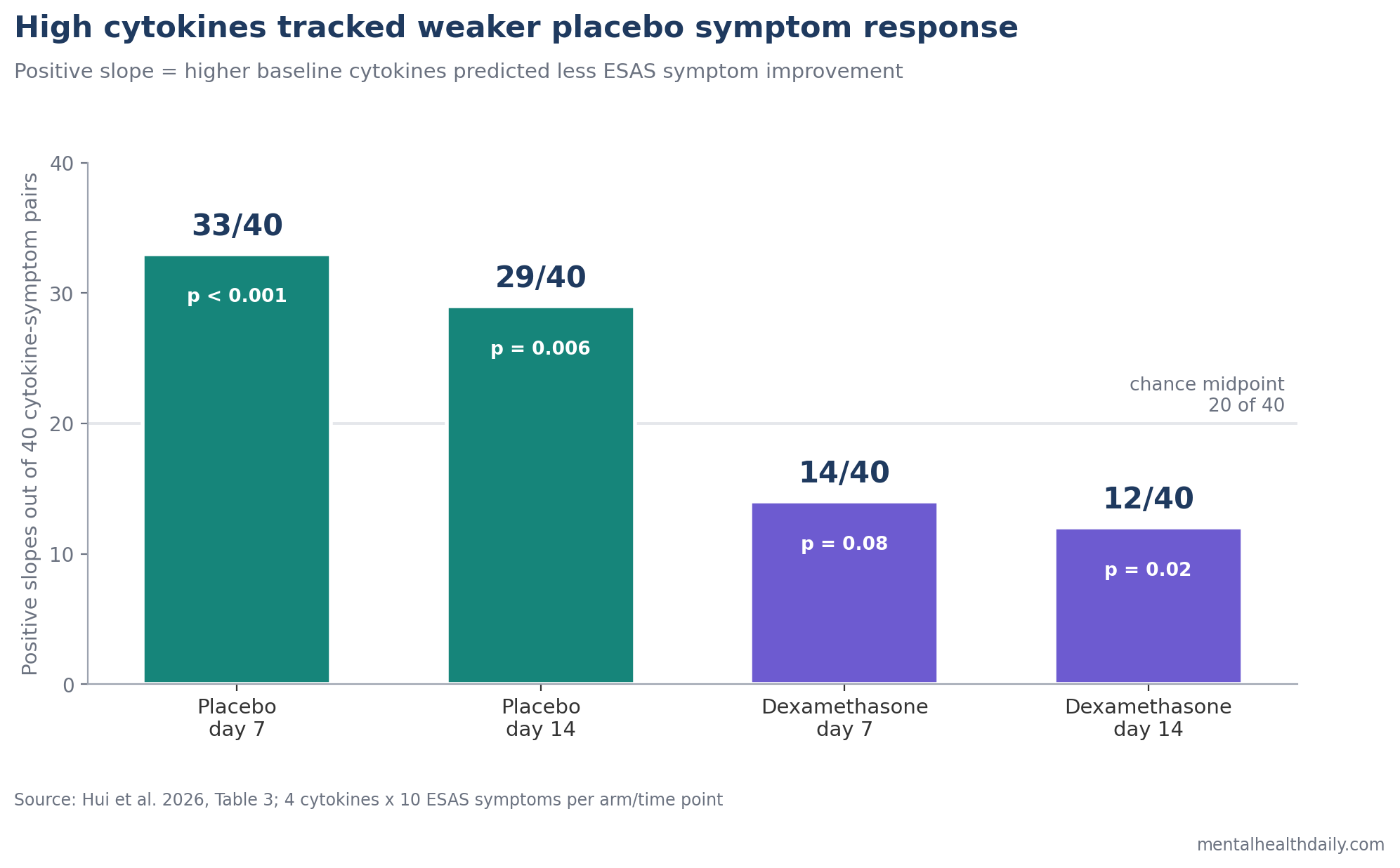
At day 7, placebo response showed positive slopes in 33 of 40 cytokine-symptom combinations. At day 14, the same direction appeared in 29 of 40. The binomial tests were significant at both time points, which is useful because individual symptom models were underpowered.
Significant placebo-arm associations appeared across multiple symptoms. Pain, nausea, drowsiness, dyspnea, and appetite had at least 1 significant cytokine association at day 7. Nausea, dyspnea, and appetite retained at least 1 significant placebo association at day 14.
Dyspnea anchored the pattern. Higher baseline IL-6 predicted weaker placebo dyspnea improvement at day 7 (slope 0.51; p < 0.0001) and day 14 (slope 0.61; p < 0.0001). TNFα, IL-8, and IL-10 also showed significant placebo-dyspnea associations at day 7, while TNFα and IL-8 remained significant at day 14.
Placebo Biology Has Prior Signals in Depression, IBS, and Cancer Fatigue
Hui et al.’s analysis sits inside a small but relevant biomarker-placebo literature. The adjacent studies do not prove the same mechanism, but they show why the inflammation-placebo question is plausible.
- Cancer fatigue trials: Roji et al. reviewed drug trials for cancer-related fatigue and found placebo response common enough to affect trial interpretation.3
- Depression and inflammation: Raison et al. tested infliximab, an anti-TNF drug, in treatment-resistant depression and showed that baseline inflammatory status could separate response patterns inside a placebo-controlled trial.4
- Irritable bowel syndrome: Kokkotou et al. reported serum correlates of placebo effect in IBS, a symptom condition where expectation and bodily sensation are tightly coupled.5
- Cancer fatigue genetics: Hoenemeyer et al. explored whether catechol-O-methyltransferase (COMT), a dopamine-metabolism gene, related to open-label placebo response for cancer-related fatigue.6
The common thread is not “placebo is fake.” It is that placebo response has measurable biological moderators in some settings, especially when outcomes are patient-reported symptoms such as pain, fatigue, dyspnea, depression, or gastrointestinal distress.
Inflammation Could Change Symptom Perception and Expectancy Pathways
Inflammation affects symptom circuits. Experimental immune activation can alter limbic, somatosensory, thalamocortical, dopamine, and serotonin pathways involved in pain, mood, dyspnea, fatigue, and bodily salience.7
Placebo effects also use brain circuits. Placebo analgesia and expectancy effects have been linked to changes in pain-related brain activity, context learning, valuation, and top-down modulation of sensory processing.2
That overlap gives the Hui finding a plausible mechanism: higher inflammatory tone may make symptoms less flexible in response to context, expectation, or supportive trial contact. A patient with lower inflammatory signaling may have more room for symptom perception to shift under placebo conditions.
The mechanism remains unsettled. The 2026 analysis did not measure brain activity, expectancy, clinician interaction quality, dopamine signaling, or serotonin signaling. It only showed that baseline cytokines repeatedly pointed in the direction of weaker placebo symptom improvement.
The Result Is Useful for Trial Design, Not Patient Selection Yet
For research, the most useful interpretation is trial calibration. If high-inflammation patients are less likely to show placebo response, cytokine profiles could eventually help trialists understand why a placebo arm improved less or more than expected.
Potential trial uses include:
- Stratification: balancing high- and low-inflammation patients across treatment arms before randomization.
- Responder modeling: testing whether baseline inflammation changes placebo response, active-drug response, or both.
- Endpoint interpretation: separating drug failure from a placebo arm that improved unusually strongly or weakly.
- Sample-size planning: estimating whether biomarker-defined subgroups need different trial sizes.
For clinical care, the result is much less actionable. No one should use TNFα, IL-6, IL-8, or IL-10 to decide whether an individual cancer patient is “placebo responsive.” The subgroup was too small, the models were exploratory, and the measured outcomes were secondary symptoms inside a dyspnea trial.
11 Placebo Patients Cannot Establish a Biomarker Test
Several limitations keep the finding in the hypothesis-generating lane.
- Small placebo arm: only 11 patients were randomized to placebo, and fewer had day-7 or day-14 symptom data.
- Post hoc analysis: the biomarker work used available blood specimens rather than a prospective placebo-biomarker design.
- Multiple testing: 4 cytokines, 10 symptoms, and 2 time points create many chances for false-positive findings.
- COVID-era specimen limits: pandemic restrictions reduced blood collection and contributed to missing data.
- Low baseline severity: several secondary symptoms started near the floor, which limits measurable improvement.
- Non-specific effects: regression to the mean, Hawthorne effects, expectancy, and co-interventions could still explain part of the placebo response.
Still, the directionality matters. A random noise pattern would not be expected to produce 33 of 40 placebo slopes in the same negative-response direction at day 7, then 29 of 40 at day 14. The right conclusion is calibrated: too preliminary for clinical use, too coherent to ignore in future placebo-controlled symptom trials.
Questions About Cytokines and Placebo Response
Does high inflammation mean placebo cannot work?
No. Hui et al. found a probabilistic pattern in a small trial subgroup, not an individual rule. Some patients with higher cytokines may still improve on placebo, and some patients with lower cytokines may not.
Why would placebo response involve the immune system?
Patient-reported symptoms are produced by brain-body systems. Inflammation can alter pain, fatigue, mood, breathlessness, and sensory salience; placebo effects can alter expectation, threat appraisal, and sensory processing. Cytokines may influence how much those systems can shift during a trial.
Did dexamethasone work better in high-cytokine patients?
The current analysis focused on symptom-response patterns in both arms, but its clearest claim was the placebo-arm direction. A prior ABCD biomarker analysis reported that higher baseline cytokines were linked to greater dyspnea reduction with dexamethasone and lower dyspnea reduction with placebo.8
Can cytokines be used to design better symptom trials?
Possibly, but not yet routinely. A larger prospective trial could pre-specify cytokine strata, measure expectancy and co-interventions, and test whether inflammation predicts placebo response after controlling for baseline symptom severity.
Is placebo response the same as “just imagination”?
No. Placebo response is measured symptom change in a placebo arm. It can include expectation, context, natural fluctuation, regression to the mean, and biological pathways. The point of biomarker work is to separate those mechanisms more carefully, not to dismiss symptoms.
References
- Predictive biomarkers of placebo response in patients with cancer: an exploratory analysis of the ABCD randomized clinical trial. Hui D et al. Supportive Care in Cancer. 2026;34:452. doi:10.1007/s00520-026-10689-9
- The neuroscience of placebo effects: connecting context, learning and health. Wager TD & Atlas LY. Nature Reviews Neuroscience. 2015;16(7):403-418. doi:10.1038/nrn3976
- Placebo response in trials of drug treatments for cancer-related fatigue: a systematic review, meta-analysis and meta-regression. Roji R et al. BMJ Supportive & Palliative Care. 2020;10:385-394. doi:10.1136/bmjspcare-2019-002163
- A randomized controlled trial of the tumor necrosis factor antagonist infliximab for treatment-resistant depression: the role of baseline inflammatory biomarkers. Raison CL et al. JAMA Psychiatry. 2013;70:31-41. doi:10.1001/2013.jamapsychiatry.4
- Serum correlates of the placebo effect in irritable bowel syndrome. Kokkotou E et al. Neurogastroenterology & Motility. 2010;22:285-e81. doi:10.1111/j.1365-2982.2009.01440.x
- An exploratory analysis of the association between catechol-O-methyltransferase and response to a randomized open-label placebo treatment for cancer-related fatigue. Hoenemeyer TW et al. Frontiers in Psychiatry. 2021;12:684556. doi:10.3389/fpsyt.2021.684556
- Cytokine targets in the brain: impact on neurotransmitters and neurocircuits. Miller AH et al. Depression and Anxiety. 2013;30:297-306. doi:10.1002/da.22084
- Predictive biomarkers of dyspnea response to dexamethasone and placebo in cancer patients. Hui D et al. Journal of Pain and Symptom Management. 2024. doi:10.1016/j.jpainsymman.2024.07.003